Electronic Clinical Decision Support for Management of Depression in Primary Care: A Prospective Cohort Study

ABSTRACT
Objective: To assess the utility of an electronic clinical decision support tool for management of depression in primary care.
Method: This prospective study was conducted in a national network of ambulatory practices over a 1-year period (October 2007-October 2008). A clinical decision support tool was embedded into the electronic health record of 19 primary care practices with 119 providers. The main components included (1) the 9-item Patient Health Questionnaire (PHQ-9), with 9 questions paralleling the 9 DSM-IV criteria for the diagnosis of major depressive disorder; (2) a suicide assessment form; and (3) brief patient and provider education. Use of each component was tracked in the electronic health record. Providers completed baseline and postintervention surveys regarding their depression management practices and their perceptions of the clinical decision support tool.
Results: According to electronic health record tracking, the PHQ-9 form was used in 45.6% of the 16,052 adult patients with depression and in 73.7% of the 1,422 patients with new depression. The suicide assessment form was used in 62.0% of patients with possible suicidality. Education modules were rarely used. From before to after the study, providers reported increased use of standardized tools for depression diagnosis (47% to 80%, P < .001) and monitoring (27% to 85%, P < .001). The majority of providers reported often using the PHQ-9 and suicide forms and felt them to be very helpful in patient care, with 85% planning to continue their use after the study.
Conclusions: The electronic health record-based clinical decision support tool was extensively used and perceived as very helpful for assessment of patients’ symptoms but not for provider education. These findings can help guide national efforts incorporating clinical decision support for quality improvement.
Prim Care Companion CNS Disord 2012;14(1):doi:10.4088/PCC.11m01191
© Copyright 2012 Physicians Postgraduate Press, Inc.
Submitted: March 31, 2011; accepted July 22, 2011.
Published online: February 2, 2012.
Corresponding author: James M. Gill, MD, MPH, Delaware Valley Outcomes Research, 17 Henderson Hill Rd, Newark, DE 19713 ([email protected]).
Depression is a common medical condition, with a 20% prevalence of significant depressive symptoms1 and a 6.6% annual prevalence of major depressive disorder (MDD)2 among adults in the United States. Most people seek care for depression from their primary care physician rather than from a mental health specialist.3-5 Treatment of depression is particularly important in primary care, since many patients with depression have comorbid medical conditions,6 and depression can worsen medical conditions such as diabetes,7-9 cardiovascular disease,10-13 and cancer.14,15
However, treatment of depression in primary care is not always optimal.3,5,16 One reason for this nonoptimal care is that primary care is more complex, with patients often being treated for multiple problems during a single visit.16-18 The Institute of Medicine and other organizations have called for methods to improve depression management in the primary care setting.19 This management includes use of standardized depression symptom questionnaires.
One way to facilitate the use of these tools is through electronic health records (EHRs). An EHR can make depression severity questionnaires easily available at the point of care. The EHR can track results over time so that providers can more easily determine improvement in depression symptoms and incorporate guidelines so that changes in depression scores can trigger recommendations for further treatment. Because of the advantages of EHR-based interventions, the Institute of Medicine and other experts recommend that clinical decision support (CDS) tools be incorporated into EHRs whenever possible.20,21
The purpose of this study was to incorporate a depression severity questionnaire and other CDS tools into the EHR for use at the point of care in primary care settings and to examine use of these tools as well as provider perceptions of how these tools improved quality of care.
METHOD
Setting and Population
This prospective cohort study was conducted within a national practice-based research network called the Centricity Healthcare User Research Network. The Centricity Healthcare User Research Network is a network of physicians and other providers in ambulatory practices that use a particular outpatient EHR, Centricity Electronic Medical Record (GE Healthcare, Waukesha, Wisconsin), and have agreed to share data and participate in quality of care studies. Previous Centricity Healthcare User Research Network studies have examined EHR-based tools for improving quality in primary care settings.22,23
For this study, offices that participate in the Centricity Healthcare User Research Network were recruited if they were primary care offices that cared for adults (family medicine, general internal medicine, or general practice) that had been using the Centricity Electronic Medical Record for at least 1 year. Nineteen offices from 9 states participated in the study. These practices ranged in size from 1 to 24 providers, with a median of 4 and a mean of 6 providers. Within these offices, we included all physicians and midlevel providers (nurse practitioners or physician assistants) who practiced primary care at least 8 hours per week. There were 121 such providers at the beginning of the study plus an additional 2 providers who joined the practices within the initial 3 months of the study, for a total of 123 participants. The study was granted exempt status by the institutional review board of the principal investigator’s institution.

- Symptom severity questionnaires such as the 9-item Patient Health Questionnaire (PHQ-9) can assist primary care clinicians in diagnosing and monitoring depression.
- This study showed that, when embedded into an electronic health record, the PHQ-9 is easy to use and leads to improvements in quality of care.
