Pharmacologic Treatment of Dimensional Anxious Depression: A Review
ABSTRACT
Objective: To review the pharmacologic treatment of dimensionally defined anxious depression.
Data Sources: English-language, adult human research articles published between 1949 and February 2013 were identified via PUBMED and EMBASE. The search term was treatment of anxious depression.
Study Selection: We identified and reviewed 304 original articles. Of these, 31 studies of patients with anxious depression, who were treated with an antidepressant or antipsychotic, are included in this review.
Data Extraction: All studies explicitly used a dimensional definition of anxious depression. All patients were treated with either antidepressants or antipsychotic medications.
Results: Of the 31 relevant psychopharmacologic studies identified, 7 examined patients receiving only 1 medication, 2 studied cotherapeutic strategies, 1 examined antipsychotic augmentation, and 21 compared multiple medications. Eleven were pooled analyses from several studies. All studies were of adults (18-92 years old). The Hamilton Depression Rating Scale Anxiety/Somatization Factor Score was used to define anxious depression in 71% of the studies, and 77.4% were post hoc analyses of previous datasets. Seventeen studies found selective serotonin reuptake inhibitors (SSRIs), serotonin-norepinephrine reuptake inhibitors (SNRIs), and/or tricyclic antidepressants (TCAs) to be useful for successfully treating anxious depression. However, patients with anxious depression were less likely to experience sustained response or remission. Furthermore, baseline anxious depression puts patients at greater risk for side effect burden.
Conclusions: Despite achieving response with SSRIs, SNRIs, and TCAs, patients with dimensionally defined anxious depression do not maintain response or remission and often report a larger burden of side effects compared to nonanxious depressive patients, suggesting that it is a harder-to-treat subtype of major depressive disorder.
Prim Care Companion CNS Disord 2014;16(3):doi:10.4088/PCC.13r01621
© Copyright 2014 Physicians Postgraduate Press, Inc.
Submitted: December 20, 2013; accepted February 5, 2014.
Published online: May 29, 2014.
Corresponding author: Dawn F. Ionescu, MD, Bldg 10, CRC Room 7-5545, 10 Center Drive, MSC 1282, Bethesda, MD 20892 ([email protected]).
Subtyping in major depressive disorder (MDD) is critical for improving the classification, diagnosis, and treatment of psychiatric disease. In particular, anxious depression is a topic of clinical interest, as it is common, affecting approximately 50% of patients with MDD.1 Certainly, increasing interest in further classifying the effects of anxiety within depression is evident through the recent addition of the “anxious distress” specifier to the diagnosis of MDD in the newly published Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5).2 In particular, understanding clinical biomarkers (ie, subtyping MDD) allows for stratification of patients early in the disease process—a step critical for predicting treatment response to antidepressant therapies.3 Importantly, patient stratification moves toward the personalization of psychiatric treatments, with the ultimate goal of rapidly improving depression through the prescribing of patient-specific drug regimens.
In particular, anxious depression is clinically thought to be a more difficult-to-treat subtype of MDD. Dimensionally defined anxious depression is associated with greater symptom severity, worse functioning, and/or poorer treatment outcomes in some,1,4,5 but not all,6-9 studies. For example, 1 naturalistic study found that patients with anxious depression had an overall worse response to a wide range of antidepressants (including selective serotonin reuptake inhibitors [SSRIs] and serotonin-norepinephrine reuptake inhibitors [SNRIs]), longer treatment response latency, and smaller reduction of symptoms.10 In another naturalistic study, anxious depressive patients took twice as long to recover from depressive episodes compared to nonanxious depressive patients.11 Conversely, a recent naturalistic study did not find that anxious depression predicted worse outcomes for a variety of antidepressant treatments.7
Such conflicting results may be due, in part, to the heterogeneity used to define anxious depression throughout the literature—indeed, the criteria used to define anxious depression varies frequently among studies, though the term itself stays constant.12 For example, anxious depression has been defined dimensionally (as MDD plus anxiety symptoms, often quantified on a rating scale), syndromally (as MDD plus and anxiety disorder), and as mixed-anxiety depressive disorder (a term reserved for symptoms of depression and anxiety that do not meet full criteria for either disorder). Such heterogeneity in the definitions makes it difficult to draw firm conclusions. In order to avoid intertwining various conceptualizations of anxious depression, this article will use the more stringent criteria associated with dimensionally defined anxious depression.
Despite disagreement within the literature as to whether meaningful treatment differences exist between anxious and nonanxious depressive patients, the treatment of anxious depression is an important clinical concern. Therefore, given that dimensionally defined anxious depression is clinically common, this article will review the literature on the efficacy and tolerability of pharmacologic treatments for dimensionally defined anxious depression.

- Anxiety within depression is a common clinical finding.
- Although patients with anxious depression may be successfully treated with selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, and tricyclic antidepressants, they do not stay well as long as their nonanxious counterparts and are more likely to experience a greater burden of side effects.
METHOD
Using the search term treatment of anxious depression, 144 articles published between 1949 and February 2013 were identified via PubMed. The same search via EMBASE revealed 160 articles. This strict search term was used to identify studies that focused only on the treatment of anxious types of depression. In this way, articles pertaining to the treatment of general MDD and other subtypes of depression (ie, atypical, melancholic) were excluded. On the basis of a review of the titles and abstracts of all 304 articles, 31 psychopharmacologic studies of patients with unipolar MDD receiving antidepressants or antipsychotics were identified for inclusion in the present review (Table 1). All articles were English-language, peer-reviewed, published studies (age range of patients was 18-92 years). No case reports were included.
Click figure to enlarge
Click figure to enlarge
Click figure to enlarge
Click figure to enlarge
All studies explicitly used a dimensional definition of anxious depression, particularly because treatment response for patients with dimensional anxious depression has been suggested to be worse than for patients with nonanxious depression.4,5,10,11 Specifically, all subjects were diagnosed with MDD on the basis of DSM or International Classification of Diseases criteria plus significant anxiety as measured by a clinician-rated scale. For instance, a typical definition might encompass a DSM diagnosis of MDD plus a score ≥ 7 on the Hamilton Depression Rating Scale (HDRS) Anxiety/Somatization Factor Score (A/S).13 The HDRS A/S consists of 6 items from the 17- or 21-item HDRS (psychic anxiety, somatic anxiety, somatic symptoms [gastrointestinal], somatic symptoms [general], hypochondriasis, and insight) and was first derived from a factor analysis of the 17-item HDRS.13 Particular emphasis was placed on searching for articles that used the HDRS A/S, as it has been shown to be useful for both clinical and research settings,14 allowing for the seamless translation of research results into clinical practice. Of note, a previous review discussed treatments for syndromally defined anxious depression, defined as MDD plus an anxiety disorder.15 In the current review, findings are broadly organized by medication class.
