From Lithium Intoxication to Lung Cancer: A Woman’s Diagnostic Journey
To the Editor: Sometimes, the suspicion of lithium intoxication may cause an “intoxication” in clinical diagnosis.
Case report. Ms A, a 47-year-old woman with bipolar affective disorder (of multiple etiologies, including those conforming to ICD-10 and DSM-IV criteria) who had been treated with lithium, was admitted to our emergency department in December 2009 for myalgia, fever, and generalized weakness. Five years prior, she attempted suicide by jumping from the fifth floor. She had spinal decompression from T12-L3 as well as an instrumented reconstruction with platinum rods. Because of the spinal cord injury, she was using a catheter to empty the bladder.
Her body temperature was 37.5°C. An x-ray study of the chest showed an infiltration into the left apex. Urinalysis revealed trace bacteria, 9-11 white blood cells per high power field. The plasma lithium concentration was 2 mmol/L, and the creatinine level was 0.8 mg/dL. The erythrocyte sedimentation rate was 80 mm/h. The 24-hour urine amount was 6000-7000 mL.
In light of these findings, it is thought that lithium toxicity developed due to urinary or pulmonary infection. Lithium was stopped after the possibility of intoxication was identified. Olanzapine was started at the dose of 10 mg/d as a mood stabilizer. Because the patient’s general condition was poor, the lithium could not be restarted and the diagnosis of intoxication could not be confirmed.
The muscle strength in both of the upper extremities was normal. In the lower extremities, paraplegia with brisk deep tendon reflexes and Babinski’s sign was detected bilaterally. These findings were considered sequelae of the prior spinal cord damage. Nerve conduction studies identified a serious decrease in the amplitudes in the lower extremities, suggesting motor axonal damage. The cerebrospinal fluid (CSF) analysis showed 100 white cells/mm3, 315 mg/dL protein, and glucose level within normal limits. In light of these findings, an acute motor axonal neuropathy was diagnosed.
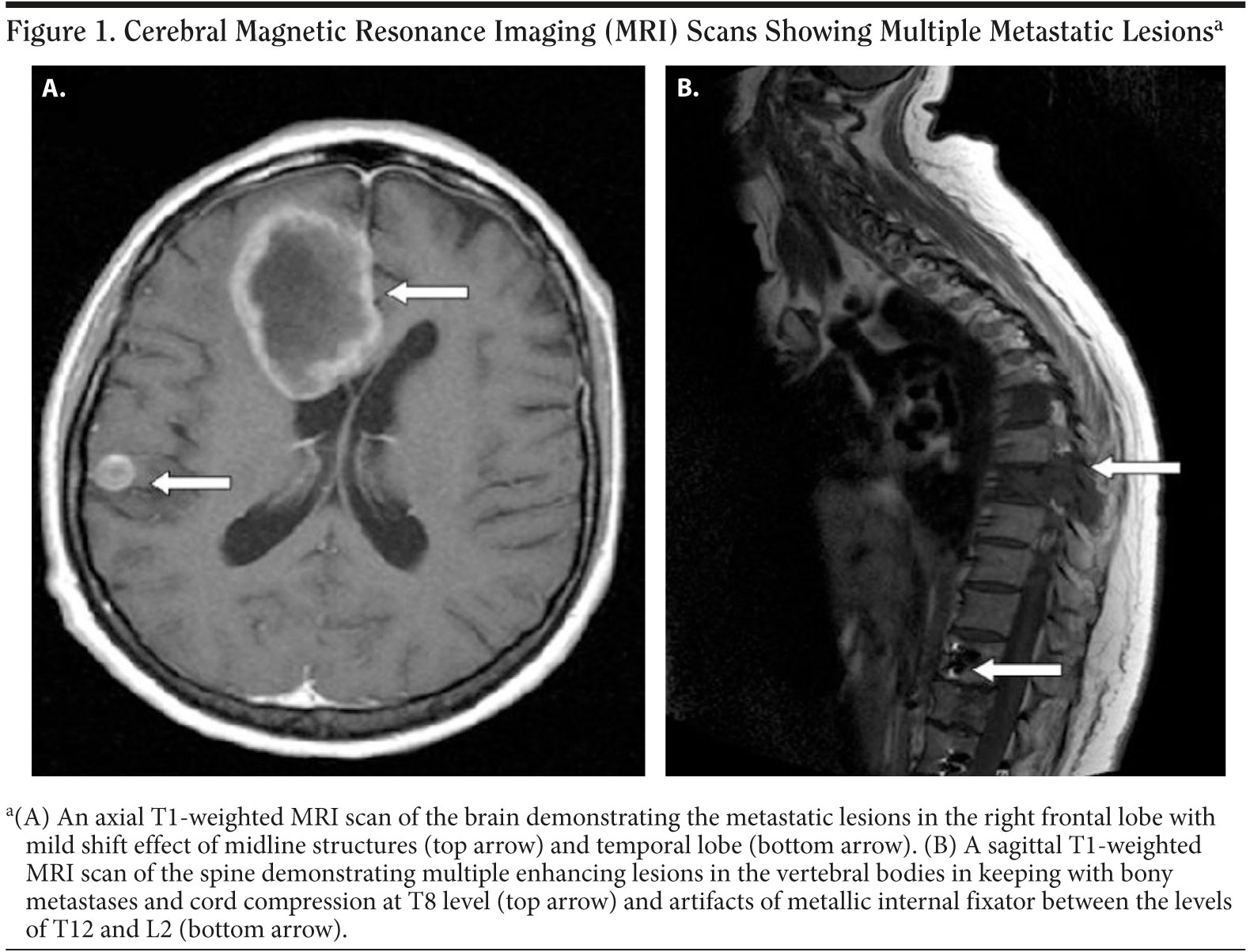
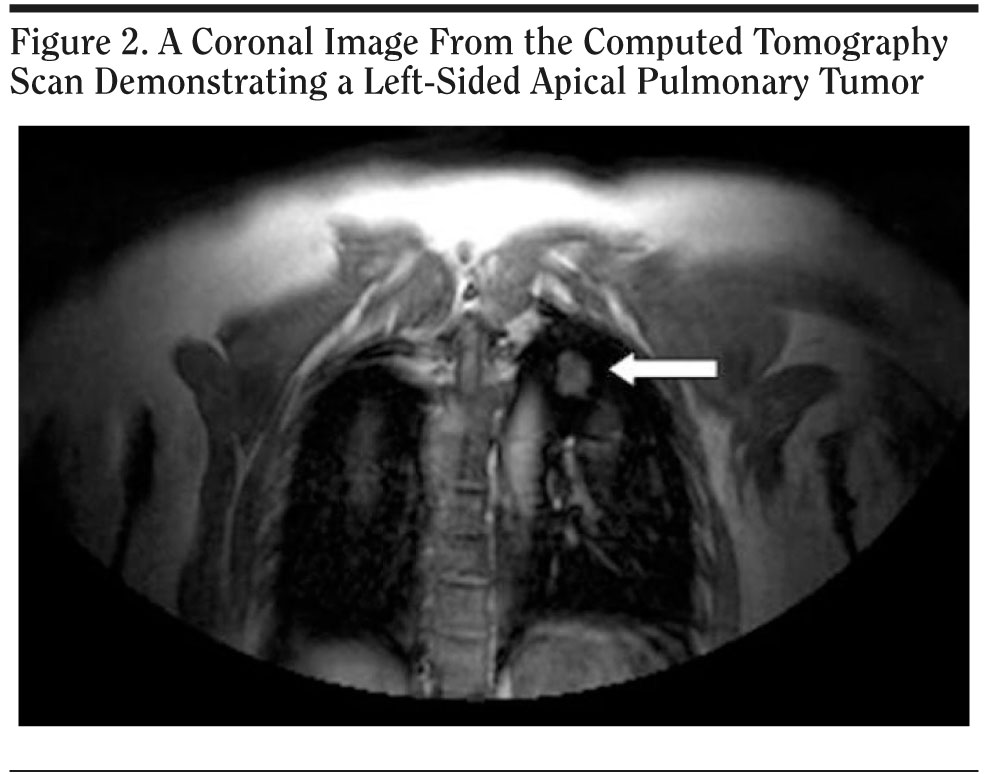
Ms A received intravenous immunoglobulin (0.4 mg/kg/d) for 5 days. No clinical improvement was seen. The second CSF analysis showed 200 white cells/mm3, 823 mg/dL protein, and glucose level within normal limits. The spine was investigated with magnetic resonance imaging (MRI). Because thoracal epidural metastatic lesions were detected in spinal MRI, the cerebral MRI was established for research of spreading. It showed multiple metastatic lesions in brain parenchyma as well (Figure 1). Thoracic computed tomography (CT) showed a lung mass as the primary focus (Figure 2). Biopsy demonstrated lung adenocarcinoma.
