Beneficial Effects of Fluvoxamine for Chorea in a Patient With Huntington’s Disease: A Case Report
To the Editor: Huntington’s disease is a neurodegenerative illness that has a robust genetic basis with onset in middle age and that is characterized by involuntary choreatic movements, behavioral and psychiatric disturbances, and dementia. The etiopathogenesis of Huntington’s disease has still not been resolved, and a cure does not exist; the many therapeutic options currently available exist only for treating symptoms and signs with a view to improving quality of life. We report a case in which a patient with Huntington’s disease benefited from fluvoxamine treatment in terms of mood symptoms as well as choreatic movements.1
Case report. Mr A, a 38-year-old man, suffered from depressed mood, insomnia, poor appetite, fatigue, and difficulty concentrating; occasional involuntary violent behavior toward family members; involuntary sudden movements in his upper limbs; and involuntary muscle contractions in his face and trunk. Per his history, the involuntary movements had started initially with his fingers 2 years ago, but he had not presented to the hospital. After a year and a half, involuntary movements spread to his upper limbs and were present during the day except when the patient was sleeping. He presented at that time to a neurology department in another city, but he did not continue his follow-up treatment.
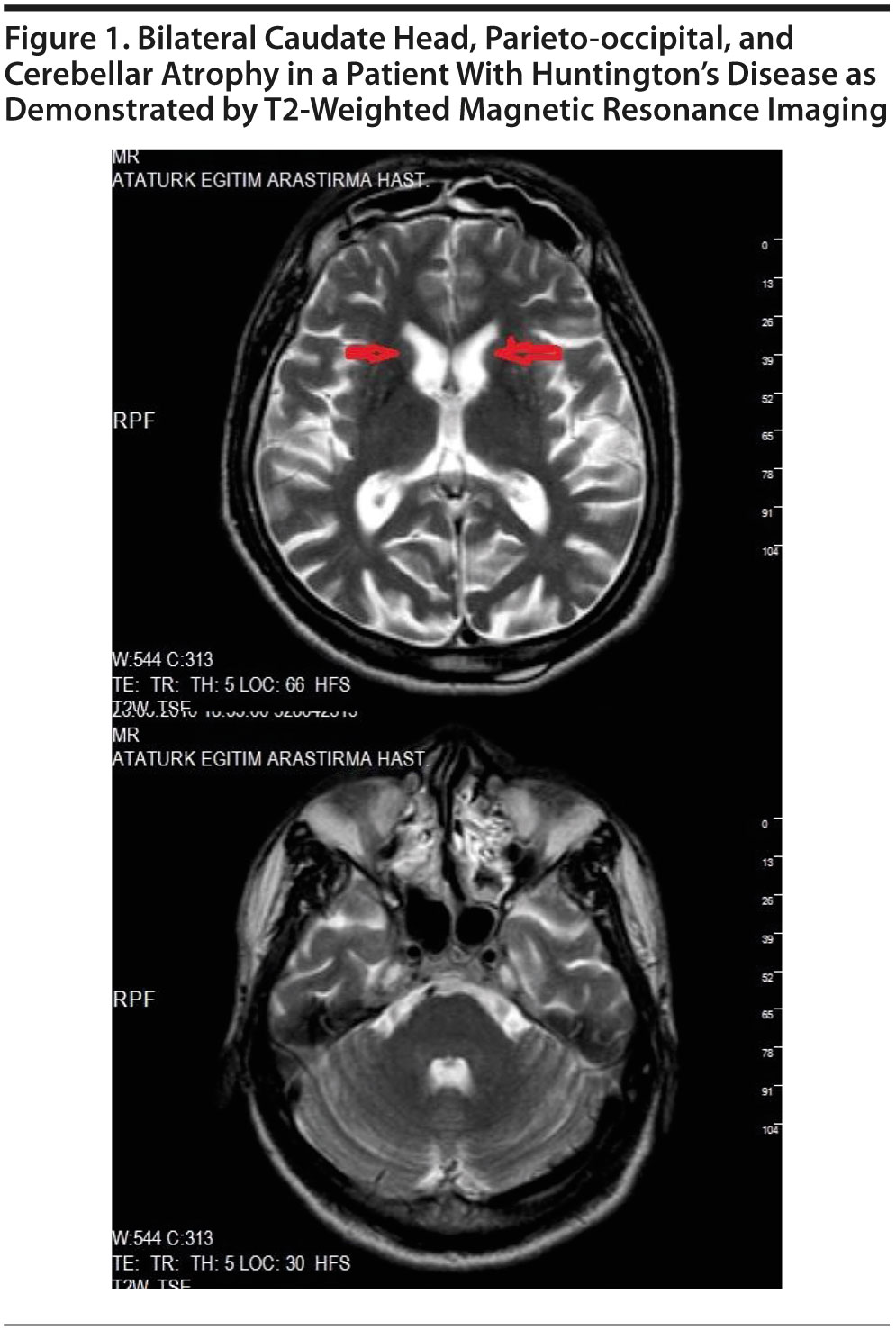
He presented to our outpatient clinic approximately 2 months later with complaints of depressed mood, insomnia, poor appetite, fatigue, and difficulty concentrating as well as occasional involuntary violent behavior and abnormal movements of different parts of his body, and he agreed to be hospitalized. On psychiatric examination, depressed and anxious mood, insomnia, poor appetite, fatigue, and aggressiveness were noted. His cognitive functioning was within normal limits. On physical and neurologic examination, chorea was noted in both arms and both hands and also his face and neck. He had no exposure to antipsychotic medication. Family history revealed that his mother had similar abnormal movements and that she died 5 or 6 years after initiation of these abnormal movements; however, she could not be diagnosed. Electroencephalography revealed no abnormalities, and blood chemistry measurements, complete blood cell count, and thyroid function tests were all within normal limits. Brain magnetic resonance imaging revealed focal cortical bilateral atrophy in occipital and parieto-occipital lobes (Figure 1) as well as bicaudate atrophy and cerebellar atrophy.