RESULTS
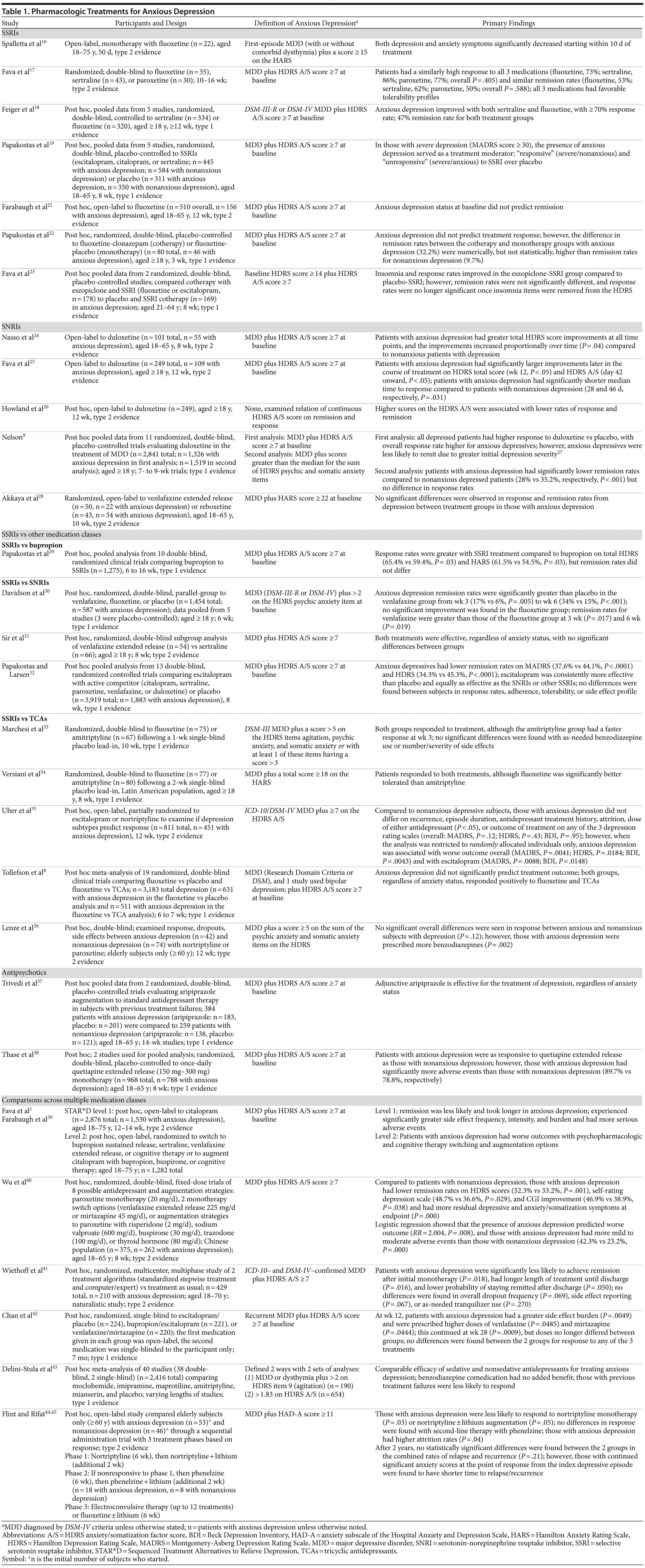
Of the 31 relevant psychopharmacologic studies exploring the treatment of anxious depression, 11 were open-label,1,16,21,24-26,28,35,39,44,45 17 were randomized and double-blind,8,9,17-19,22,23,29-34,36-38,40 1 was randomized and single-blind,42 1 was a pooled study that mixed single- and double-blind studies,43 and 1 used a treatment algorithm.41 Seven studies examined only 1 medication,9,16,21,24-26,38 2 studied cotherapeutic strategies,22,23 1 examined antipsychotic augmentation,37 and 21 compared multiple medications.1,8,17-19,28-36,39-45 Eleven were pooled analyses from several studies,8,9,18,19,23,29,30,32,37,38,43 71% used the HDRS A/S to define anxious depression,1,8,9,17-19,21-26,29,31,32,35,37-42 and 77.4% were post hoc analyses of previous datasets.1,8,9,18,19,21-23,26,29-32,35-45
Seven studies examined only SSRIs,16-19,21-23 1 compared SSRIs with bupropion,29 3 compared SSRIs to SNRIs,30-32 and 5 compared SSRIs to tricyclic antidepressants (TCAs).8,33-36 Five studies examined SNRIs alone.9,24-26,28 One study investigated antipsychotic monotherapy,38 and another examined antipsychotic augmentation for the treatment of anxious depression.37 Eight studies made comparisons across multiple medication classes.1,39-45
SSRI Studies
Several studies found that SSRIs successfully treated anxious depression. Spalletta and colleagues16 evaluated open-label monotherapy with fluoxetine for first-episode anxious depression (n = 22). Significant score improvements from baseline were observed on the HDRS (P < .0001) and Hamilton Anxiety Rating Scale (HARS; P < .0005) in response to treatment, mostly within 10 days.16
Another study compared the efficacy and tolerability of 3 different SSRIs (fluoxetine, n = 35; sertraline, n = 43; and paroxetine, n = 30) for the treatment of anxious depression in outpatients.17 Response rates and remission rates were ≥ 50% for all 3 treatments, with a low frequency of adverse events. Another study pooled results of 5 trials examining the antidepressant efficacy of sertraline (n = 334) or fluoxetine (n = 320) in outpatients with anxious depression.18 Post hoc analyses found that both antidepressants similarly improved several outcome measures (HDRS total score and Clinical Global Impressions [CGI] scores); ≥ 70% of patients achieved response (≥ 50% reduction from baseline HDRS A/S score), and 47% achieved remission.18
Another study reanalyzed data from 5 different trials examining the efficacy of SSRIs (escitalopram, citalopram, sertraline) in 1,690 patients with MDD, of which 756 had anxious depression.19 SSRI treatment was superior to placebo in treating those with severe anxious depression (Montgomery-Asberg Depression Rating Scale [MADRS] score ≥ 30) on the basis of change in MADRS score (P = .0414) and response rates (P = .0173) but not remission rates. In contrast, patients with severe nonanxious depression showed significant improvements on all 3 measures (all: P < .0001). Interestingly, using change in MADRS scores to measure outcome, the presence or absence of anxious depression did not serve as a treatment moderator of SSRI efficacy over placebo. However, when patients with severe depression were analyzed separately, anxiety status did serve as a treatment moderator, so that the efficacy of SSRI treatment was superior to placebo only for severe nonanxious depression.19
A previous study found that early improvements (within 1 week) in the somatic symptoms (general) item of the HDRS A/S predicted higher remission rates for fluoxetine or St. John’s wort extract (hypericum perforatum), but not placebo, in 135 patients with MDD.20 This finding led the authors to further examine the post hoc relationship between anxious depression at baseline and treatment response using data from MDD patients with anxious depression from a trial of fluoxetine.21 Anxious depression status at baseline did not predict remission at endpoint (odds ratio: 0.989, P = .97). However, remitters (with either anxious or nonanxious MDD) had significantly greater early reductions (between baseline and week 1) in the HDRS A/S somatic symptoms (gastrointestinal) item (P = .006) compared to nonremitters. 21
Two post hoc SSRI studies explored the benefits of cotherapy. The first compared fluoxetine-clonazepam versus fluoxetine-placebo in anxious (n = 46) and nonanxious (n = 34) depression in a 3-week trial.22 Again, anxious depression status did not predict improvement in response to treatment. However, the difference in remission rates between cotherapy and monotherapy in patients with anxious depression (32.2%) was numerically, but not statistically, higher than remission rates for patients with nonanxious depression (9.7%). The other cotherapy study compared the efficacy of eszopiclone-SSRI (fluoxetine or escitalopram, n = 178) versus SSRI-placebo (n = 169) for the treatment of comorbid insomnia and anxious depression using pooled data from 2 clinical trials.23 Insomnia rates significantly improved from baseline for the eszopiclone group compared to the placebo group. Response rates on the HDRS were greater for the eszopiclone group than for the placebo group (55.6% vs 42%, respectively, P = .01); however, this difference was no longer significant when insomnia items were removed.23
SNRI Studies