Click figure to enlarge
Click figure to enlarge
In this patient, our first diagnosis was chronic lithium intoxication. Lithium is a mood-stabilizing agent commonly used for the treatment of bipolar disorder and it has a narrow therapeutic window from 0.6 to 1.5 mmol/L. Risk factors for lithium intoxication include drug interactions, infection, and dehydration.1
Our second diagnosis was acute motor axonal neuropathy. Acute motor axonal neuropathy is a known variant of Guillain-Barré syndrome with a clinical course that includes motor paralysis, hyporeflexia, albuminocytological dissociation in CSF, and finding of axonal involvement on nerve conduction study.2 Intravenous immunoglobulin and plasmapheresis have also been suggested for acute motor axonal neuropathy, as well as for Guillain-Barré syndrome.3 But our case did not show a response to intravenous immunoglobulin.
Because of the failure to improve despite intravenous immunoglobulin treatment, the patient’s prior spine surgery history, persistent abnormal CSF findings, and isolated lower extremity paresis suggestive of paraspinal lesion clued us that a spine MRI should be done immediately. We thought that lithium intoxication and sequelae findings of the former spinal injury were masking primary lung cancer, a metastatic cranial mass, and neoplastic polyradiculopathy. On the other hand, whole findings may have originated from the combination of these diseases.
References
1. Dunner DL. Optimizing lithium treatment. J Clin Psychiatry. 2000;61(suppl 9):76-81. PubMed
2. Kaida K, Kusunoki S. Guillain-Barré syndrome: update on immunobiology and treatment. Expert Rev Neurother. 2009;9(9):1307-1319. PubMed doi:10.1586/ern.09.77
3. Vucic S, Kiernan MC, Cornblath DR. Guillain-Barré syndrome: an update. J Clin Neurosci. 2009;16(6):733-741. PubMed doi:10.1016/j.jocn.2008.08.033
Author affiliations: Department of Neurology, Faculty of Medicine, Maltepe University, Istanbul, Turkey.
Potential conflicts of interest: None reported.
Funding/support: None reported.
Published online: April 14, 2011 (doi:10.4088/PCC.10l01048gre).
Prim Care Companion CNS Disord 2011;13(2):e1-e2
© Copyright 2011 Physicians Postgraduate Press, Inc.