Click figure to enlarge
Consultation from the neurology department was made. Huntington’s disease was suspected, and the neurology department recommended a genetic investigation. He scored 22 on the Hamilton Depression Rating Scale (HDRS)2 and received a diagnosis of mood disorder (major depressive disorder) due to organic etiology according to DSM-IV-TR. He was started on fluvoxamine 100 mg/d. After 5 days, his choreatic movements decreased dramatically, but did not disappear. With the patient’s permission, we interrupted fluvoxamine treatment to understand whether or not the decrease in chorea stemmed from fluvoxamine treatment. Two days after fluvoxamine was stopped, chorea of the upper limbs increased dramatically. Genetic investigation confirmed CAG repeats in the abnormal range (1 allele with 40 repeats and another with 17 repeats) after 4 weeks, at which time Mr A was diagnosed with Huntington’s disease. At the fifth week, his depression had remitted as determined by an HDRS score of 6. His choreatic movements decreased but did not disappear. At outpatient follow-up, his symptoms were as stable as at discharge.
Huntington’s disease is an autosomal dominantly inherited disease caused by an elongated CAG repeat on the short arm of chromosome 4p16.3 in Huntingtin gene 2. Curative treatment does not exist. Hyperkinesia, or chorea, is treated with dopamine receptor blocking or depleting agents.3
A study that included the selective sigma-1 receptor agonist [11C]SA4503 and positron emission tomography showed that fluvoxamine bound to sigma-1 receptors in the living human brain at therapeutic doses, suggesting that sigma-1 receptors play a role in the mechanism of action of fluvoxamine. There is also conflicting evidence that sigma-1 agonists increase and reduce dopamine levels in the striatum.4 Although Furuse and Hashimoto5,6 reported antipsychotic-induced akathisia cases that resolved with administration of the sigma-1 receptor agonist fluvoxamine, the mechanism of the benefit was unclear due to the complex pathophysiology of akathisia. We7 reported that fluvoxamine was effective for treating both hemiballism and depression in a patient, and suggested that fluvoxamine might act as a reducer of dopamine in the striatal area. We more recently reported a case in which fluvoxamine was beneficial for tardive dyskinesia as well as major depressive disorder.8 Similarly, fluvoxamine reduced dopaminergic activity in the striatal area in the present case.
In conclusion, to our knowledge, this is the first case study in which the potent sigma-1 agonist fluvoxamine was shown to be effective in reducing chorea as well as treating depressive disorder in a patient with Huntington’s disease. It is difficult, in a case study, to demonstrate the effects of fluvoxamine on hyperkinetic movement disorders. More detailed, double-blind studies should clarify the potential use of fluvoxamine in the treatment of hyperkinetic movement disorders.
Author affiliations: Kırklareli State Hospital, Kırklareli (Dr Albayrak), and Department of Psychiatry, Atat×¼rk Research and Education Hospital, Ankara (Drs G. K. UÄŸurlu, M. UÄŸurlu, and Çayköyl×¼), Turkey.
Potential conflicts of interest: None reported.
Funding/support: None reported.
Published online: November 1, 2012.
Prim Care Companion CNS Disord 2012;14(6):doi:10.4088/PCC.12l01369
© Copyright 2012 Physicians Postgraduate Press, Inc.
References
1. Bruyn GW. Huntington’s chorea: historical, clinical and laboratory synopsis. In: Vinken PJ, Bruyn GW, eds. Handbook of Clinical Neurology. Vol 6. Amsterdam, The Netherlands: Elsevier; 1968:298-378.
2. Hamilton M. A rating scale for depression. J Neurol Neurosurg Psychiatry. 1960;23(1):56-62. PubMed doi:10.1136/jnnp.23.1.56
3. Huntington Study Group. Tetrabenazine as antichorea therapy in Huntington disease: a randomized controlled trial. Neurology. 2006;66(3):366-372. PubMed doi:10.1212/01.wnl.0000198586.85250.13
4. Ishikawa M, Ishiwata K, Ishii K, et al. High occupancy of sigma-1 receptors in the human brain after single oral administration of fluvoxamine: a positron emission tomography study using [11C]SA4503. Biol Psychiatry. 2007;62(8):878-883. PubMed doi:10.1016/j.biopsych.2007.04.001
5. Furuse T, Hashimoto K. Fluvoxamine for blonanserin-associated akathisia in patients with schizophrenia: report of five cases. Ann Gen Psychiatry. 2010;9(1):17. PubMed doi:10.1186/1744-859X-9-17
6. Furuse T, Hashimoto K. Fluvoxamine for aripiprazole-associated akathisia in patients with schizophrenia: a potential role of sigma-1 receptors. Ann Gen Psychiatry. 2010;9(1):11. doi:10.1186/1744-859X-9-11 PubMed
7. Cayköyl×¼ A, Albayrak Y, UÄŸurlu GK, et al. Beneficial effects of fluvoxamine for hemiballism in a patient with depressive disorder: a case report. Acta Neurol Belg. 2011;111(1):62-65. PubMed
8. Albayrak Y, Ekinci O. Duloxetine-associated tardive dyskinesia resolved with fluvoxamine: a case report. J Clin Psychopharmacol. In press.