Duloxetine has been studied by several groups as a putative treatment for anxious depression. One 8-week study examined clinical and demographic predictors of response to duloxetine in 101 outpatients with MDD, 55 of whom had anxious depression.24 Anxious depressive patients showed greater improvements at all points as measured by total HDRS score, and the improvements increased proportionally over time (P = .04) compared to nonanxious depressive patients. Another trial compared the efficacy and tolerability of open-label duloxetine between outpatients with anxious (n = 109) and nonanxious (n = 140) depression.25 Compared to nonanxious depressive patients, those with anxious depression had significantly larger improvements later in the course of treatment as measured by HDRS total (week 12, P < .05) and HDRS A/S (day 42 onward, P < .05) scores, but no differences were found between HARS or CGI-S scores. Those with anxious depression had a significantly shorter median time to response compared to those with nonanxious depression (28 vs 46 days, respectively, P = .031), although remission and response rates at endpoint were similar. General safety and tolerability between the groups were similar.25
Interestingly, another post hoc analysis of the same dataset found that higher HDRS A/S scores were associated with lower rates of response and remission when continuous scores were examined.26 Although previous findings from this dataset showed that patients with anxious depression had larger improvements and shorter time to response with duloxetine treatment,25 using the HDRS A/S as a continuous score suggests that patients with more severe and complicated depression had a less robust treatment response.
In another post hoc examination of duloxetine for the treatment of anxious depression, 1 study pooled data from 11 trials, with lengths ranging from 7 to 9 weeks.9 Of the 2,841 total patients randomized, 1,326 met criteria for anxious depression. Response rates to duloxetine were higher than placebo in both groups, with the overall response rate being significantly higher in anxious compared to nonanxious depressed patients (44% vs 41%, respectively, P < .001). However, anxious depressive patients were less likely to experience remission than nonanxious patients (27.5% vs 34.7%, respectively, P < .001), although the author later concluded that this result was due to greater severity of initial depression.27 Notably, a secondary analysis of the data (anxious depression defined as MDD plus combined HDRS psychic anxiety and somatic anxiety item scores greater than the median) found that 1,519 patients met criteria for anxious depression. Compared to nonanxious patients, anxious subjects had significantly lower remission rates (35.2% vs 28%, respectively, P < .001) but no difference in response rates.
A Turkish study compared the efficacy and tolerability of venlafaxine extended release (venlafaxine extended release [XR]) to reboxetine (a norepinephrine reuptake inhibitor not approved for use in the United States) in the treatment of depressed patients over 10 weeks.28 Fifty (22 with anxious depression) patients were randomized to open-label venlafaxine XR, and 43 (34 with anxious depression) were randomized to reboxetine. No significant differences were observed in response and remission rates from depression between treatment groups in those with anxious depression.28
SSRIs Versus Other Medication Classes
Several studies compared SSRIs to other classes of medications:
SSRIs versus bupropion. Papakostas and colleagues29 performed a post hoc meta-analysis on 10 studies comparing the efficacy of bupropion, a norepinephrine and dopamine reuptake inhibitor, with SSRIs (escitalopram, fluoxetine, sertraline, and paroxetine) for the treatment of anxious depression (n = 1,275). Response rates were greater with SSRI treatment compared to bupropion on the basis of total scores from the HDRS (65.4% vs 59.4%, respectively, P = .03) and HARS (61.5% vs 54.5%, respectively, P = .03); however, remission rates did not differ.29
SSRIs versus SNRIs. A post hoc analysis of pooled data from 5 trials compared the efficacy of venlafaxine (n = 542) to fluoxetine (n = 555) or placebo (n = 357) in 1,454 outpatients with MDD.30 “Severe” anxious depression was quantified by a baseline score > 2 on the HDRS psychic anxiety item (n = 587). Remission rates in this group were significantly greater for venlafaxine compared to placebo from week 3 (17% vs 6%, respectively, P = .005) to week 6 (34% vs 15%, respectively, P < .001). No significant improvement was found in the fluoxetine group, and remission rates for venlafaxine were greater than those in the fluoxetine group at 3 (P = .017) and 6 weeks (P = .019).30
In contrast, a post hoc subgroup analysis of an 8-week study comparing venlafaxine XR (n = 54) to sertraline (n = 66) found that both treatments similarly improved symptoms of anxious depression.31 The HDRS response rates for sertraline and venlafaxine XR were 79.6% and 68.9%, respectively (P = .26); remission rates (63% vs 54.1%, P = .44) were similar between treatment groups.31
Another post hoc study examined the efficacy of escitalopram in treating anxious depression and pooled individual patient data from 13 trials.32 Of 3,919 individuals with MDD, 1,883 were classified as having anxious depression; 858 were treated with escitalopram, 714 were treated with active competitor (citalopram, sertraline, paroxetine, venlafaxine, or duloxetine), and 311 were treated with placebo. Escitalopram was consistently more effective than placebo and equally as effective as the SNRIs or other SSRIs in the treatment of anxious depression. No differences were found in response rates, adherence, tolerability, or side effect profile between patients with anxious and nonanxious depression. However, patients with anxious depression had lower overall remission rates as measured by the MADRS (37.6% vs 44.1%, respectively, P < .0001) and HDRS (34.3% vs 45.3%, respectively, P < .0001).32