Interventions
The intervention included a CDS tool that was embedded into the EHR, as well as provider education on guidelines for depression in primary care. The CDS and educational materials were intended to assist in the diagnosis and management of depression on the basis of recommendations of the MacArthur Foundation Initiative on Depression and Primary Care.24
The CDS tool was designed to automatically activate when an EHR note was started for any adult patient office visit with an active diagnosis of depression. Depression was defined by the EHR problem list using ICD-9 codes corresponding to the diagnoses of major depressive disorder (296.2, 296.3), depressive psychosis (298.0), depression not otherwise specified (311), prolonged situational depression (309.1), and dysthymic disorder (300.4). Patients with a codiagnosis of mania (296.0), bipolar disorder (296.4-8), or schizophrenia (295) were excluded since these diagnoses often require referral to a psychiatrist or a change in the approach to treatment of depression. When the form was activated, providers had the option of using the form at that visit or not. They also had the option to indicate that the patient’s depression was being managed elsewhere (eg, by a psychiatrist), in which case the form would no longer activate at future visits. The form could also be manually activated, eg, for patients with a possible new diagnosis of depression.
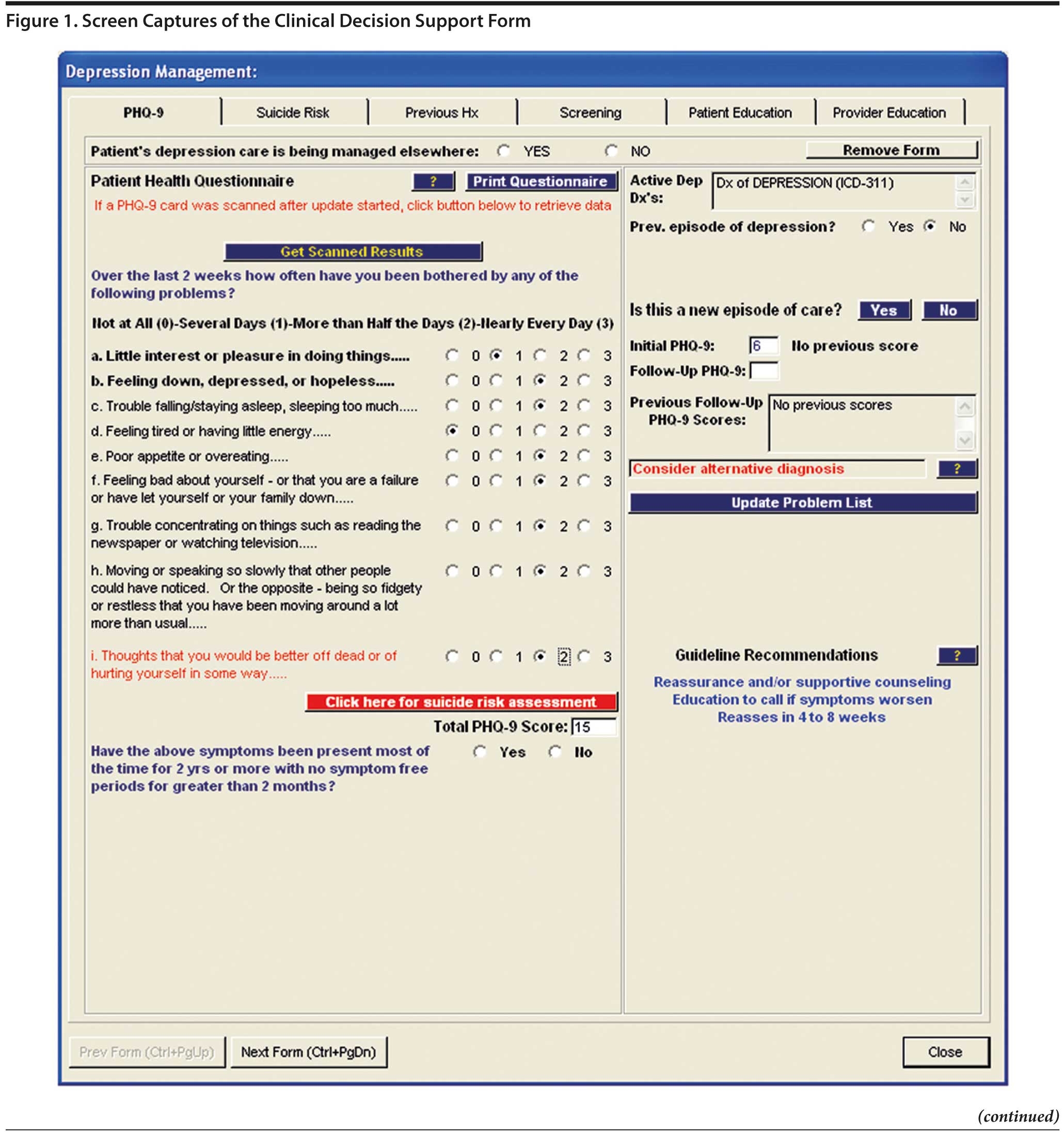
The CDS form had several components, as shown in Figure 1. The first component included the 9-item Patient Health Questionnaire (PHQ-9), with 9 questions paralleling the 9 DSM-IV criteria for the diagnosis of major depressive disorder. The PHQ-9 has been used and validated both for the diagnosis and follow-up of depression.25-29 The PHQ-9 could either be administered by a clinician (by verbally asking questions) or self-administered. When self-administered, the patients could either write their responses on a printed questionnaire or on a Scantron (Scantron Corporation, Eagan, Minnesota) form that was then loaded into the EHR by the staff. Scores were calculated from patients’ responses to the PHQ-9 questions and compared to any previous scores. For new episodes of depression, the form prompted the provider about appropriate diagnoses based on responses to the PHQ-9 (eg, if the patient met the criteria for major depressive disorder, and if so, whether the score indicated mild, moderate, or severe major depressive disorder). For ongoing diagnoses, the provider was prompted depending on whether the patient’s PHQ-9 score had improved according to national guidelines. If the patient’s scores had not improved adequately in an appropriate time frame, a recommendation was provided to consider intensification of therapy. The recommendation did not specify how to intensify therapy (eg, increase dose of medication vs switch or augment medication vs add nonpharmacologic therapy vs refer to a specialist).
