Posttraumatic stress disorder (PTSD) is a debilitating disease with limited available treatment options and for which novel effective interventions constitute a significant unmet need. This case report describes successful treatment of a patient with panic disorder and PTSD stemming from the 2010 Moscow subway terrorist attacks through the combination of script-driven trauma memory reactivation and inhalation of a xenon-based gas mixture. Xenon is a competitive inhibitor of N-methyl-d-aspartate receptors known to play a role in memory reconsolidation, a learning and memory process wherein memories temporarily enter a labile state after reactivation and may be modified. Literature describing current pharmacologic and exposure-based treatments is reviewed and provides the basis for use of this novel treatment strategy to target and modify emotional memories.
Combining Xenon Inhalation With Trauma Memory Reactivation to Reduce Symptoms of Posttraumatic Stress Disorder:
Case Report, Justification of Approach, and Review of the Literature
ABSTRACT
Posttraumatic stress disorder (PTSD) is a debilitating disease with limited available treatment options and for which novel effective interventions constitute a significant unmet need. This case report describes successful treatment of a patient with panic disorder and PTSD stemming from the 2010 Moscow subway terrorist attacks through the combination of script-driven trauma memory reactivation and inhalation of a xenon-based gas mixture. Xenon is a competitive inhibitor of N-methyl-d-aspartate receptors known to play a role in memory reconsolidation, a learning and memory process wherein memories temporarily enter a labile state after reactivation and may be modified. Literature describing current pharmacologic and exposure-based treatments is reviewed and provides the basis for use of this novel treatment strategy to target and modify emotional memories.
Prim Care Companion CNS Disord 2019;21(5):18nr02395
To cite: Dobrovolsky A, Bogin V, Meloni EG. Combining xenon inhalation with trauma memory reactivation to reduce symptoms of posttraumatic stress disorder: case report, justification of approach, and review of the literature. Prim Care Companion CNS Disord. 2019;21(5):18nr02395.
To share: https://doi.org/10.4088/PCC.18nr02395
© Copyright 2019 Physicians Postgraduate Press, Inc.
aPirogov Russian National Research Medical University, Moscow, Russia
bNobilis Therapeutics Inc, Portland, Oregon
cMcLean Hospital, Belmont, Massachusetts
*Corresponding author: Alexander Dobrovolsky, MD, PhD, Pirogov Russian National Research Medical University, Ostrovitianov str 1, Moscow, Russia 117997 ([email protected]).
Posttraumatic stress disorder (PTSD) is a debilitating psychiatric condition associated with tremendous emotional and financial costs to the health care system. It is estimated that approximately 7% of Americans will experience PTSD at one point in their lives, with significantly higher proportions of war veterans suffering from the disorder (approximately 12%–30%).1 Diagnosis of PTSD is based on exposure of the individual to a traumatic event and the manifestation of symptoms categorized into 4 clusters. The first, termed reexperiencing, involves the emotional and perceptual reliving of a traumatic event either spontaneously or in response to triggers that remind one of the event. The second symptom cluster, termed avoidance, involves avoidance of places and activities that are reminders of the event. The third cluster involves hypervigilance about one’s surroundings, sleep disturbance, anxiety, and lack of ability to maintain anger control, which sometimes leads to physical violence. In the DSM-5, a fourth cluster of symptoms has been added termed negative alterations in cognitions and mood. This cluster incorporates several symptoms previously included in the DSM-IV avoidance and numbing cluster with the addition of persistent distorted blame of self or others, persistent negative emotional state, the tendency to social isolation, and reduced ability to experience positive emotions in relationships with others based on empirical data on the phenomenology of the condition.2 A diagnosis of PTSD requires that symptoms must be present for over 1 month and create distress and functional impairment (eg, social, occupational).
A US government study3 conducted in 2008 estimated that PTSD in veterans of the Iraq and Afghanistan wars cost the American health care system 2.8 billion dollars annually. Patients with PTSD are reported to have a severely depressed quality of life,4 including deterioration of marital and family relationships,5 inability to maintain employment,6 exaggerated proclivity toward substance abuse, general medical illnesses such as increased risk of heart failure,7 suicidal tendencies and completed suicides,8 and early death.9 In addition, patients with PTSD are reported to have an increased incidence of clinical depression as a comorbidity.10
Currently, the main treatment interventions for PTSD include psychotropic medications or psychotherapy. Antidepressants are commonly prescribed.11 The selective serotonin reuptake inhibitor (SSRI) antidepressants sertraline and paroxetine are the only US Food and Drug Administration (FDA)–approved medications for the condition. Although positive effects were reported in the pivotal studies11–14 supporting the approval of sertraline, it is important to mention that these effects did not represent a major clinical improvement for PTSD sufferers. Two clinical studies15,16 that evaluated SSRIs in combat-related PTSD demonstrated no significant benefit. This finding, in part, is associated with recommendations against the use of SSRIs in the treatment of PTSD.17 The selective serotonin-norepinephrine reuptake inhibitor venlafaxine and the sympatholytic α-blocker prazosin have demonstrated some efficacy in open-label trials.18,19 Prazosin, however, was recently shown to be ineffective in achieving various efficacy endpoints of PTSD in a large randomized, placebo-controlled trial20 in veterans with chronic PTSD.
Other pharmacologic strategies, including second-generation antipsychotic augmentation of unsuccessful antidepressant therapy, as well as divalproex and bupropion, also appear to be ineffective or to show very limited benefit in patients with PTSD. Use of benzodiazepines, while widely used in clinical settings, has no supporting evidence and is described as ineffective and potentially harmful in the recent Department of Veterans Affairs/Department of Defense Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder21and were further shown to decrease the efficacy of exposure therapy for combat-related PTSD.22 According to the same guidelines,21 use of exposure therapy is one of the recommended treatments.
CASE PRESENTATION
The patient was a 32-year-old woman, a talented apparel designer, who was referred by a neurologist with a preliminary diagnosis of panic disorder (episodic paroxysmal anxiety, ICD-10-CM code F41.0). The patient’s complaints were summarized as episodes of shortness of breath, palpitations, a feeling of tension in the neck and head, and dizziness, accompanied by fear of losing consciousness and death. She also complained of insomnia.