SSRIs versus TCAs. In one 10-week study, anxious depressive patients were randomized to receive fluoxetine (n = 75) or amitriptyline (n = 67) in a double-blind fashion following a 1-week, single-blind placebo trial.33 Both medication groups showed a comparable response (67.1% vs 78.6%, based on the HDRS); however, the amitriptyline group showed a significantly faster reduction in scores at week 3 compared to the fluoxetine group (mean ± SD score reductions of 17.3 ± 6.2 vs 14.7 ± 6.3, respectively, P = .02). The groups did not differ significantly in the number or severity of side effects observed. Notably, the dose of fluoxetine used was low, and the protocol allowed for use of bromazepam (a benzodiazepine) as needed for severe agitation and anxiety; its use, dosage, and duration did not differ between groups.33
A similar study randomized Latin American patients to fluoxetine (n = 77) or amitriptyline (n = 80) for up to 8 weeks.34 Though both groups had similar reductions in HDRS and HARS total scores from baseline, the amitriptyline group showed a significantly greater improvement than the fluoxetine group for only 1 score: the HDRS sleep factor (P < .001), which comprises the early, middle, and late insomnia items. Positive response rates were seen among patients in the fluoxetine (74%) and amitriptyline (74.4%) medication groups, although the amitriptyline group reported significantly more side effects.34
A post hoc analysis of a 12-week trial examined whether subtypes of depression predicted treatment response to escitalopram or nortriptyline.35 Of the 811 patients, 451 met criteria for anxious depression. These patients received either escitalopram (n = 233 randomly, n = 225 nonrandomly) or nortriptyline (n = 235 randomly, n = 118 nonrandomly; specifically, if patients had a contraindication to one of the medications, they were nonrandomly assigned to the other antidepressant). Patients with anxious depression did not differ from those with nonanxious depression on measures of recurrence, episode duration, antidepressant treatment history, attrition, dose of either antidepressant, or treatment outcome as measured by 3 depression rating scales (MADRS, P = .12; HDRS, P = .43; Beck Depression Inventory [BDI], P = .95). However, when the analysis was restricted to randomly allocated individuals only, anxious depression was associated with worse outcome overall (MADRS, P = .0041; HDRS, P = .0184; BDI, P = .0043) and especially worse outcomes in those treated with escitalopram (MADRS, P = .0088; BDI, P = .0148).35
A large post hoc meta-analysis of 19 trials compared fluoxetine versus placebo and fluoxetine versus TCAs.8 Of the 3,183 subjects with MDD, 631 in the fluoxetine versus placebo analysis and 511 in the fluoxetine versus TCAs analysis met criteria for anxious depression. Regardless of anxiety status, depressed subjects responded positively to active treatment; fluoxetine and TCAs were similarly effective. In this study, anxious depression did not significantly predict treatment outcome. Note, this study allowed for a heterogeneous definition of depression, including MDD defined using Research Domain Criteria or DSM criteria; 1 trial allowed for bipolar depression.8
In a study of medication effects in the elderly (age ≥ 60 years), anxious (n = 42) and nonanxious (n = 74) patients with depression were randomly assigned to double-blind treatment with nortriptyline or paroxetine.36 A post hoc analysis revealed no significant differences in overall response rates between patients with anxious and nonanxious depression (71% vs 57%, respectively, P = .12) or in response rates with nortriptyline (81% vs 75%, respectively), time to response with nortriptyline (2 vs 4.5 weeks), response rates with paroxetine (60% vs 67%, respectively), or time to response with paroxetine (7 vs 4 weeks, respectively). No differences were found in terms of dropout rates (38% vs 46%, respectively); most dropouts occurred secondary to side effects. However, individuals with anxious depression were prescribed significantly more lorazepam (64% vs 34%, respectively, P = .002) for sleep and anxiety.36
Antipsychotic Studies
In order to determine the efficacy and safety of aripiprazole augmentation to standard antidepressant therapy in MDD subjects with previous treatment failures, Trivedi and colleagues37 pooled data from 2 trials. In this analysis, 384 patients with anxious depression (aripiprazole, n = 183; placebo, n = 201) were compared to 259 patients with nonanxious depression (aripiprazole, n = 138; placebo, n = 121). In both groups, adjunctive aripiprazole was effective and well tolerated. Beginning at weeks 1 or 2 and continuing through the remainder of the study, patients with anxious depression receiving aripiprazole had significantly greater improvements in total MADRS score compared to patients receiving placebo (−8.72 vs −6.17, P ≤ .001), a result similarly significant in the nonanxious depression group (−8.61 vs 4.97, P ≤ .001). Adverse event profiles did not differ.37
Two studies were pooled in a post hoc analysis (n = 968) to investigate once-daily quetiapine extended-release monotherapy for the treatment of MDD.38 Anxious depression accounted for 81.4% (n = 788) of the sample at baseline. Patients with anxious depression responded equally well to quetiapine XR but had a greater incidence of adverse events (89.7% vs 78.8%).