Click figure to enlarge
Click figure to enlarge
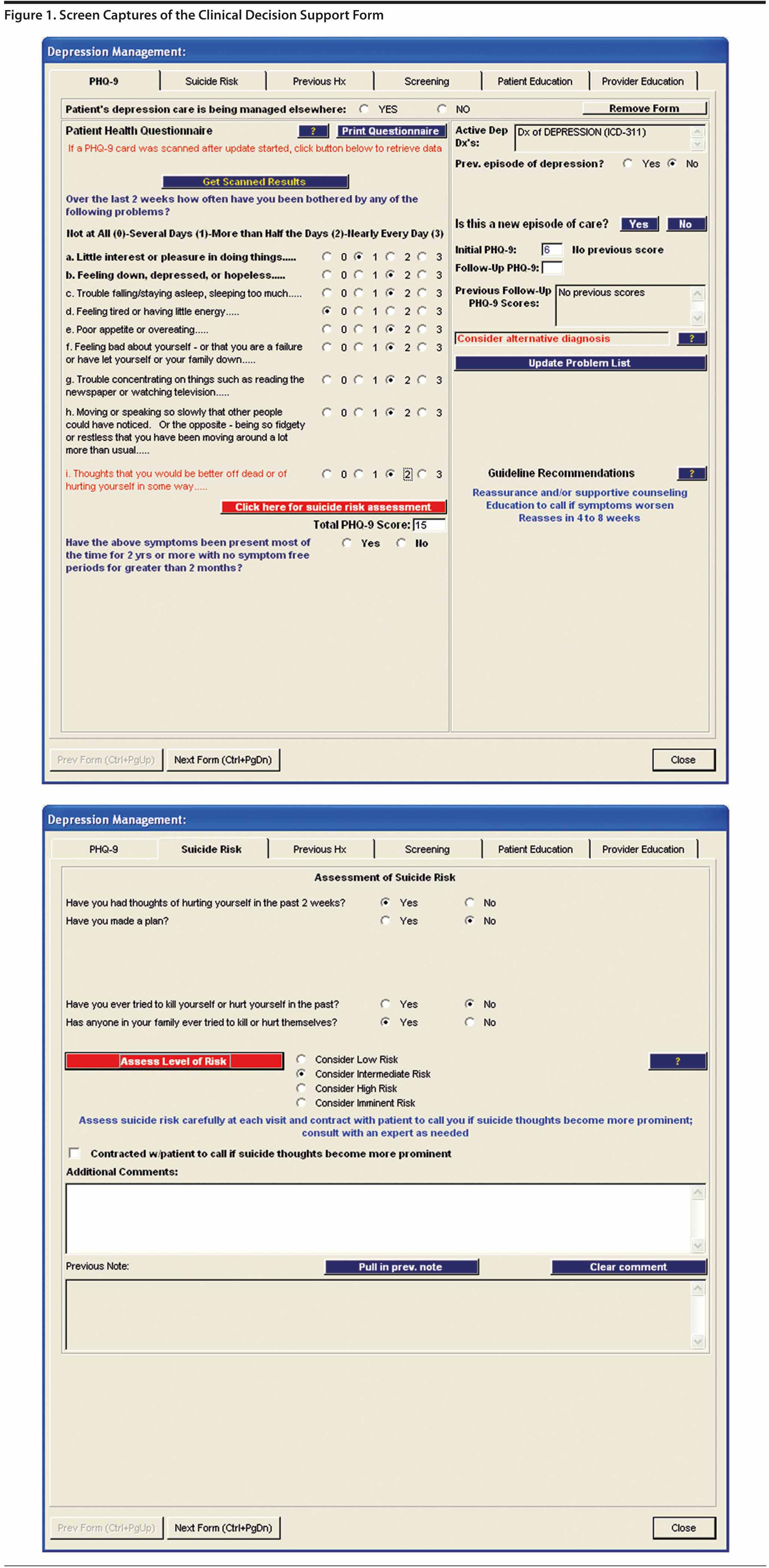
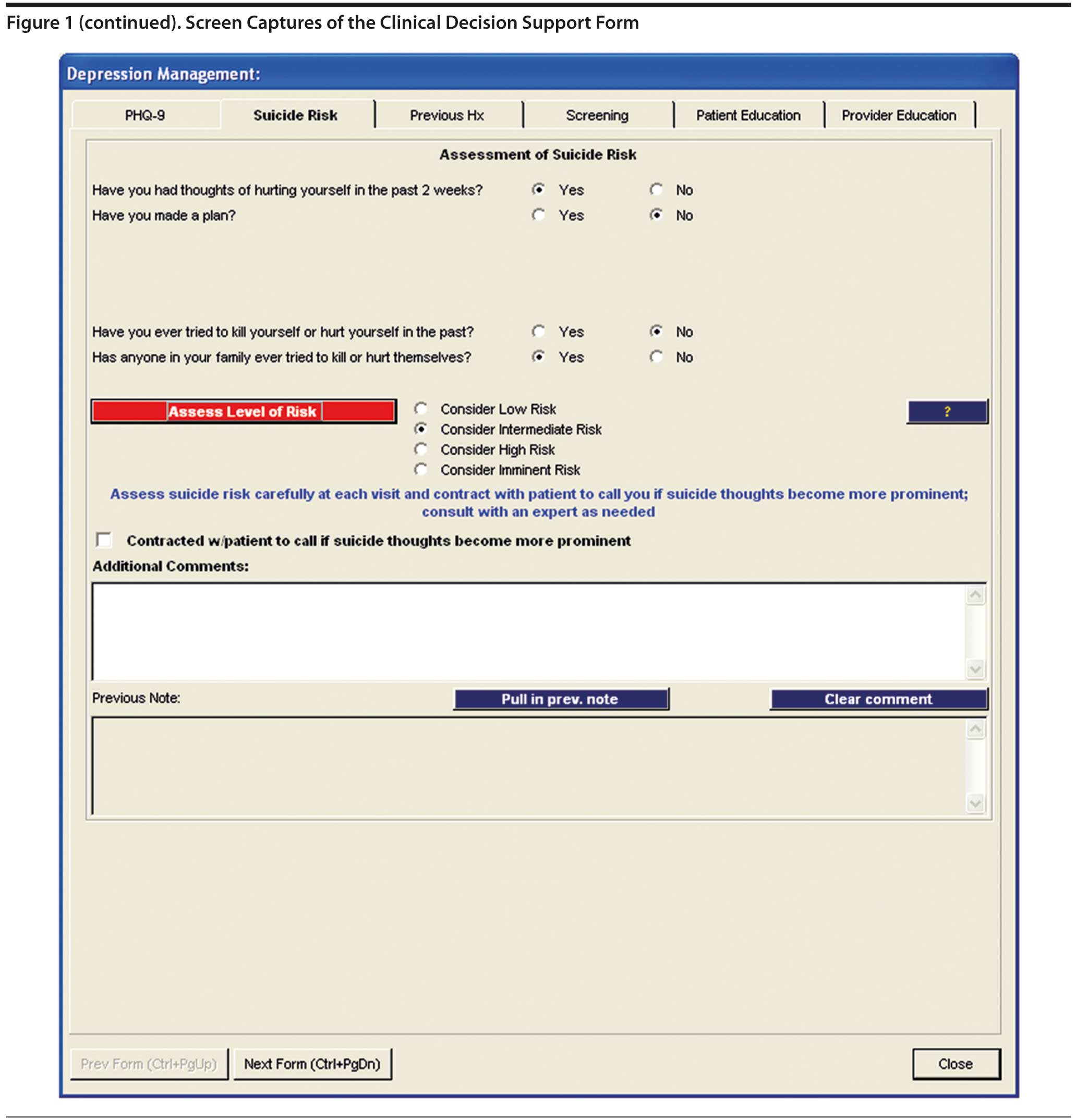
The second component of the form was a suicide risk assessment. Providers were prompted to use this component of the form if the patient’s response to the ninth question on the PHQ-9 indicated possible suicidal thoughts.
A third component of the form included provider education. This provider education was in the form of common clinical questions such as, “What is the best way to manage sexual side effects of antidepressant medications?” This Web-based continuing medical education (CME) was first provided to participating providers prior to the start of the study and remained available during the study period. To access this CME during the study period, providers could go directly to the Web site that was used at the initial CME offering, or they could link to this site through the EHR (in which case they could either complete the CME immediately or could have an e-mail reminder sent to them with a link to the CME module). Finally, the providers had the option of getting “short answers” to the common clinical questions by clicking a button on the EHR form, without going to the longer Web-based CME module.