History of Illness
The panic attacks first occurred in the fall of 2010. While obtaining a history from the patient, it was discovered that around 10:00 am on March 29, 2010, she witnessed the consequences of the terrorist attack that had just occurred in the Moscow subway. The patient recalled when an elderly woman entered the subway car in which she was riding and reported 2 explosions at neighboring stations. At the next stop, people entered the car with signs of injuries. She stated, “Their clothes were covered in blood, they were agitated, some were crying, some were wondering about possible new explosions.” Most of the passengers started calling mobile phones, everyone was discussing the incident, and often the words nightmare and horror were used. The patient remembered getting off the subway and heading for the exit, surrounded by a crowd of worried passengers and feeling scared. She went to work on foot, which should have been a 5-minute trip, but she got to the office by 2:00 pm with no recollection of how she got there. The patient’s supervisor initially reprimanded her for being late; she had difficulty answering questions, was confused and pale, and finally began to cry. The next day, she realized that due to her anxiety she could no longer get to work by subway or other means of public transportation. She was allowed to work from home and married in the summer, but gradually her symptoms intensified due to growing alarm and constant thoughts about the experienced event, and she had to quit her job in the early fall of 2010. Since the incident, the patient had not used the subway and avoided passing by its entrances. Once passing by such an entrance, she experienced the specific smell of the subway and heard the noise of the passing train, which triggered memories of the incident and provoked a flashback that manifested as reliving the event and seeing the face of the elderly woman who had informed the passengers of the explosions.
Eight years later, at the time of assessment, the patient still vividly remembered the face of the elderly woman who reported the terrorist attack, people with injuries, blood-soaked clothes, and an endless stream of people wanting to leave the subway. These memories were unprovoked and obsessive, forcing her to stop what she was doing at the time, often with the sensation of impending doom and death. It took her, on average, at least 30 minutes to calm down, and the residual somatic symptoms such as sweating and tachycardia often lasted several hours. Within the last 12 months, 4 attacks were so severe that her husband had to call an ambulance, and each time the emergency department staff diagnosed these episodes as panic attacks. At her husband’s insistence, she saw a neurologist and was started on a daily SSRI and a benzodiazepine as needed for panic attacks. Prescribed therapy did not decrease the frequency of the attacks but reduced the severity of the somatic component. When the frequency and severity of the attacks increased, the patient started taking benzodiazepines more frequently.
The patient never returned to full-time work, significantly decreased contacts with friends and relatives, and began to help her husband with his work, essentially becoming his assistant. Sometimes she performed freelance work from home, which usually consisted of requests from friends and acquaintances, as she was afraid to take on new clients because she felt that her condition could worsen at any time.
Clinical Assessment
The patient was a young woman who looked her stated age. She was oriented to place, time, and self. Her height was 5 ft 31/2 in (161 cm), her weight was 115 lb (52 kg), and her blood pressure and heart rate were within normal limits. She was neatly dressed, moving somewhat rigidly; her speech was literate, soft, and slow, with normal prosody and modulations. She answered the questions completely. No alterations in thought process or stupefaction were noted.
During the interview, when asked to talk about the incident in the subway, the patient’s mood changed drastically. Her voice became quieter, and it was obvious that she was fighting tears. Blotchy red spots appeared on her neck and chest; she clasped her hands around her waist as if trying to warm herself and described pronounced discomfort similar to what she experienced before the panic attacks. The interviewer redirected the line of questions, and the focus of the conversation changed to current affairs and her warm and supportive relationship with her husband. After 15 minutes, she reported a reduction in unpleasant symptoms.
Given the patient’s history of a traumatic event and persuasive clinical findings, the diagnosis of PTSD was strongly suspected. The PTSD Checklist for DSM-5 (PCL-5)23 was administered, which supported the diagnosis of PTSD. Psychiatric comorbidity was assessed with the Mini-International Neuropsychiatric Interview24 and was negative. As a desensitizing therapy, the method of fear memory reconsolidation blockade through script-driven memory reactivation and subsequent inhalation of subanesthetic doses of xenon, which had been successfully used in our clinic, was proposed. After providing informed consent and receiving relevant instructions, the patient wrote down her recollection of the traumatic event, which was 11/2 pages long.
Xenon Administration
Therapy was started on November 7, 2018, with a total of 8 sessions, and each included the patient reading the script record of the event followed immediately by inhalation of the xenon-oxygen mixture. At the beginning of each visit, the PCL-5 was administered.
Administration of xenon was performed through inhalation of xenon-oxygen mixtures ranging from 15%/85% to 25%/75%. The selected dosing regimen and the composition of the gas mixtures were based on the historical evidence of safety of subanesthetic use of xenon in imaging.25 Medical-grade xenon (Medksenon, 99.9999%, Atommedcenter, Moscow, Russia) and medical-grade oxygen in separate containers were admixed. Mixing and administration of gases in preset concentration and volume were accomplished with the use of the MAGi-AMTS1 (Atommedcenter, Moscow, Russia), which enables the operator to adjust the concentration of xenon in the gas mixture and contains the electronic flowmeter with a software module that allows for such adjustments. The xenon-oxygen mixture was administered via a face mask. The patient was asked to slowly inhale, holding her breath for 5–10 seconds, and exhale into the loop. After 35–40 seconds, she exhaled outside the contour and breathed in the new portion of gas mixture. Xenon inhalation lasted from 3 to 4 minutes, and the xenon consumption was capped at 3.0 L per procedure.
The patient’s blood pressure, heart rate, and oxygen saturation were measured before, during, and 20 minutes after each session. Table 1 describes the treatments. The patient tolerated xenon inhalations well with no side effects, such as euphoria, lightheadedness, headache, nausea, or vomiting, during or after the procedure. Table 2 presents the results of the PCL-5, which was administered on day 1, at the completion of the study (day 33), and a month later (day 58).
Outcomes
At the fourth visit before the introduction of the script-driven memory reactivation, the patient reported that she was able to recall the entire subway trip the day of the attack, the name of the subway station where she first heard about the explosion, the route with a transfer on her way to work that day, and some details of the events that took place after she arrived at work. Between the third and fourth treatment sessions, the patient reported a week-long period of increased irritability, which she subsequently described as an increasing influx of emotions that she was unaccustomed to and somewhat scared of. After the fourth and fifth sessions, the patient, without informing the physician, went into the vestibules of different subway stations and spent 15–20 minutes there. She described moderate discomfort without an influx of memories or the occurrence of a panic attack. According to a preliminary agreement with the physician, 2 weeks after the eighth session, she and her husband rode the subway through several stations each way. The agreement included the possibility of carrying out another xenon inhalation after the trip. At the office visit that took place within 30 minutes of her subway ride, the patient appeared a little excited from the idea of the trip itself but quickly calmed down and declined the xenon procedure, believing that she had coped with the task successfully. She was seen a month later and stated that she had started drawing again, feeling that she missed not only her favorite occupation, but also this important part of her life before the traumatic event, and that she now drew a lot and with pleasure. She resumed reading fiction. She became interested in getting up to speed with her professional field. Her circle of activities had noticeably expanded, and she started socializing with her husband and going out with friends, which she had not done for many years.