Comparisons Across Multiple Medication Groups
Several large trials have compared multiple medication classes for the treatment of anxious depression. In particular, the Sequenced Treatment Alternatives to Relieve Depression (STAR*D) study is one of the most comprehensive antidepressant treatment studies completed to date.1,39 In level 1 of STAR*D, outpatients with MDD received citalopram (n = 2,876). Post hoc analysis revealed that those with anxious depression (n = 1,530) experienced significantly greater side effect frequency, intensity, and burden and had more serious adverse events than those with nonanxious depression. In level 2, those who did not remit with or tolerate citalopram in level 1 were randomly switched to sustained-release bupropion, sertraline, or venlafaxine XR or to continued citalopram plus augmentation with sustained-release bupropion or buspirone. Level 2 subjects could also be switched to depression-focused cognitive therapy as an augmentation strategy or as monotherapy. Again, patients with anxious depression did worse with switching and augmentation options, suggesting that anxious depression is a negative predictor of outcome for treatments with psychopharmacologic or cognitive therapy interventions.1,39
In order to replicate and confirm the previous findings that anxious depression is associated with poorer treatment outcomes,1 Wu and colleagues40 examined data from Chinese patients with treatment-resistant depression enrolled in trials of a variety of antidepressant and augmentation treatment strategies. This post hoc study compared the efficacy and tolerability of 8 possible treatment groups. Of the 375 depressed patients, 262 had anxious depression, and treatment strategies were evenly distributed between groups. Compared to those with nonanxious depression, patients with anxious depression had lower remission rates as assessed by the HDRS (52.3% vs 33.2%, P = .001), lower ratings on self-rating depression scales (48.7% vs 36.6%, P = .029), less improvement in symptoms on the CGI (46.9% vs 38.9%, P = .038), and more residual depressive and anxiety/somatization symptoms at endpoint (P = .000). Logistic regression showed that anxious depression predicted worse outcome (RR = 2.004, P = .008); compared to those with nonanxious depression, anxious depressive patients had more mild to moderate adverse events (23.2% vs 42.3%, P = .000).40
The German Algorithm Project, phase 3 (GAP3) was part of a randomized controlled multicenter multiphase study that evaluated 2 different treatment algorithms (standardized stepwise drug treatment regimen and computerized decision-making/expert opinion) with treatment as usual in inpatients with MDD.41 Patients in the standardized stepwise drug treatment regimen could be treated with sertraline, venlafaxine, reboxetine, or amitriptyline monotherapy at the physician’s discretion. Within this group, 1 of 3 “second-step strategies” (lithium augmentation, high-dose monotherapy, or antidepressant switch) was compared in patients nonresponsive to monotherapy after 4 weeks of treatment. A computerized decision/expert system suggested continuing or changing the present strategy on the basis of a probability matrix from individual patient response data. Post hoc analysis of the 429 total MDD patients in GAP3 revealed that 210 had anxious depression. Compared to patients with nonanxious depression, those with anxious depression in the standardized stepwise drug treatment regimen were significantly less likely to achieve remission after initial monotherapy (P = .018), had longer length of treatment until discharge (59.16 ± 40.51 days vs 50.25 ± 35.54 days; P = .016), and had lower probability of maintaining remission after discharge (73% vs 82%, P = .050). No differences were found in overall dropout frequency, side effect reporting, or as-needed tranquilizer use.41
Another post hoc analysis compared treatment outcomes and side effect burden between outpatients with anxious (n = 497) and nonanxious (n = 168) depression from the Combining Medications to Enhance Depression Outcomes (CO-MED) study.42 Patients were randomized to escitalopram plus placebo (n = 224), sustained-release bupropion plus escitalopram (n = 221), or venlafaxine XR plus mirtazapine (n = 220), with escalating doses based on acceptable side effects. At week 12, patients with anxious depression had a greater side effect burden (P = .0049) and were prescribed higher doses of venlafaxine (P = .0485) and mirtazapine (P = .0444) than subjects with nonanxious depression. The increased side effect burden continued through week 28 in patients with anxious depression compared to their nonanxious counterparts (P = .0009), but doses no longer differed. Nevertheless, despite having greater severity of symptoms at baseline (P < .0001), more baseline melancholic and lethargic symptom features (P < .0001), worse cognitive functioning (P = .0001), lower quality of life (P = .0008), and poorer work and worse social adjustment (P = .0017) than patients with nonanxious depression, no differences were found between the groups in response or drop-out rates to any of the 3 treatments.42
A large, post hoc meta-analysis of 40 studies (n = 2,416) compared moclobemide, imipramine, maprotiline, amitriptyline, mianserin, and placebo for the treatment of anxious depression.43 Of particular note, the authors defined anxious depression the following 2 ways: (1) MDD (or dysthymia in 1 study) plus a score > 2 on the HDRS agitation item (n = 190) or (2) a baseline score > 1.83 on the HDRS A/S (“high” agitation group based on the upper third of responses, n = 654). Response to antidepressant treatment between high and low agitation groups was statistically insignificant using either definition, although there was a clear superiority of treatment over placebo. However, the high agitation group had significantly lower response to placebo. In all groups, previous treatment resistance significantly reduced the likelihood of response to therapy.43
Notably, 2 post hoc studies examined various medications for the treatment of anxious depression in elderly subjects (≥ 60 years old).44,45 One open-label study found that, compared to those with nonanxious depression (n = 46), patients with anxious depression (n = 53) were less likely to respond to nortriptyline monotherapy (P = .03), a difference that remained significant after 2 additional weeks of adjunctive lithium for those who failed to respond to nortriptyline alone (P = .05). This difference did not remain significant in the second part of the study, in which treatment-resistant patients were given phenelzine with or without lithium augmentation.44 In the overall study, those with anxious depression had higher attrition rates (P = .04). The investigators then examined outcome over a 2-year follow-up period.45 No statistically significant differences were found between the 2 groups in combined rates of relapse and recurrence; however, those with continued significant anxiety scores at the point of response from the index depressive episode had shorter times to relapse/recurrence (P = .001).
CONCLUSIONS
As reviewed previously, research has shown that patients with dimensionally defined anxious depression may be successfully treated with several drug classes, including SSRIs,8,16-19,23,29,31-34,36 SNRIs,9,24,25,28,30-32 and TCAs.8,33,34,36 However, studies have also noted that patients with anxious depression often do not experience sustained response or remission following initial successes in treatment,1,9,32,39-41 and that baseline anxious depression may put patients at greater risk for side effects.1,38-40,42 In particular, large studies comparing multiple medication classes and treatment modalities found that patients with anxious depression had overall poorer treatment outcomes than depressed patients without anxiety.1,38-41 These large studies highlight the important treatment differences between patients with anxious and nonanxious depression that may not be evident in smaller, open-label studies.
Despite overall poorer outcomes, clinicians will be faced with the challenge of successfully treating patients with anxious depression. As noted previously, studies have shown SSRIs to be effective treatments.8,16-19,23,29,31-34,36 Regarding SNRIs, patients with anxious depression showed greater improvements than those with nonanxious depression in open-label24,25 and placebo-controlled duloxetine trials.9 Only 1 study showed that SNRIs were clearly superior to SSRIs in treating anxious depression,30 in contrast to 2 studies that found both medication classes to be equally effective, with no advantage for SNRI over SSRI use.31,32 It should also be noted that, given their clinical effectiveness and relatively favorable safety profile compared to TCAs, SSRIs and SNRIs should both be considered first-line treatments for anxious depression. Even though patients with anxious depression may experience initial responses, clinicians should prepare for earlier relapses and higher reports of side effects.
Possible explanations for why patients with anxious depression have poorer overall outcomes may be because they represent a harder-to-treat clinical population. It has been suggested that anxious patients with depression may have increased residual anxiety following treatment, in addition to having more sensitivity to somatic sensations, leading to a higher side effect burden.1 Also, patients with anxious depression are characterized by having more physical illness, lower socioeconomic status, greater severity of depression, and later onset of depression,1,41 all of which may be implicated in poorer treatment outcomes. Additionally, anxious depressive patients may have poorer outcomes due to higher baseline depressive symptoms,27 although most studies control for baseline differences in their analyses.