The form also included patient education materials about depression that could be printed directly from the EHR. The patient education materials included lists of resources wherein patients could get more information or assistance for their depression. Finally, the form included tools to screen for bipolar disorder as well as generalized anxiety disorder and included a place to document previous psychiatric history.
The CDS was implemented by all sites on the same day (October 15, 2007). Prior to this “go-live” day, all providers participated in a training session that included use of the form (including the PHQ-9, education, and other CDS tools). Providers had the choice of completing this training via a live “Web-ex” session or by linking to an archived Web-based training session.
Outcomes
The main outcomes were the providers’ use of the CDS form and educational materials and their opinions of these forms and how they affected their practice. There were 2 ways in which use of the CDS form was measured. First, use of the form was tracked through the EHR. We determined the proportion of active patients with any diagnosis of depression and with new episodes of depression for whom the CDS form was used. Active patients were defined as those with at least 1 office visit during the study year (October 2007-October 2008) and in the prior year. New episodes were defined by a diagnosis of depression that started during the study year, with no diagnosis of depression or antidepressant medication in the prior 6 months.
Second, participating providers were surveyed at the end of the study period via a Web-based survey. This survey included questions about how frequently they used the specific components of the form and how these components were used. In addition to questions about use of the study forms, providers were asked about their usual practice with regard to use of standardized tools to diagnosis and monitor depression. These latter questions were asked both before the study and at the end of the study in order to examine changes in practice patterns. Finally, providers were asked about their practice characteristics (eg, practice location) and their personal characteristics (eg, age, gender, specialty, and years in practice) prior to the study. We also compared provider responses regarding use of the key components of the form across specialty and years in practice. For analytic simplicity, years in practice was categorized ≤ 10 years or ≥ 10 years. For these comparisons, the χ2 test was used, with P < .05 as the cutoff for statistical significance.
RESULTS
The 123 participating providers had 77,335 active adult patients, 16,052 (20.8%) of whom had a diagnosis of depression and 1,422 (1.8%) of whom met the criteria for a new episode of depression during the study year. Of the participating providers, 119 of the 123 (96.7%) completed the baseline survey, including information about their characteristics. Table 1 shows that most of these providers were family physicians and in practice for more than 10 years.
Click figure to enlarge
Click figure to enlarge
Click figure to enlarge
Click figure to enlarge
Table 2 shows the results for the patient-level outcomes according to data from the EHR. The PHQ-9 form was used for 1,048 (73.7%) patients with new depression and for 7,305 (45.6%) patients with any depression. Of those patients for whom the PHQ-9 form was used, 280 with new depression and 1,440 with any depression indicated possible suicidal ideation on their PHQ-9 form. For these patients, the suicide assessment form was completed for 67.9% of patients with new depression and for 62.0% of patients with any depression. Patient education handouts were used much less frequently—for 31 patients with new depression and 59 patients with any depression.
Of the 123 initial study providers, 112 were still in the study practices at the end of the study, and 110 (98.2%) of those completed the endpoint surveys. Table 3 shows the responses of these providers at the end of the study regarding their use of the CDS forms. Of these providers, 89% stated that they often used the PHQ-9 form for patients with new episodes of depression, and 78% stated that they often used the PHQ-9 for all patients with depression. Also, 79% of providers said they used the suicide assessment form. Providers were less likely to often use other components of the CDS forms, including treatment guidelines (42%) and screening for generalized anxiety disorder (34%) and bipolar disorder (25%). Most providers rarely or never used the provider education modules included in the CDS form. However, 85% of responding providers said they were likely to continue to use the CDS tool after the study was completed.
As shown in Table 4, there were some notable differences across provider characteristics in terms of how they reported use of key components of the form. The most striking differences were by provider specialty. Family medicine providers were significantly more likely than general internal medicine providers to report often using the components that screened for generalized anxiety disorder (44% vs 10%, P < .0001) and bipolar disorder (26% vs 2%, P < .0001). There was also a nonsignificant trend for family medicine providers to report more often using the PHQ-9 for patients with new depression compared to general internal medicine providers (95% vs 74%, P = .06). With regard to years in practice, providers in practice more than 10 years were significantly more likely to report often using the component that screened for bipolar disorder (35% vs 13%, P < .05).
We asked providers how and why they used the main components of the CDS tool—the PHQ-9 and suicide assessment forms. For patients with new episodes of depression, the most common reasons to use the PHQ-9 were to confirm the diagnosis and assess severity of depression. For patients with ongoing depression, the most common reasons were to monitor severity and determine recovery status (Table 5). The most common reason to use the suicide assessment form was when patients expressed thoughts of self-harm (77%) or as a result of their PHQ-9 scores (69%).
Click figure to enlarge
Table 6 shows providers’ opinions about whether different components of the CDS tool were helpful. The large majority of providers agreed or strongly agreed that the PHQ-9 and suicide risk assessment components were helpful in improving patient care (90% and 75%, respectively). An even higher proportion agreed or strongly agreed that these components were helpful in documenting patient care (93% and 86%, respectively). The other components were not viewed as helpful by most providers, with 44% saying that patient education helped to improve patient care and only 10% saying that provider education helped to improve patient care.