Exposure Therapy
One effective treatment approach, exposure therapy, originates from the hypothesis that PTSD is a disorder of emotional learning.26 Specifically, in exposure therapy the goal is to relive a traumatic event within a safe context to alter the emotional manifestations associated with the event. Since PTSD is the only psychiatric disorder that requires the occurrence of an external event as a prerequisite to diagnosis, this event provides the context for learning. It is known that across species, pairing a neutral stimulus with an aversive one leads to the learning of a conditioned fear response. In humans with PTSD, the matrix of sensory stimuli embedded in the traumatic memory serves as a cue that evokes a conditioned fear response in the absence of the original trauma (the unconditioned aversive stimuli). This conditioned fear response manifests as avoidance of trauma-associated cues, including thoughts, feelings, or sensory (eg, olfactory) reminders and the experience of emotional distress when faced with these reminders. A conditioned fear response can be initially adaptive, but it should extinguish when the conditioned cues are no longer accompanied by actual risk of danger. Individuals with PTSD have not learned that the stimuli associated with their trauma no longer signals danger. Thus, PTSD may manifest with a persisting conditioned fear response independent of the original trauma and difficulty learning that stimuli previously associated with a trauma should not lead to a fear response.27 Through exposure therapy, the clinician attempts to correct the negative associations in PTSD and accelerate extinction of the associated emotional memory.
Animal and human research demonstrates that fear is extinguished experimentally by repeatedly presenting the conditioned stimulus in the absence of the aversive stimulus, a process that has been associated with amygdala depotentiation.28 In humans, this model translates into repeatedly re-experiencing the traumatic memory in a safe environment (absence of the aversive stimuli) until the fear is extinguished. This process is hypothesized to be part of the mechanism of action in exposure therapy, the treatment with the strongest empirical evidence for PTSD.29 According to a 2008 Institute of Medicine report,30 exposure therapy was the only intervention with sufficient evidence to conclude efficacy in the treatment of PTSD. Although exposure therapy has been shown to be efficacious for the treatment of PTSD, a recent randomized clinical study31 in 370 military personnel with PTSD showed relatively modest reductions in PTSD symptom severity.
Memory Lability During Reconsolidation
The mental re-experience of the traumatic event is critical to the maintenance of posttraumatic symptoms over time. Animal and clinical research of memory consolidation has demonstrated that new memories are maintained in short-term memory until they are transferred at the cellular level into long-term storage.32 This consolidation is necessary for the development of stable long-term memory of a traumatic event. When reactivated, the memory can again become labile, allowing for updating of new information before it is reconsolidated to long-term memory for more permanent storage.33 This lability of memory during reconsolidation offers a very important window during which the long-term traumatic memories can be influenced. Thus, reconsolidation is an important mechanism for updating or modifying memories in which it may be possible to intervene. While exposure therapy alone has some success clinically,34 preclinical research has shown the feasibility of degrading the persistence of a fear memory by interfering with the cellular mechanisms associated with memory reconsolidation.35 Unfortunately, the chemical agents that have demonstrated efficacy in preclinical models are generally protein synthesis inhibitors (eg, anisomycin), which are not clinically feasible.
Augmentation of Exposure Therapy
One of the important aspects of exposure therapy is the mechanism by which during retrieval the memory becomes sensitive to manipulation before reconsolidation. If manipulation is induced during the reconsolidation phase, but prior to the full extinction process, the memory may be lost or its emotional significance may be altered. The experimental manipulation of memory reconsolidation was resurrected after a 30-year hiatus36 by Nader and colleagues,37 who described the disruption of Pavlovian fear memories by anisomycin administered after memory retrieval. The principle of reconsolidation manipulation is based on the findings that “new” memories are initially labile and sensitive to disruption before being consolidated into stable long-term memories. The process of memory reconsolidation appears to involve new protein synthesis, particularly in the areas of the brain known as the lateral and basal nuclei of the amygdala that are believed to be a site of memory storage in fear learning. This process was demonstrated previously by experiments in which injections of the protein synthesis inhibitor anisomycin into the lateral and basal nuclei of the amygdala shortly after training prevented consolidation of fear memories.38,39
The experiments by Nader et al37 showed that consolidated fear memories, when reactivated during retrieval, return to a labile state in which infusion of anisomycin shortly after memory reactivation produces amnesia on later tests regardless of whether reactivation was performed 1 or 14 days after conditioning. However, in the absence of memory reactivation, treatment with anisomycin left memory intact. Consistent with a time-limited role for protein synthesis in consolidation, delay of the infusion until 6 hours after memory reactivation produced no amnesia. These data showed that consolidated fear memories, when briefly reactivated, return to a labile state that requires de novo protein synthesis for reconsolidation. This study37 demonstrated first that consolidated memories could be “erased” after retrieval and second that mechanistically this so-called reconsolidation process resembled the original consolidation in its requirement for protein synthesis.
Although use of protein synthesis inhibitors is not clinically useful in humans for reconsolidation blockade, various pharmacotherapeutics are being developed for augmentation of the extinction learning process that may occur during exposure therapy. For instance, D-cycloserine (DCS) is a partial agonist at the N-methyl-d-aspartate (NMDA) receptor, a member of the glutamate receptor family, which has an essential role in mediating learning and memory. Both fear learning and extinction are blocked by antagonists at the glutamatergic NMDA receptor, whereas enhancement of NMDA function is thought to enhance both consolidation/reconsolidation and extinction.
The importance of the NMDA system in extinction is suggested by numerous studies.40–43 In 1 experimental study, Zimmerman and Maren44 assessed the role of NMDA receptors in the central nucleus of the amygdala (CEA), which is known to be involved in the acquisition of conditioned fear, but it is unknown whether it plays a role in fear extinction. Infusion of glutamate receptor antagonists into the basolateral complex of the amygdala (BLA) or CEA prior to the extinction of fear to an auditory conditioned stimulus (CS) in rats was performed. Infusion of the α-amino-3-hydroxyl-5-methyl-4-isoxazole-propionate (AMPA) receptor antagonist 2,3-dihydroxy-6-nitro-7-sulfamoyl-benzo[f]quinoxaline-2,3-dione into either the CEA or BLA impaired the expression of conditioned freezing to the auditory CS but did not impair the formation of a long-term extinction memory to that CS. In contrast, infusion of the NMDA receptor antagonist D,L-2-amino-5-phosphonopentanoic acid (APV) into the amygdala spared the expression of fear to the CS during extinction training but impaired the acquisition of a long-term extinction memory. Importantly, only APV infusions into the BLA impaired extinction memory. These results reveal that AMPA and NMDA receptors within the amygdala make dissociable contributions to the expression and extinction of conditioned fear, respectively.44
The role of NMDA receptors is central in modulation of fear memories in conditions such as panic disorder and PTSD. In a recent article,45 NMDA receptor antagonists were identified as the most promising target for novel pharmacotherapies to treat PTSD. The data were generated from a survey of 45 PTSD investigators from around the world who were asked to rank the top 5 potential new therapeutic targets for PTSD.45 Furini et al46 reviewed the history of fear extinction research and efforts to determine the mechanisms involved. The authors46 summarized that fear extinction is initiated and maintained by interactions between the hippocampus, basolateral amygdala, and ventromedial prefrontal cortex, which involves feedback regulation of the latter by the other 2 areas. Fear extinction depends on NMDA receptor activation. It is positively modulated by d-serine acting on the glycine site of NMDA receptors.