Although clinical relevance is limited at this time, literature from naturalistic genetics research may provide some insights into the differences in treatment response between anxious and nonanxious depressive patients. For example, although no overall impact of the norepinephrine transporter (NET) or serotonin transporter (5-HTT) genes were found for antidepressant treatment response in MDD, 1 study reported that, when stratified for anxious depression, a significant detrimental effect of the less active serotonin transporter-linked promoter region haplotypes (5-HTTLPR S allele [P = .007] and 5-HTTLPR/5-HTT rs25531 [P = .049]) was found for treatment response in patients with anxious depression.46 Another naturalistic treatment study found that patients with anxious depression who carried the less active neuropeptide Y (NPY) rs16147 −399C allele responded more slowly to antidepressants after 2 weeks and failed to achieve remission after 4 weeks of treatment.47 Similarly, the rarer T allele of the rs10473984 single-nucleotide polymorphism (SNP) within the corticotropin-releasing hormone binding protein (CRHBP) gene was associated with poorer treatment outcomes with citalopram.48 The brain-derived neurotrophic factor (BDNF) rs7124442 TT genotype has also been related to worse treatment outcomes after 6 weeks in subjects with MDD, particularly those with anxious depression.49 The use of genetic biomarkers for stratifying depression subtypes may ultimately lead to improved treatment outcomes in the future.
Regarding anxious depression as a predictor of short-term treatment outcome, 6 studies found that delineating anxious from nonanxious depression is not of particular use.8,9,19,21,22,35 However, 1 study did find that in patients with severe depression (MADRS score ≥ 30), anxious depression served as a response moderator for SSRIs compared to placebo, in that responsive patients were diagnosed with nonanxious MDD, and unresponsive patients were more likely to have anxious depression—a result that was only found when severity of depression was taken into account.19 In addition, a large Chinese study found that a diagnosis of anxious depression predicted worse outcome.40 Of utmost clinical importance, several studies indicated that baseline anxious depression may increase the risk of side effects.1,38-40,42 Certainly, anxious depression may serve as a useful predictor for risk of side effect burden, if not also for treatment outcomes, in some cases. Larger investigations into this topic are warranted.
Several limitations deserve mention. For one, most (77.4%) of the articles reviewed were post hoc analyses of datasets generated for other primary studies. Although studies of this nature are important, this highlights the critical need for future a priori explorations into the treatment of anxious depression. Another key concern is that the term anxious depression suffers from inherent problems with heterogeneity of definitions.12 Even within this review of studies carefully limited to dimensionally defined anxious depression, definitions between studies often varied. For example, although most studies (71%) employed the HDRS A/S definition,1,8,9,17-19,21-26,29,31,32,35,37-42 other studies chose to examine only certain items from the HDRS or HDRS A/S,30,33,36,43 or required certain cutoffs on the HARS16,28,34 or the anxiety subscale of the Hospital Anxiety and Depression Scale.44,45 While these definitions certainly share some similarities, such variation makes it difficult to draw strong conclusions when making comparisons across studies. In addition, categorical anxious depression, defined as MDD plus and anxiety disorder, is another important way of defining this concept. Omitting this type of anxious depression from the review may inherently miss important treatment discussions. (For a review of the treatment of categorical anxious depression, see the discussion by Pollack.15) Certainly, further expanding the search term beyond treatment of anxious depression may produce an even larger yield than reviewed in this article.
A recent review of the neurobiology of anxious depression found that those with dimensionally defined anxious depression may differ from those with nonanxious depression in some neurobiological aspects, including heightened hemispheric asymmetries.50 Taken together with the evidence reviewed herein that anxious depression may be more difficult to treat than nonanxious depression, these data may provide evidence that anxious depression may be an important subtype of MDD. The diagnostic and treatment implications of this distinction are critical to both clinicians and researchers alike and underscore the need for future studies. In particular, a priori hypothesis-driven studies examining treatment differences between anxious and nonanxious depressive patients may provide valuable information for clinicians that extend beyond our current armamentarium of psychiatric drug treatments. Truly, a dearth of literature examines other types of medication classes aside from those with monoaminergic mechanisms for the treatment of anxious depression. Investigations into experimental medications with mechanisms that manipulate cholinergic51 and/or glutamatergic52 systems may be warranted at this time.
Despite the fact that patients with anxious depression may improve with traditional antidepressants, they do not stay well for as long as their nonanxious counterparts and experience a greater burden of side effects. Specifically, future research should aim at understanding the reasons for such differences between these 2 depressed groups. Delineating clinically relevant predictors of response via diagnostic subtyping (ie, anxious depression) is crucial for improving treatment outcomes in all depressed patients. Uncovering modifiable differences between anxious and nonanxious depressive patients that clinicians can use to enhance treatment outcomes would provide a positive advancement for the field of clinical psychiatry. Ultimately, future research is critical for the successful treatment of this traditionally difficult-to-treat group of anxious depressive patients.
Drug names: aripiprazole (Abilify), bupropion (Wellbutrin, Aplenzin, and others), buspirone (BuSpar and others), citalopram (Celexa and others), clonazepam (Klonopin and others), duloxetine (Cymbalta), escitalopram (Lexapro and others), eszopiclone (Lunesta), fluoxetine (Prozac and others), imipramine (Tofranil and others), lithium (Lithobid and others), lorazepam (Ativan and others), mirtazapine (Remeron and others), nortriptyline (Pamelor, Aventyl, and others), paroxetine (Paxil, Pexeva, and others), phenelzine (Nardil), quetiapine (Seroquel), risperidone (Risperdal and others), sertraline (Zoloft and others), trazodone (Oleptro and others), venlafaxine (Effexor and others).
Disclosure of off-label usage: The authors have determined that, to the best of their knowledge, no medications are approved by the US Food and Drug Administration for the treatment of anxious depression.
Author affiliations: Experimental Therapeutics and Pathophysiology Branch, Intramural Research Program, National Institute of Mental Health, National Institutes of Health, Bethesda, Maryland.
Financial disclosure: Dr Zarate is listed as a coinventor on a patent application for the use of ketamine and its metabolites in major depression. Dr Zarate has assigned his rights in the patent to the US government but will share a percentage of any royalties that may be received by the government. Drs Ionescu, Niciu, and Richards report no conflicts of interest related to the subject of this article.
Funding/support: Funding for this work was supported by the Intramural Research Program, National Institute of Mental Health, National Institutes of Health (IRP-NIMH-NIH); by a NARSAD Independent Investigator grant to Dr Zarate; and a Brain and Behavior Mood Disorders Research Award to Dr Zarate. No other external funds were used for this study.
Role of the sponsor: The funding source did not have any role in the design or conduct of the study; collection, management, analysis, or interpretation of data; or in preparation, review, or approval of the manuscript.
Acknowledgment: Ioline Henter, MA, National Institute of Mental Health, provided invaluable editorial assistance. Ms Henter reports no conflicts of interest related to the subject of this article.