Click figure to enlarge
Finally, for the 105 providers who completed both the baseline and endpoint surveys, the percentage of providers reporting that they frequently use a standardized tool for diagnosing depression increased from 47% to 80% from before to after the study (P < .001). The percentage of providers reporting that they frequently use a standardized tool for monitoring depression increased from 27% to 85% (P < .001).
DISCUSSION
This study demonstrated the successful integration of a clinical decision support tool for management of depression in primary care settings.
National guidelines suggest that primary care providers should use standardized questionnaires to assess the severity of depression at initial diagnosis as well as to monitor the severity of depression over time.19,30 The providers in this study reported a dramatic increase in these recommended practices. From before to after the intervention, the proportion of providers that frequently used standardized tools to diagnose depression nearly doubled, and the proportion that frequently used these tools to monitor depression more than tripled.
The most widely used component of the form was the PHQ-9. Nearly 90% of study providers said that they often or almost always used the PHQ-9 for new episodes of depression, and nearly 80% said that they often or almost always used it for ongoing depression. The high use of the PHQ-9 reported by providers was supported by results from the EHR data; although these results cannot be directly compared since one represents provider rates and the other represents patient rates, the results were very consistent.
Providers used the PHQ-9 mainly to confirm the diagnosis and assess severity of new episodes of depression and to monitor depression over time, which is exactly what is recommended by national guidelines.24 Interestingly, about half also said they used the PHQ-9 to help convince patients that they were depressed. Nearly all providers said that the PHQ-9 form was helpful in improving the care of patients and had changed their practice. These data provide strong evidence that providers felt that the EHR-based CDS was successful in improving quality of care for depression as recommended by national guidelines, specifically use of standardized tools for diagnosis and monitoring of depression.
These findings are similar to what has been found in several other studies that implemented the PHQ-9 form in primary care offices. One study was conducted in a single office that implemented the Scantron version of the PHQ-9 into the Centricity EHR.27 That study demonstrated successful use of the form for depression screening, but providers also found the form helpful for determining remission.27
Another study was conducted in a national practice-based research network similar to the current study.31 In this study, all 16 participating offices implemented the PHQ-9 for diagnosing depression, and 13 offices implemented it for monitoring depression.31 Two years after the study was completed, the majority of offices continued to use the PHQ-9 for this purpose.32 However, the study did not examine the practice patterns for individual providers.
A study that did examine practices of individual providers began as a randomized controlled trial wherein nurse managers administered the PHQ-9 between office visits.33 After the randomized trial was completed, providers in both the intervention and control groups were given the PHQ-9 as part of their usual process of care. Three years later, 87% of providers said that they were “using the PHQ-9 as a goal to help assess depression diagnosis and severity.” These providers used the tool both for making an initial diagnosis (91%) and for providing routine follow-up care (76%); however, the study did not examine how often these providers used the PHQ-9.33
While these previous studies have demonstrated the utility of the PHQ-9 for depression care in primary care, they did not examine the other CDS tools that were included in our study. For example, our study showed that a suicide assessment form was widely used and was felt to be helpful in improving care. However, the provider and patient education components were not commonly used, and the provider education was not thought to be particularly helpful. It could be that providers felt comfortable with their knowledge of depression management but felt that they needed tools to put this knowledge into practice (such as the PHQ-9).
This study is also unique in that it examined clinical decision support that was incorporated into an EHR. Experts recommend that CDS tools be incorporated into EHRs whenever possible to facilitate the process of care.20,21 Also, one of the criteria for “meaningful use” of EHRs is the use of CDS tools.34 One previous study did incorporate CDS for depression into an EHR on the basis of PHQ-9 score results.35 However, the PHQ-9 was not directly linked to the EHR and was not used at the point of care. So, the PHQ-9 results could not be used to monitor treatment over time.35 The present study is the first to our knowledge to examine CDS tools for depression that are incorporated directly into the EHR.
Several limitations must be considered when interpreting the results of this study. First, most of the data come from provider reports, and providers may overestimate their behaviors in practice. However, we were also able to track use of the intervention through the EHR, and these patterns of use generally confirmed the provider responses. Second, while this study showed improvements in recommended processes of care, it did not examine outcomes of care for persons with depression. Since the PHQ-9 was implemented as part of the study, we were not able to compare depression severity from before to after the study or to compare the intervention to no intervention. Finally, there are limitations to how the results can be generalized. The study was conducted in a national practice-based research network of offices that use an EHR. While the national scope and wide variety of practices makes it more generalizable than studies in single practices or institutions, it could be that providers who participate in a practice-based research network and specifically those who agreed to participate in this study were more amenable than other providers to improvements in quality of care.