Pharmacologic manipulation of extinction has been successfully performed in rodent models. For example, Ledgerwood et al47 established a system wherein rats received 5 light-shock pairings as conditioning. The following day, rats received 6 light-alone presentations to induce extinction. Twenty-four hours later, rats received 1 light-alone presentation (test). Subcutaneous DCS injection before or after extinction training significantly enhanced extinction; the dose-response curve for this effect was linear. An increase in the delay of DCS administration after extinction training led to a linear decrease in the facilitatory effect. The effect of systemic administration was replicated by intrabasolateral amygdala infusion. These results suggest that DCS facilitates extinction of conditioned freezing by acting on consolidation processes partly mediated by the basolateral amygdala.47
Xenon
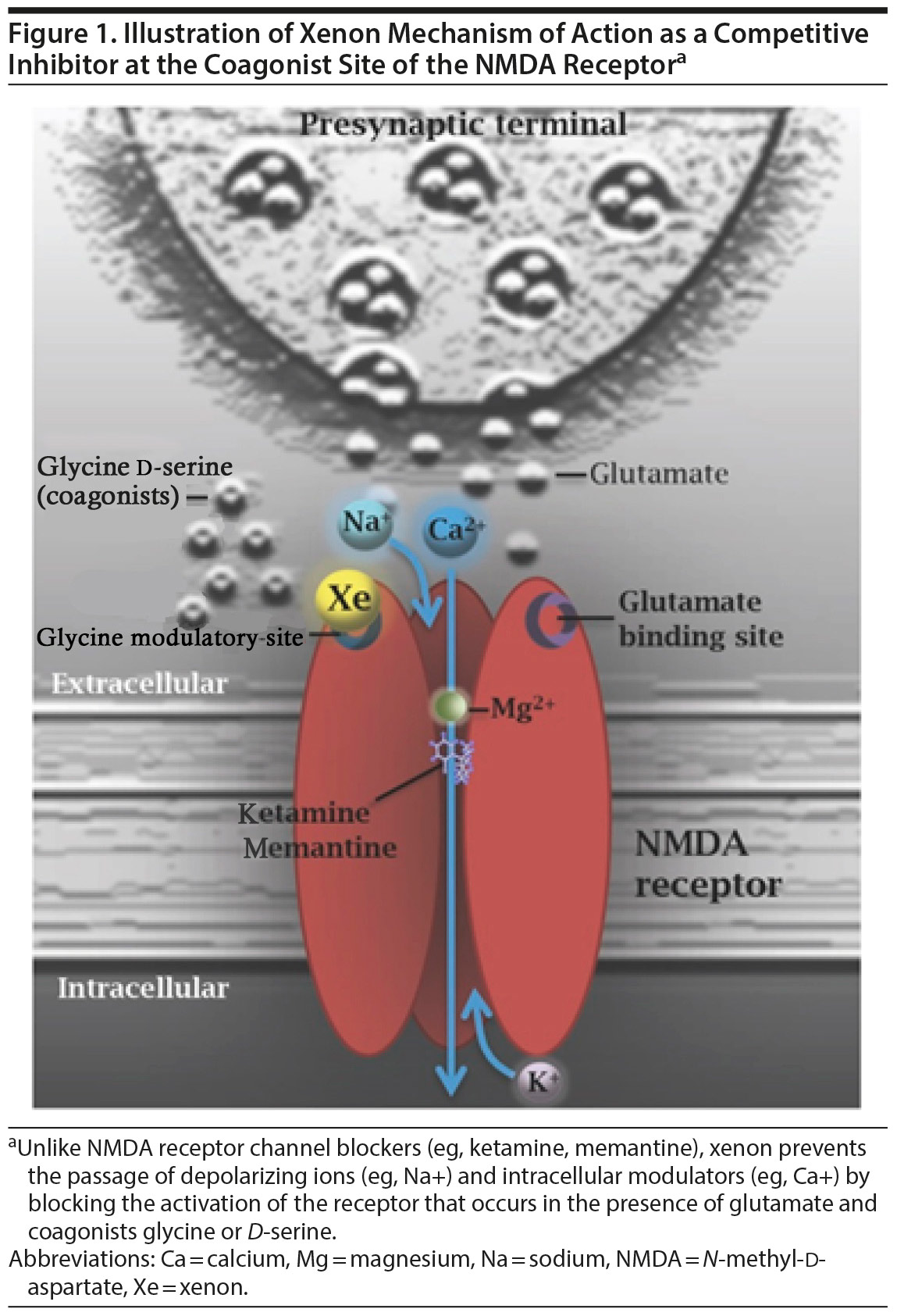
Xenon is a noble gas that was first discovered in 1898 by British chemists Sir William Ramsay and Morris W. Trave as a result of repeated fractional distillation of the noble gas krypton. It is an extremely rare element in the atmosphere, comprising approximately 0.05 ppm in air. Xenon is a competitive inhibitor of the NMDA receptor through blockade of the glycine coagonist site (Figure 1), thus reducing glutamate neurotransmission and inhibiting neuronal excitation. Xenon also blocks excitotoxicity produced by excess glutamate (such as occurs after neuronal insult) and the deleterious effects of excessive influx of calcium ions, which results in neuroprotection.48 In addition, xenon reduces excitatory neurotransmission through downregulation of 5-HT3,49 nicotinic acetylcholine,50 and AMPA receptors51 as well as potassium52 and hyperpolarization-activated cyclic nucleotide-gated channels.53 It also facilitates inhibitory neurotransmission by upregulating glycine receptors50 and activating TREK1 channels.54 Xenon has been shown to inhibit neuroinflammation in animal models of stroke and ischemia/reperfusion,55,56 has proven clinical safety and efficacy in reperfusion of neonatal ischemia,57 and has been demonstrated to inhibit NF-κ B, TNF-α, and proinflammatory cytokines.58 The medical use of the inert gas xenon for the induction of anesthesia was first reported in 1951 in the journal Science.59 Subsequently, the unique properties of xenon, which include (1) rapid on-off kinetics, (2) lack of metabolites and excretion only through the lungs, and (3) ability to inhibit glutamatergic signaling and excitotoxicity, led to numerous scientific investigations of these preclinical and clinical data.