REFERENCES
1. Fava M, Rush AJ, Alpert JE, et al. Difference in treatment outcome in outpatients with anxious versus nonanxious depression: a STAR*D report. Am J Psychiatry. 2008;165(3):342-351. doi:10.1176/appi.ajp.2007.06111868 PubMed
2. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition. Arlington, VA: American Psychiatric Publishing; 2013.
3. Niciu MJ, Mathews DC, Nugent AC, et al. Developing biomarkers in mood disorders research through the use of rapid-acting antidepressants[published online ahead of print December 18, 2013]. Depress Anxiety. doi:10.1002/da.22224 PubMed
4. Fava M, Alpert JE, Carmin CN, et al. Clinical correlates and symptom patterns of anxious depression among patients with major depressive disorder in STAR*D. Psychol Med. 2004;34(7):1299-1308. doi:10.1017/S0033291704002612 PubMed
5. Domschke K, Deckert J, Arolt V, et al. Anxious versus non-anxious depression: difference in treatment outcome. J Psychopharmacol. 2010;24(4):621-622. doi:10.1177/0269881108097723 PubMed
6. Köhler S, Unger T, Hoffmann S, et al. Acute and long-term treatment outcome in depressed inpatients with versus without anxious features: results of a one-year follow-up study. J Affect Disord. 2013;150(3):1055-1061. doi:10.1016/j.jad.2013.05.043 PubMed
7. Seo HJ, Song HR, Jeong S, et al. Does comorbid subthreshold anxiety predict treatment response in depression? results from a naturalistic cohort study (the CRESCEND study). J Affect Disord. 2014;152-154:352-359. doi:10.1016/j.jad.2013.09.037 PubMed
8. Tollefson GD, Holman SL, Sayler ME, et al. Fluoxetine, placebo, and tricyclic antidepressants in major depression with and without anxious features. J Clin Psychiatry. 1994;55(2):50-59. PubMed
9. Nelson JC. Anxiety does not predict response to duloxetine in major depression: results of a pooled analysis of individual patient data from 11 placebo-controlled trials. Depress Anxiety. 2010;27(1):12-18. doi:10.1002/da.20632 PubMed
10. Altamura AC, Montresor C, Salvadori D, et al. Does comorbid subthreshold anxiety affect clinical presentation and treatment response in depression? a preliminary 12-month naturalistic study. Int J Neuropsychopharmacol. 2004;7(4):481-487. doi:10.1017/S1461145704004626 PubMed
11. Clayton PJ, Grove WM, Coryell W, et al. Follow-up and family study of anxious depression. Am J Psychiatry. 1991;148(11):1512-1517. PubMed
12. Ionescu DF, Niciu MJ, Henter ID, et al. Defining anxious depression: a review of the literature. CNS Spectr. 2013;18(5):252-260. doi:10.1017/S1092852913000114 PubMed
13. Cleary P, Guy W. Factor analysis of Hamilton Depression Scale. Drugs Exp Clin Res. 1977;1:115-120.
14. McClintock SM, Husain MM, Bernstein IH, et al. Assessing anxious features in depressed outpatients. Int J Methods Psychiatr Res. 2011;20(4):e69-e82. doi:10.1002/mpr.353 PubMed
15. Pollack MH. Comorbid anxiety and depression. J Clin Psychiatry. 2005;66(suppl 8):22-29. PubMed
16. Spalletta G, Pasini A, Caltagirone C. Fluoxetine alone in the treatment of first episode anxious-depression: an open clinical trial. J Clin Psychopharmacol. 2002;22(3):263-266. doi:10.1097/00004714-200206000-00006 PubMed
17. Fava M, Rosenbaum JF, Hoog SL, et al. Fluoxetine versus sertraline and paroxetine in major depression: tolerability and efficacy in anxious depression. J Affect Disord. 2000;59(2):119-126. doi:10.1016/S0165-0327(99)00131-7 PubMed
18. Feiger AD, Flament MF, Boyer P, et al. Sertraline versus fluoxetine in the treatment of major depression: a combined analysis of five double-blind comparator studies. Int Clin Psychopharmacol. 2003;18(4):203-210. doi:10.1097/00004850-200307000-00002 PubMed
19. Papakostas GI, Fan H, Tedeschini E. Severe and anxious depression: combining definitions of clinical subtypes to identify patients differentially responsive to selective serotonin reuptake inhibitors. Eur Neuropsychopharmacol. 2012;22(5):347-355. doi:10.1016/j.euroneuro.2011.09.009 PubMed
20. Farabaugh A, Mischoulon D, Fava M, et al. The relationship between early changes in the HAMD-17 anxiety/somatization factor items and treatment outcome among depressed outpatients. Int Clin Psychopharmacol. 2005;20(2):87-91. doi:10.1097/00004850-200503000-00004 PubMed
21. Farabaugh AH, Bitran S, Witte J, et al. Anxious depression and early changes in the HAMD-17 anxiety-somatization factor items and antidepressant treatment outcome. Int Clin Psychopharmacol. 2010;25(4):214-217. doi:10.1097/YIC.0b013e328339fbbd PubMed
22. Papakostas GI, Clain A, Ameral VE, et al. Fluoxetine-clonazepam cotherapy for anxious depression: an exploratory, post-hoc analysis of a randomized, double blind study. Int Clin Psychopharmacol. 2010;25(1):17-21. doi:10.1097/YIC.0b013e32833205a4 PubMed
23. Fava M, Schaefer K, Huang H, et al. A post hoc analysis of the effect of nightly administration of eszopiclone and a selective serotonin reuptake inhibitor in patients with insomnia and anxious depression. J Clin Psychiatry. 2011;72(4):473-479. doi:10.4088/JCP.09m05131gry PubMed
24. Nasso ED, Chiesa A, Serretti A, et al. Clinical and demographic predictors of improvement during duloxetine treatment in patients with major depression: an open-label study. Clin Drug Investig. 2011;31(6):385-405. doi:10.2165/11588800-000000000-00000 PubMed
25. Fava M, Martinez JM, Greist J, et al. The efficacy and tolerability of duloxetine in the treatment of anxious versus nonanxious depression: a post-hoc analysis of an open-label outpatient study. Ann Clin Psychiatry. 2007;19(3):187-195. doi:10.1080/10401230701465178 PubMed
26. Howland RH, Wilson MG, Kornstein SG, et al. Factors predicting reduced antidepressant response: experience with the SNRI duloxetine in patients with major depression. Ann Clin Psychiatry. 2008;20(4):209-218. doi:10.1080/10401230802437639 PubMed