Despite these limitations, this study has significant implications for improving quality of depression care in primary care settings. The study suggests that EHR-based CDS can be useful in improving provider practice with respect to the key recommendations of national guidelines, which recommend using standardized severity tools for diagnosing and monitoring depression. Providers used these tools frequently, thought they were helpful in improving care with minimal disruption, and said they were likely to continue using the forms after the study was completed. These findings can help to guide national efforts to incorporate effective and efficient clinical decision support into primary care offices.
Author affiliations: Delaware Valley Outcomes Research, Newark (Dr Gill and Mss Chen and Grimes); Department of Family and Community Medicine, Thomas Jefferson University, Philadelphia, Pennsylvania (Drs Gill and Diamond); Department of Medical Informatics and Clinical Epidemiology, Oregon Health and Sciences University, Portland (Dr Lieberman); and Department of Family and Community Medicine and Department of Psychiatry, University of Michigan, Ann Arbor (Dr Klinkman).
Potential conflicts of interest: Dr Gill has served as a consultant and received grant/research support from GE Healthcare IT; Dr Lieberman was formerly an employee of GE Healthcare; and Dr Klinkman has served on the scientific advisory boards for Pfizer (formerly Wyeth). Mss Chen and Grimes and Dr Diamond report no conflicts of interest.
Funding/support: This study was funded by Wyeth.
Previous presentation: Some of the results were presented as a poster presentation at the North American Primary Care Research Group Annual Meeting; November 17, 2009; Montreal, Canada.
Acknowledgments: The authors thank the physicians and practices of the Medical Quality Improvement Consortium that participated in this study. They also thank the project manager, Katherine Rosch Hegedus, BSME, and Cheryl Mongillo, who assisted with manuscript preparation. Mss Rosch Hegedus and Mongillo are employees of DVOResearch, Newark, Delaware, and their work on the project was supported by Wyeth.
REFERENCES
1. Shim RS, Baltrus P, Ye J, et al. Prevalence, treatment, and control of depressive symptoms in the United States: results from the National Health and Nutrition Examination Survey (NHANES), 2005-2008. J Am Board Fam Med. 2011;24(1):33-38 PubMed.
2. Kessler RC, Berglund P, Demler O, et al; National Comorbidity Survey Replication. The epidemiology of major depressive disorder: results from the National Comorbidity Survey Replication (NCS-R). JAMA. 2003;289(23):3095-3105. PubMed doi:10.1001/jama.289.23.3095
3. Un×¼tzer J, Katon W, Sullivan M, et al. Treating depressed older adults in primary care: narrowing the gap between efficacy and effectiveness. Milbank Q. 1999;77(2):225-256, 174. PubMed doi:10.1111/1468-0009.00132
4. Klinkman MS, Okkes I. Mental health problems in primary care: a research agenda. J Fam Pract. 1998;47(5):379-384. PubMed
5. Ford DE. Managing patients with depression: is primary care up to the challenge? J Gen Intern Med. 2000;15(5):344-345. PubMed doi:10.1046/j.1525-1497.2000.03011.x
6. Gill JM, Klinkman MS, Chen YX. Antidepressant medication use for primary care patients with and without medical comorbidities: a National Electronic Health Record (EHR) Network Study. J Am Board Fam Med. 2010;23(4):499-508. PubMed
7. Rush WA, Whitebird RR, Rush MR, et al. Depression in patients with diabetes: does it impact clinical goals? J Am Board Fam Med. 2008;21(5):392-397. PubMed doi:10.3122/jabfm.2008.05.070101
8. de Groot M, Anderson R, Freedland KE, et al. Association of depression and diabetes complications: a meta-analysis. Psychosom Med. 2001;63(4):619-630. PubMed
9. Egede LE, Nietert PJ, Zheng D. Depression and all-cause and coronary heart disease mortality among adults with and without diabetes. Diabetes Care. 2005;28(6):1339-1345. PubMed
10. Carney RM, Freedland KE, Steinmeyer B, et al. Depression and five year survival following acute myocardial infarction: a prospective study. J Affect Disord. 2008;109(1-2):133-138. PubMed doi:10.1016/j.jad.2007.12.005
11. Frasure-Smith N, Lespérance F, Talajic M. Depression following myocardial infarction: impact on 6-month survival. JAMA. 1993;270(15):1819-1825. PubMed doi:10.1001/jama.270.15.1819
12. Jia H, Damush TM, Qin H, et al. The impact of poststroke depression on healthcare use by veterans with acute stroke. Stroke. 2006;37(11):2796-2801. PubMed doi:10.1161/01.STR.0000244783.53274.a4
13. Morris PL, Robinson RG, Samuels J. Depression, introversion and mortality following stroke. Aust N Z J Psychiatry. 1993;27(3):443-449. PubMed doi:10.3109/00048679309075801
14. Meyer HA, Sinnott C, Seed PT. Depressive symptoms in advanced cancer, pt 2: depression over time; the role of the palliative care professional. Palliat Med. 2003;17(7):604-607. PubMed doi:10.1191/0269216303pm813oa
15. Watson M, Haviland JS, Greer S, et al. Influence of psychological response on survival in breast cancer: a population-based cohort study. Lancet. 1999;354(9187):1331-1336. PubMed doi:10.1016/S0140-6736(98)11392-2
16. Solberg LI, Korsen N, Oxman TE, et al. The need for a system in the care of depression. J Fam Pract. 1999;48(12):973-979. PubMed
17. Rost K, Nutting P, Smith J, et al. The role of competing demands in the treatment provided primary care patients with major depression. Arch Fam Med. 2000;9(2):150-154. PubMed doi:10.1001/archfami.9.2.150
18. Nutting PA, Rost K, Smith J, et al. Competing demands from physical problems: effect on initiating and completing depression care over 6 months. Arch Fam Med. 2000;9(10):1059-1064. PubMed doi:10.1001/archfami.9.10.1059
19. Depression Guideline Panel. Depression in Primary Care: Treatment of Major Depression. Vol 2. AHCPR Publication No. 93-0551. Rockville, MD: US Department of Health and Human Services; 1993.