We conducted an open-label clinical trial60 to determine the safety and efficacy of subanesthetic concentrations of xenon gas in the treatment of patients with panic disorder. Patients with panic disorder alone (N = 42) or panic disorder with other comorbidities (N = 39) received 6 to 7 treatment sessions wherein they inhaled increasing concentrations of xenon up to 30%. The study60 demonstrated that xenon is a potentially effective modality in acute treatment of panic disorder; the antipanic effect of xenon administration persisted for at least 6 months, and xenon was well tolerated.
Xenon Inhalation Therapy for Blockade
of Trauma Memory Reconsolidation
In the previously described study,47 DCS (acting as an NMDA receptor partial agonist) was used to explicitly enhance the extinction learning process. Of note, while a number of early extinction-augmentation clinical trials61,62 were positive with DCS, more recent studies63 have been mixed or negative. One explanation for these more recent treatment failures is that if the fear memory was not extinguished during brief exposure therapy, the process of memory reconsolidation would prevail over memory extinction (which requires a more robust and longer duration and consistent reactivation). As a partial agonist, DCS would be predicted to enhance the reconsolidation (as meaningful extinction learning could not be achieved) instead of blocking it, resulting in an apparent treatment failure. This treatment failure may be especially true in cases in which DCS was administered before reactivation of the trauma memory. In contrast, if good extinction learning was achieved, DCS would be predicted to enhance extinction over reconsolidation. Hence, the blocking of memory reconsolidation with a short-acting NMDA antagonist such as xenon, which can be given in a temporally dependent manner, may be a more practical, robust, and feasible way to modulate PTSD memories than the enhancement of extinction with NMDA partial agonists such as DCS.
Xenon may have distinct advantages over other NMDA antagonists, such as ketamine, for future translation to the clinical setting. First, subsedative concentrations of xenon that would sufficiently block the NMDA receptor without producing full anesthesia could potentially be administered briefly in a safe and effective manner in the outpatient setting with minimal or no medical monitoring. Second, in contrast to existing NMDA receptor channel blockers like ketamine (Figure 1), xenon has been shown to inhibit NMDA receptor activity through competitive inhibition of the coagonist glycine at the glycine site of the NMDA receptor64—an action that does not induce psychotomimetic effects. Given these unique characteristics, preliminary investigation into the safety and efficacy of administration of brief subsedative xenon concentrations as a pharmacologic intervention to treat PTSD is warranted.
While xenon has yet to be approved as an anesthetic agent in the United States, there is extensive clinical experience using subsedative concentrations of xenon as a contrast agent in xenon-enhanced computed tomography (Xe-CT). The safety of xenon diagnostic drug products has been evaluated in 2 large-scale studies.65,66 Latchaw et al65 conducted a large multicenter trial to assess safety in 1,830 patients who underwent CT cerebral blood flow (CBF) examinations. The dose included 32% Xe-CT for a period of 4.3 minutes. In this analysis, the most common adverse event was respiratory irregularity (defined as a pause > 10 seconds) in 3.6% of patients. None of these events were prolonged or serious. Other less-frequent events included headache (0.4%), seizures (0.2%), nausea and vomiting (0.2%), and change in neurologic status (0.1%).65
Another multicenter study published by Carlson and colleagues66 was conducted in over 2,000 patients with a variety of neurologic disorders, including stroke, occlusive vascular disease, traumatic brain injury, subarachnoid hemorrhage, aneurysms, tumors, and epilepsy. This large study66 was conducted under an FDA investigational new drug application with data (including adverse events) presumably collected in accordance with Good Clinical Practice guidelines. Dosing was administered at a concentration of 28% Xe-CT and inhaled over a period of 4.3 minutes. Results demonstrated a very low risk of adverse events and no risk of permanent morbidity or sequelae from xenon inhalation. Overall, respiratory adverse events were the most common, with 5.9% of patients experiencing minimal respiratory suppression (10–19 seconds), 1.9% of patients experiencing prolonged respiratory suppression (> 20 seconds), and 1.7% experiencing hyperventilation. Notably, none of these adverse events resulted in any consequence to any patient, and all events resolved spontaneously in response to normalized pCO2 or cessation of xenon administration. Other adverse events occurred in 2.6% of patients including impaired consciousness, tremors, hypertension, dyspnea, taste disturbance, and numbness.66 Importantly, for both of these large studies,65,66 the severity of underlying neurologic disorders in these patients may have contributed to the occurrence of adverse events.
Moreover, because xenon gas rapidly dissolves in the blood and freely crosses the blood-brain barrier, this subanesthetic concentration provides good brain penetration and establishes cerebral levels of xenon sufficient to be detected by Xe-CT.67 In addition, several other small studies68–72 have examined the administration of subsedative doses of xenon (ranging from 10%–47%) to patients or healthy volunteers and found it to be well tolerated and with no significant adverse physiologic effects.
The hypothesis that xenon inhalation therapy could be used for blockade of trauma memory reconsolidation as a clinical strategy to treat disorders of emotional memory is supported by studies showing that (1) xenon inhibits NMDA receptors,64 which are known to play a role in memory reconsolidation73; (2) xenon reduces NMDA-mediated synaptic currents and neuronal plasticity in the basolateral amygdala and CA1 region of the amygdala74 and the hippocampus,75 which are brain areas involved in Pavlovian fear conditioning used to elucidate learning and memory processes including reconsolidation76,77; and (3) NMDA receptor glycine site antagonists like xenon do not appear to have significant abuse potential and do not induce psychosis,78 which is consistent with clinical experience.68
Along these lines, Meloni et al79 examined whether xenon administered after fear memory reactivation could affect subsequent expression of fear-like behavior (freezing) in rats, hypothesizing that xenon would block fear memory reconsolidation. Male Sprague-Dawley rats were trained for contextual and cued fear conditioning, and the effects of inhaled xenon (25%, 1 hour) on fear memory reconsolidation were tested using conditioned freezing measured days or weeks after reactivation/xenon administration. Xenon administration immediately after fear memory reactivation significantly reduced conditioned freezing when tested 48 hours, 96 hours, or 18 days after reactivation/xenon administration. Xenon did not affect freezing when treatment was delayed until 2 hours after reactivation or when administered in the absence of fear memory reactivation. On the basis of these data, Meloni et al79 concluded that (1) xenon substantially and persistently inhibits trauma memory reconsolidation after reactivation in a time-dependent manner, (2) it could be used as a new research tool to characterize reconsolidation and other memory processes, and (3) it could be developed to treat people with PTSD and other disorders related to emotional memory. Similar amnestic-like effects were observed using ketamine given immediately after reactivation of a contextual fear memory, suggesting an NMDA receptor–dependent blockade of reconsolidation80 and supporting the development of translational studies examining the effects of ketamine-assisted psychotherapy for PTSD81 along the same lines as that proposed for xenon.