27. Nelson JC. Effects of baseline depression severity on remission rates with duloxetine and placebo in anxious and nonanxious patients with major depression. J Clin Psychopharmacol. 2011;31(5):682-684. doi:10.1097/JCP.0b013e31822bee26 PubMed
28. Akkaya C, Sivrioglu EY, Akgoz S, et al. Comparison of efficacy and tolerability of reboxetine and venlafaxine XR in major depression and major depression with anxiety features: an open label study. Hum Psychopharmacol. 2006;21(5):337-345. doi:10.1002/hup.770 PubMed
29. Papakostas GI, Stahl SM, Krishen A, et al. Efficacy of bupropion and the selective serotonin reuptake inhibitors in the treatment of major depressive disorder with high levels of anxiety (anxious depression): a pooled analysis of 10 studies. J Clin Psychiatry. 2008;69(8):1287-1292. doi:10.4088/JCP.v69n0812 PubMed
30. Davidson JR, Meoni P, Haudiquet V, et al. Achieving remission with venlafaxine and fluoxetine in major depression: its relationship to anxiety symptoms. Depress Anxiety. 2002;16(1):4-13. doi:10.1002/da.10045 PubMed
31. Sir A, D’ Souza RF, Uguz S, et al. Randomized trial of sertraline versus venlafaxine XR in major depression: efficacy and discontinuation symptoms. J Clin Psychiatry. 2005;66(10):1312-1320. doi:10.4088/JCP.v66n1015 PubMed
32. Papakostas GI, Larsen K. Testing anxious depression as a predictor and moderator of symptom improvement in major depressive disorder during treatment with escitalopram. Eur Arch Psychiatry Clin Neurosci. 2011;261(3):147-156. doi:10.1007/s00406-010-0149-3 PubMed
33. Marchesi C, Ceccherininelli A, Rossi A, et al. Is anxious-agitated major depression responsive to fluoxetine? a double-blind comparison with amitriptyline. Pharmacopsychiatry. 1998;31(6):216-221. doi:10.1055/s-2007-979331 PubMed
34. Versiani M, Ontiveros A, Mazzotti G, et al. Fluoxetine versus amitriptyline in the treatment of major depression with associated anxiety (anxious depression): a double-blind comparison. Int Clin Psychopharmacol. 1999;14(6):321-327. doi:10.1097/00004850-199911000-00001 PubMed
35. Uher R, Dernovsek MZ, Mors O, et al. Melancholic, atypical and anxious depression subtypes and outcome of treatment with escitalopram and nortriptyline. J Affect Disord. 2011;132(1-2):112-120. doi:10.1016/j.jad.2011.02.014 PubMed
36. Lenze EJ, Mulsant BH, Dew MA, et al. Good treatment outcomes in late-life depression with comorbid anxiety. J Affect Disord. 2003;77(3):247-254. doi:10.1016/S0165-0327(02)00177-5 PubMed
37. Trivedi MH, Thase ME, Fava M, et al. Adjunctive aripiprazole in major depressive disorder: analysis of efficacy and safety in patients with anxious and atypical features. J Clin Psychiatry. 2008;69(12):1928-1936. doi:10.4088/JCP.v69n1211 PubMed
38. Thase ME, Demyttenaere K, Earley WR, et al. Extended release quetiapine fumarate in major depressive disorder: analysis in patients with anxious depression. Depress Anxiety. 2012;29(7):574-586. doi:10.1002/da.21970 PubMed
39. Farabaugh A, Alpert J, Wisniewski SR, et al. Cognitive therapy for anxious depression in STAR(*) D: what have we learned? J Affect Disord. 2012;142(1-3):213-218. doi:10.1016/j.jad.2012.04.029 PubMed
40. Wu Z, Chen J, Yuan C, et al. Difference in remission in a Chinese population with anxious versus nonanxious treatment-resistant depression: a report of OPERATION study. J Affect Disord. 2013;150(3):834-839. doi:10.1016/j.jad.2013.03.012 PubMed
41. Wiethoff K, Bauer M, Baghai TC, et al. Prevalence and treatment outcome in anxious versus nonanxious depression: results from the German Algorithm Project. J Clin Psychiatry. 2010;71(8):1047-1054. doi:10.4088/JCP.09m05650blu PubMed
42. Chan HN, Rush AJ, Nierenberg AA, et al. Correlates and outcomes of depressed outpatients with greater and fewer anxious symptoms: a CO-MED report. Int J Neuropsychopharmacol. 2012;15(10):1387-1399. doi:10.1017/S1461145711001660 PubMed
43. Delini-Stula A, Mikkelsen H, Angst J. Therapeutic efficacy of antidepressants in agitated anxious depression: a meta-analysis of moclobemide studies. J Affect Disord. 1995;35(1-2):21-30. doi:10.1016/0165-0327(95)00034-K PubMed
44. Flint AJ, Rifat SL. Anxious depression in elderly patients: response to antidepressant treatment. Am J Geriatr Psychiatry. 1997;5(2):107-115. PubMed
45. Flint AJ, Rifat SL. Two-year outcome of elderly patients with anxious depression. Psychiatry Res. 1997;66(1):23-31. doi:10.1016/S0165-1781(96)02964-2 PubMed
46. Baffa A, Hohoff C, Baune BT, et al. Norepinephrine and serotonin transporter genes: impact on treatment response in depression. Neuropsychobiology. 2010;62(2):121-131. doi:10.1159/000317285 PubMed
47. Domschke K, Dannlowski U, Hohoff C, et al. Neuropeptide Y (NPY) gene: impact on emotional processing and treatment response in anxious depression. Eur Neuropsychopharmacol. 2010;20(5):301-309. doi:10.1016/j.euroneuro.2009.09.006 PubMed
48. Binder EB, Owens MJ, Liu W, et al. Association of polymorphisms in genes regulating the corticotropin-releasing factor system with antidepressant treatment response. Arch Gen Psychiatry. 2010;67(4):369-379. doi:10.1001/archgenpsychiatry.2010.18 PubMed
49. Domschke K, Lawford B, Laje G, et al. Brain-derived neurotrophic factor (BDNF) gene: no major impact on antidepressant treatment response. Int J Neuropsychopharmacol. 2010;13(1):93-101. doi:10.1017/S1461145709000030 PubMed
50. Ionescu DF, Niciu MJ, Mathews DC, et al. Neurobiology of anxious depression: a review. Depress Anxiety. 2013;30(4):374-385. doi:10.1002/da.22095 PubMed
51. Drevets WC, Zarate CA Jr, Furey ML. Antidepressant effects of the muscarinic cholinergic receptor antagonist scopolamine: a review. Biol Psychiatry. 2013;73(12):1156-1163. doi:10.1016/j.biopsych.2012.09.031 PubMed
52. Aan Het Rot M, Zarate CA Jr, Charney DS, et al. Ketamine for depression: where do we go from here? Biol Psychiatry. 2012;72(7):537-547. doi:10.1016/j.biopsych.2012.05.003 PubMed