20. Institute of Medicine Committee on Quality of Health Care in America. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academy Press; 2001.
21. Berner ES. Clinical Decision Support Systems: State of the Art. AHRQ Publication No. 09-0069-EF. Rockville, MD: Agency for Healthcare Research and Quality; 2009.
22. Gill JM, Chen YX, Glutting JJ, et al. Impact of decision support in electronic medical records on lipid management in primary care. Popul Health Manag. 2009;12(5):221-226. PubMed doi:10.1089/pop.2009.0003
23. Gill JM, Landon BE, Antonelli RC, et al. Generating the knowledge needed to make the patient-centered medical home a reality: a collaborative project of the primary care specialties. Ann Fam Med. 2010;8(1):88-89. PubMed doi:10.1370/afm.1087
24. John D and Catherine T MacArthur Foundation. The MacArthur Initiative on Depression and Primary Care. http://www.depression-primarycare.org/about/about/. Accessed November 8, 2011.
25. Spitzer RL, Kroenke K, Williams JBW. Validation and utility of a self-report version of PRIME-MD: the PHQ primary care study. Primary Care Evaluation of Mental Disorders. Patient Health Questionnaire. JAMA. 1999;282(18):1737-1744. PubMed doi:10.1001/jama.282.18.1737
26. Whooley MA, De Jonge P, Vittinghoff E, et al. Depressive symptoms, health behaviors, and risk of cardiovascular events in patients with coronary heart disease. JAMA. 2008;300(20):2379-2388. PubMed
27. Klein EW, Hunt JS, Leblanc BH. Depression screening interfaced with an electronic health record: a feasibility study in a primary care clinic using optical mark reader technology. Prim Care Companion J Clin Psychiatry. 2006;8(6):324-328. PubMed doi:10.4088/PCC.v08n0601
28. Lin EHB, Heckbert SR, Rutter CM, et al. Depression and increased mortality in diabetes: unexpected causes of death. Ann Fam Med. 2009;7(5):414-421. PubMed doi:10.1370/afm.998
29. Yawn BP, Pace W, Wollan PC, et al. Concordance of Edinburgh Postnatal Depression Scale (EPDS) and Patient Health Questionnaire (PHQ-9) to assess increased risk of depression among postpartum women. J Am Board Fam Med. 2009;22(5):483-491. PubMed doi:10.3122/jabfm.2009.05.080155
30. US Preventive Services Task Force. Screening for depression: recommendations and rationale. Am Fam Physician. 2002;66(4):647-650. PubMed
31. Nease DE Jr, Nutting PA, Dickinson WP, et al. Inducing sustainable improvement in depression care in primary care practices. Jt Comm J Qual Patient Saf. 2008;34(5):247-255. PubMed
32. Nease DE Jr, Nutting PA, Graham DG, et al. Sustainability of depression care improvements: success of a practice change improvement collaborative. J Am Board Fam Med. 2010;23(5):598-605. PubMed doi:10.3122/jabfm.2010.05.090212
33. Lee PW, Dietrich AJ, Oxman TE, et al. Sustainable impact of a primary care depression intervention. J Am Board Fam Med. 2007;20(5):427-433. PubMed doi:10.3122/jabfm.2007.05.070045
34. Office of the National Coordinator for Health Information Technology (ONC). Health Information Technology: Initial Set of Standards, Implementation Specifications, and Certification Criteria for Electronic Health Record Technology: Final Rule. Vol 75:8: Department of Health and Human Services, 2010:45 CFR Part 170. http://healthit.hhs.gov/portal/server.pt/community/healthit_hhs_gov__standards_ifr/1195. Accessed November 8, 2011.
35. Rollman BL, Hanusa BH, Lowe HJ, et al. A randomized trial using computerized decision support to improve treatment of major depression in primary care. J Gen Intern Med. 2002;17(7):493-503. PubMed doi:10.1046/j.1525-1497.2002.10421.x