CONCLUSIONS
Here, we report the remarkable improvement of a patient with panic disorder and PTSD symptoms stemming from exposure to a traumatic event. We believe that by combining xenon inhalation with trauma memory reactivation through a script-driven recounting of the event, memory reconsolidation was effectively inhibited. The overall effect was a reduction in the occurrence of panic attacks, a remission of avoidance of places and cues that triggered distress in the patient, and a regaining of quality of life through this course of trauma-focused pharmacotherapy. Given new evidence for the use of NMDA receptor antagonists as a promising treatment for PTSD, and emerging strategies that combine targeted medications with psychotherapy sessions, we believe these case report data firmly support further study of xenon-based treatments for this debilitating mental illness.
Submitted: October 15, 2018; accepted May 10, 2019.
Published online: September 19, 2019.
Potential conflicts of interest: The authors report no financial or other relationship relevant to the subject of this article. Dr Dobrovolsky is the co-founder of Nobilis Therapeutics, Inc, a company that is developing treatments for psychiatric disorders using the noble gas xenon. Dr Bogin is the co-founder and CEO of Nobilis Therapeutics, Inc, a company that is developing treatments for psychiatric disorders using the noble gas xenon. Dr Meloni is a co-inventor on patent US9737562B2 owned by The McLean Hospital Corporation and licensed by Nobilis Therapeutics, Inc, covering the therapeutic use of xenon for PTSD and other anxiety disorders. He also has received licensing royalties from the above patent and grant funding from Nobilis Therapeutics, Inc, for preclinical research outside of the submitted work.
Funding/support: None.
REFERENCES
1. PTSD. National Center for PTSD. https://www.ptsd.va.gov/understand/common/common_veterans.asp. Accessed August 19, 2019.
2. Friedman MJ. Finalizing PTSD in DSM-5: getting here from there and where to go next. J Trauma Stress. 2013;26(5):548–556. PubMed CrossRef
3. Schell TL. Invisible Wounds of War: Psychological and Cognitive Injuries, Their Consequences, and Services to Assist Recovery. Santa Monica, CA: Rand Corporation; 2008:87–115.
4. Schnurr PP, Lunney CA, Bovin MJ, et al. Posttraumatic stress disorder and quality of life: extension of findings to veterans of the wars in Iraq and Afghanistan. Clin Psychol Rev. 2009;29(8):727–735. PubMed CrossRef
5. Friedman MJ. Posttraumatic stress disorder among military returnees from Afghanistan and Iraq. Am J Psychiatry. 2006;163(4):586–593. PubMed CrossRef
6. Hoge CW, Auchterlonie JL, Milliken CS. Mental health problems, use of mental health services, and attrition from military service after returning from deployment to Iraq or Afghanistan. JAMA. 2006;295(9):1023–1032. PubMed CrossRef
7. Cohen BE, Marmar CR, Neylan TC, et al. Posttraumatic stress disorder and health-related quality of life in patients with coronary heart disease: findings from the Heart and Soul Study. Arch Gen Psychiatry. 2009;66(11):1214–1220. PubMed CrossRef
8. Kang HK, Bullman TA. Risk of suicide among US veterans after returning from the Iraq or Afghanistan war zones. JAMA. 2008;300(6):652–653. PubMed CrossRef
9. Johnson DR, Fontana A, Lubin H, et al. Long-term course of treatment-seeking Vietnam veterans with posttraumatic stress disorder: mortality, clinical condition, and life satisfaction. J Nerv Ment Dis. 2004;192(1):35–41. PubMed CrossRef
10. Breslau N, Davis GC, Peterson EL, et al. A second look at comorbidity in victims of trauma: the posttraumatic stress disorder-major depression connection. Biol Psychiatry. 2000;48(9):902–909. PubMed CrossRef
11. Bernardy NC, Lund BC, Alexander B, et al. Prescribing trends in veterans with posttraumatic stress disorder. J Clin Psychiatry. 2012;73(3):297–303. PubMed CrossRef
12. Brady K, Pearlstein T, Asnis GM, et al. Efficacy and safety of sertraline treatment of posttraumatic stress disorder: a randomized controlled trial. JAMA. 2000;283(14):1837–1844. PubMed CrossRef
13. Davidson JR, Rothbaum BO, van der Kolk BA, et al. Multicenter, double-blind comparison of sertraline and placebo in the treatment of posttraumatic stress disorder. Arch Gen Psychiatry. 2001;58(5):485–492. PubMed CrossRef
14. Marshall RD, Beebe KL, Oldham M, et al. Efficacy and safety of paroxetine treatment for chronic PTSD: a fixed-dose, placebo-controlled study. Am J Psychiatry. 2001;158(12):1982–1988. PubMed CrossRef
15. Hertzberg MA, Feldman ME, Beckham JC, et al. Lack of efficacy for fluoxetine in PTSD: a placebo controlled trial in combat veterans. Ann Clin Psychiatry. 2000;12(2):101–105. PubMed CrossRef
16. Friedman MJ, Marmar CR, Baker DG, et al. Randomized, double-blind comparison of sertraline and placebo for posttraumatic stress disorder in a Department of Veterans Affairs setting. J Clin Psychiatry. 2007;68(5):711–720. PubMed CrossRef
17. Ursano RJ, Bell C, Eth S, et al; Work Group on ASD and PTSD; Steering Committee on Practice Guidelines. Practice Guideline for the Treatment of Patients With Acute Stress Disorder and Posttraumatic Stress Disorder. Am J Psychiatry. 2004;161(suppl):3–31. PubMed
18. Davidson J, Baldwin D, Stein DJ, et al. Treatment of posttraumatic stress disorder with venlafaxine extended release: a 6-month randomized controlled trial. Arch Gen Psychiatry. 2006;63(10):1158–1165. PubMed CrossRef
19. Raskind MA, Peterson K, Williams T, et al. A trial of prazosin for combat trauma PTSD with nightmares in active-duty soldiers returned from Iraq and Afghanistan. Am J Psychiatry. 2013;170(9):1003–1010. PubMed CrossRef
20. Raskind MA, Peskind ER, Chow B, et al. A trial of prazosin for post-traumatic stress disorder in military veterans. N Engl J Med. 2018;378(6):507–517. PubMed CrossRef
21. Department of Veterans Affairs/Department of Defense. VA/DOD Clinical Practice Guideline for the Management of Posttraumatic Stress Disorder and Acute Stress Disorder. https://www.healthquality.va.gov/guidelines/MH/ptsd/VADoDPTSDCPGFinal.pdf. Accessed August 19, 2019.
22. Rothbaum BO, Price M, Jovanovic T, et al. A randomized, double-blind evaluation of D-cycloserine or alprazolam combined with virtual reality exposure therapy for posttraumatic stress disorder in Iraq and Afghanistan War veterans. Am J Psychiatry. 2014;171(6):640–648. PubMed CrossRef
23. Sveen J, Bondjers K, Willebrand M. Psychometric properties of the PTSD Checklist for DSM-5: a pilot study. Eur J Psychotraumatol. 2016;7(1):30165. PubMed CrossRef
24. Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(suppl 20):22–33, quiz 34–57. PubMed
25. Carlson AP, Brown AM, Zager E, et al. Xenon-enhanced cerebral blood flow at 28% xenon provides uniquely safe access to quantitative, clinically useful cerebral blood flow information: a multicenter study. AJNR Am J Neuroradiol. 2011;32(7):1315–1320. PubMed CrossRef
26. Foa EB, Hembree E, Rothbaum BO. Prolonged Exposure Therapy for PTSD: Emotional Processing of Traumatic Experiences, Therapist Guide. Oxford, UK: Oxford University Press; 2007.
27. Difede J, Cukor J, Wyka K, et al. D-cycloserine augmentation of exposure therapy for post-traumatic stress disorder: a pilot randomized clinical trial. Neuropsychopharmacology. 2014;39(5):1052–1058. PubMed CrossRef
28. Hong I, Song B, Lee S, et al. Extinction of cued fear memory involves a distinct form of depotentiation at cortical input synapses onto the lateral amygdala. Eur J Neurosci. 2009;30(11):2089–2099. PubMed CrossRef
29. Foa EB. In: Kean TM, Friedman M, Cohen JA, eds. Effective Treatments for PTSD: Practice Guidelines From the International Society for Traumatic Stress Studies. New York, NY; Guilford Press: 2010.
30. Institute of Medicine (IOM). Treatment of Posttraumatic Stress Disorder: An Assessment of the Evidence. Washington, DC: The National Academies Press; 2008.
31. Foa EB, McLean CP, Zang Y, et al; STRONG STAR Consortium. Effect of prolonged exposure therapy delivered over 2 weeks vs 8 weeks vs present-centered therapy on PTSD symptom severity in military personnel: a randomized clinical trial. JAMA. 2018;319(4):354–364. PubMed CrossRef
32. Amtul Z, Atta-Ur-Rahman. Neural plasticity and memory: molecular mechanism. Rev Neurosci. 2015;26(3):253–268. PubMed CrossRef
33. Myers KM, Davis M. Systems-level reconsolidation: reengagement of the hippocampus with memory reactivation. Neuron. 2002;36(3):340–343. PubMed CrossRef
34. Steenkamp MM, Litz BT, Hoge CW, et al. Psychotherapy for military-related PTSD: a review of randomized clinical trials. JAMA. 2015;314(5):489–500. PubMed CrossRef
35. Lattal KM, Abel T. Behavioral impairments caused by injections of the protein synthesis inhibitor anisomycin after contextual retrieval reverse with time. Proc Natl Acad Sci U S A. 2004;101(13):4667–4672. PubMed CrossRef
36. Misanin JR, Miller RR, Lewis DJ. Retrograde amnesia produced by electroconvulsive shock after reactivation of a consolidated memory trace. Science. 1968;160(3827):554–555. PubMed CrossRef
37. Nader K, Schafe GE, Le Doux JE. Fear memories require protein synthesis in the amygdala for reconsolidation after retrieval. Nature. 2000;406(6797):722–726. PubMed CrossRef
38. Flood JF, Bennett EL, Orme AE, et al. Effects of protein synthesis inhibition on memory for active avoidance training. Physiol Behav. 1975;14(2):177–184. PubMed CrossRef
39. Flood JF, Bennett EL, Orme E, et al. Relation of memory formation to controlled amounts of brain protein synthesis. Physiol Behav. 1975;15(1):97–102. PubMed CrossRef
40. Hirsch SJ, Regmi NL, Birnbaum SG, et al. CA1-specific deletion of NMDA receptors induces abnormal renewal of a learned fear response. Hippocampus. 2015;25(11):1374–1379. PubMed CrossRef
41. Vieira PA, Corches A, Lovelace JW, et al. Prefrontal NMDA receptors expressed in excitatory neurons control fear discrimination and fear extinction. Neurobiol Learn Mem. 2015;119:52–62. PubMed CrossRef
42. Fitzgerald PJ, Seemann JR, Maren S. Can fear extinction be enhanced? a review of pharmacological and behavioral findings. Brain Res Bull. 2014;105:46–60. PubMed CrossRef
43. Morrison FG, Ressler KJ. From the neurobiology of extinction to improved clinical treatments. Depress Anxiety. 2014;31(4):279–290. PubMed CrossRef
44. Zimmerman JM, Maren S. NMDA receptor antagonism in the basolateral but not central amygdala blocks the extinction of Pavlovian fear conditioning in rats. Eur J Neurosci. 2010;31(9):1664–1670. PubMed
45. Krystal JH, Davis LL, Neylan TC, et al. It is time to address the crisis in the pharmacotherapy of posttraumatic stress disorder: a consensus statement of the PTSD Psychopharmacology Working Group. Biol Psychiatry. 2017;82(7):e51–e59. PubMed CrossRef
46. Furini C, Myskiw J, Izquierdo I. The learning of fear extinction. Neurosci Biobehav Rev. 2014;47:670–683. PubMed CrossRef
47. Ledgerwood L, Richardson R, Cranney J. Effects of D-cycloserine on extinction of conditioned freezing. Behav Neurosci. 2003;117(2):341–349. PubMed CrossRef
48. Abraini JH, David HN, Lemaire M. Potentially neuroprotective and therapeutic properties of nitrous oxide and xenon. Ann N Y Acad Sci. 2005;1053(1):289–300. PubMed CrossRef
49. Suzuki T, Koyama H, Sugimoto M, et al. The diverse actions of volatile and gaseous anesthetics on human-cloned 5-hydroxytryptamine3 receptors expressed in xenopus oocytes. Anesthesiology. 2002;96(3):699–704. PubMed CrossRef
50. Yamakura T, Harris RA. Effects of gaseous anesthetics nitrous oxide and xenon on ligand-gated ion channels: comparison with isoflurane and ethanol. Anesthesiology. 2000;93(4):1095–1101. PubMed CrossRef
51. Weigt HU, Fohr KJ, Georgieff M, et al. Xenon blocks AMPA and NMDA receptor channels by different mechanisms. Acta Neurobiol Exp (Warsz). 2009;69(4):429–440. PubMed
52. Bantel C, Maze M, Trapp S. Noble gas xenon is a novel adenosine triphosphate-sensitive potassium channel opener. Anesthesiology. 2010;112(3):623–630. PubMed CrossRef
53. Mattusch C, Kratzer S, Buerge M, et al. Impact of hyperpolarization-activated, cyclic nucleotide-gated cation channel type 2 for the xenon-mediated anesthetic effect: evidence from in vitro and in vivo experiments. Anesthesiology. 2015;122(5):1047–1059. PubMed CrossRef
54. Gruss M, Bushell TJ, Bright DP, et al. Two-pore-domain K+ channels are a novel target for the anesthetic gases xenon, nitrous oxide, and cyclopropane. Mol Pharmacol. 2004;65(2):443–452. PubMed CrossRef
55. Fahlenkamp AV, Rossaint R, Coburn M. Neuroprotection by noble gases: new developments and insights. Anaesthesist. 2015;64(11):855–858. PubMed CrossRef
56. Peng T, Britton GL, Kim H, et al. Therapeutic time window and dose dependence of xenon delivered via echogenic liposomes for neuroprotection in stroke. CNS Neurosci Ther. 2013;19(10):773–784. PubMed
57. Dixon BJ, Reis C, Ho WM, et al. Neuroprotective strategies after neonatal hypoxic ischemic encephalopathy. Int J Mol Sci. 2015;16(9):22368–22401. PubMed CrossRef
58. Sutherland BA, Harrison JC, Nair SM, et al. Inhalation gases or gaseous mediators as neuroprotectants for cerebral ischaemia. Curr Drug Targets. 2013;14(1):56–73. PubMed CrossRef
59. Cullen SC, Gross EG. The anesthetic properties of xenon in animals and human beings, with additional observations on krypton. Science. 1951;113(2942):580–582. PubMed CrossRef
60. Dobrovolsky A, Ichim TE, Ma D, et al. Xenon in the treatment of panic disorder: an open label study. J Transl Med. 2017;15(1):137. PubMed CrossRef
61. Ressler KJ, Rothbaum BO, Tannenbaum L, et al. Cognitive enhancers as adjuncts to psychotherapy: use of D-cycloserine in phobic individuals to facilitate extinction of fear. Arch Gen Psychiatry. 2004;61(11):1136–1144. PubMed CrossRef
62. Kushner MG, Kim SW, Donahue C, et al. D-cycloserine augmented exposure therapy for obsessive-compulsive disorder. Biol Psychiatry. 2007;62(8):835–838. PubMed CrossRef
63. Bürkner P-C, Bittner N, Holling H, et al. D-cycloserine augmentation of behavior therapy for anxiety and obsessive-compulsive disorders: a meta-analysis. PLoS One. 2017;12(3):e0173660. PubMed CrossRef
64. Dickinson R, Peterson BK, Banks P, et al. Competitive inhibition at the glycine site of the N-methyl-d-aspartate receptor by the anesthetics xenon and isoflurane: evidence from molecular modeling and electrophysiology. Anesthesiology. 2007;107(5):756–767. PubMed CrossRef
65. Latchaw RE, Yonas H, Pentheny SL, et al. Adverse reactions to xenon-enhanced CT cerebral blood flow determination. Radiology. 1987;163(1):251–254. PubMed CrossRef
66. Carlson AP, Brown AM, Zager E, et al. Xenon-enhanced cerebral blood flow at 28% xenon provides uniquely safe access to quantitative, clinically useful cerebral blood flow information: a multicenter study. AJNR Am J Neuroradiol. 2011;32(7):1315–1320. PubMed CrossRef
67. Wintermark M, Sesay M, Barbier E, et al. Comparative overview of brain perfusion imaging techniques. Stroke. 2005;36(9):e83–e99. PubMed CrossRef
68. Bedi A, McCarroll C, Murray JM, et al. The effects of subanaesthetic concentrations of xenon in volunteers. Anaesthesia. 2002;57(3):233–241. PubMed CrossRef
69. Yagi M, Mashimo T, Kawaguchi T, et al. Analgesic and hypnotic effects of subanaesthetic concentrations of xenon in human volunteers: comparison with nitrous oxide. Br J Anaesth. 1995;74(6):670–673. PubMed CrossRef
70. Lorenz M, Holl K, Nemati N, et al. Effects of 33% stable xenon/O2 mixture on somatosensory evoked potentials. Neurol Res. 1991;13(2):133–135. PubMed CrossRef
71. Yonas H, Grundy B, Gur D, et al. Side effects of xenon inhalation. J Comput Assist Tomogr. 1981;5(4):591–592. PubMed CrossRef
72. Bedi A, Murray JM, Dingley J, et al. Use of xenon as a sedative for patients receiving critical care. Crit Care Med. 2003;31(10):2470–2477. PubMed CrossRef
73. Suzuki A, Josselyn SA, Frankland PW, et al. Memory reconsolidation and extinction have distinct temporal and biochemical signatures. J Neurosci. 2004;24(20):4787–4795. PubMed CrossRef
74. Haseneder R, Kratzer S, Kochs E, et al. Xenon reduces N-methyl-d-aspartate and alpha-amino-3-hydroxy-5-methyl-4-isoxazolepropionic acid receptor-mediated synaptic transmission in the amygdala. Anesthesiology. 2008;109(6):998–1006. PubMed CrossRef
75. Kratzer S, Mattusch C, Kochs E, et al. Xenon attenuates hippocampal long-term potentiation by diminishing synaptic and extrasynaptic N-methyl-d-aspartate receptor currents. Anesthesiology. 2012;116(3):673–682. PubMed CrossRef
76. Johansen JP, Cain CK, Ostroff LE, et al. Molecular mechanisms of fear learning and memory. Cell. 2011;147(3):509–524. PubMed CrossRef
77. VanElzakker MB, Dahlgren MK, Davis FC, et al. From Pavlov to PTSD: the extinction of conditioned fear in rodents, humans, and anxiety disorders. Neurobiol Learn Mem. 2014;113:3–18. PubMed CrossRef
78. Beardsley PM, Ratti E, Balster RL, et al. The selective glycine antagonist gavestinel lacks phencyclidine-like behavioral effects. Behav Pharmacol. 2002;13(7):583–592. PubMed CrossRef
79. Meloni EG, Gillis TE, Manoukian J, et al. Xenon impairs reconsolidation of fear memories in a rat model of post-traumatic stress disorder (PTSD). PLoS One. 2014;9(8):e106189. PubMed CrossRef
80. Duclot F, Perez-Taboada I, Wright KN, et al. Prediction of individual differences in fear response by novelty seeking, and disruption of contextual fear memory reconsolidation by ketamine. Neuropharmacology. 2016;109:293–305. PubMed CrossRef
81. Veen C, Jacobs G, Philippens I, et al. Subanesthetic dose ketamine in posttraumatic stress disorder: a role for reconsolidation during trauma-focused psychotherapy. Curr Top Behav Neurosci. 2018;38:137–162. PubMed CrossRef
This PDF is free for all visitors!



