
Manic Psychosis and Auditory Hallucinations Following Traumatic Brain Injury in a 13-Year-Old Boy
To the Editor: While traumatic brain injury (TBI) in childhood and adolescence is a major public health issue, psychosis following TBI is relatively rare and has been poorly studied. Risk factors predicting the onset of a specific psychiatric disorder after TBI in childhood include initial loss of consciousness, severe head injury, positive family psychiatric history, poor family functioning, and lower socioeconomic class.1
We present the case of a 13-year-old boy with DSM-IV mania and auditory hallucinations ordering him to stab a schoolmate with a chisel following TBI.
Case report. The patient’s personal history includes a premature birth at 32 weeks of gestational age due to uncompensated maternal diabetes; however, psychomotor development was normal and his parents described a well-socialized child with satisfactory school results despite the fact that he grew up in a conflictual family with poor income. Family history also includes an uncle suffering from psychosis.
Click figure to enlarge
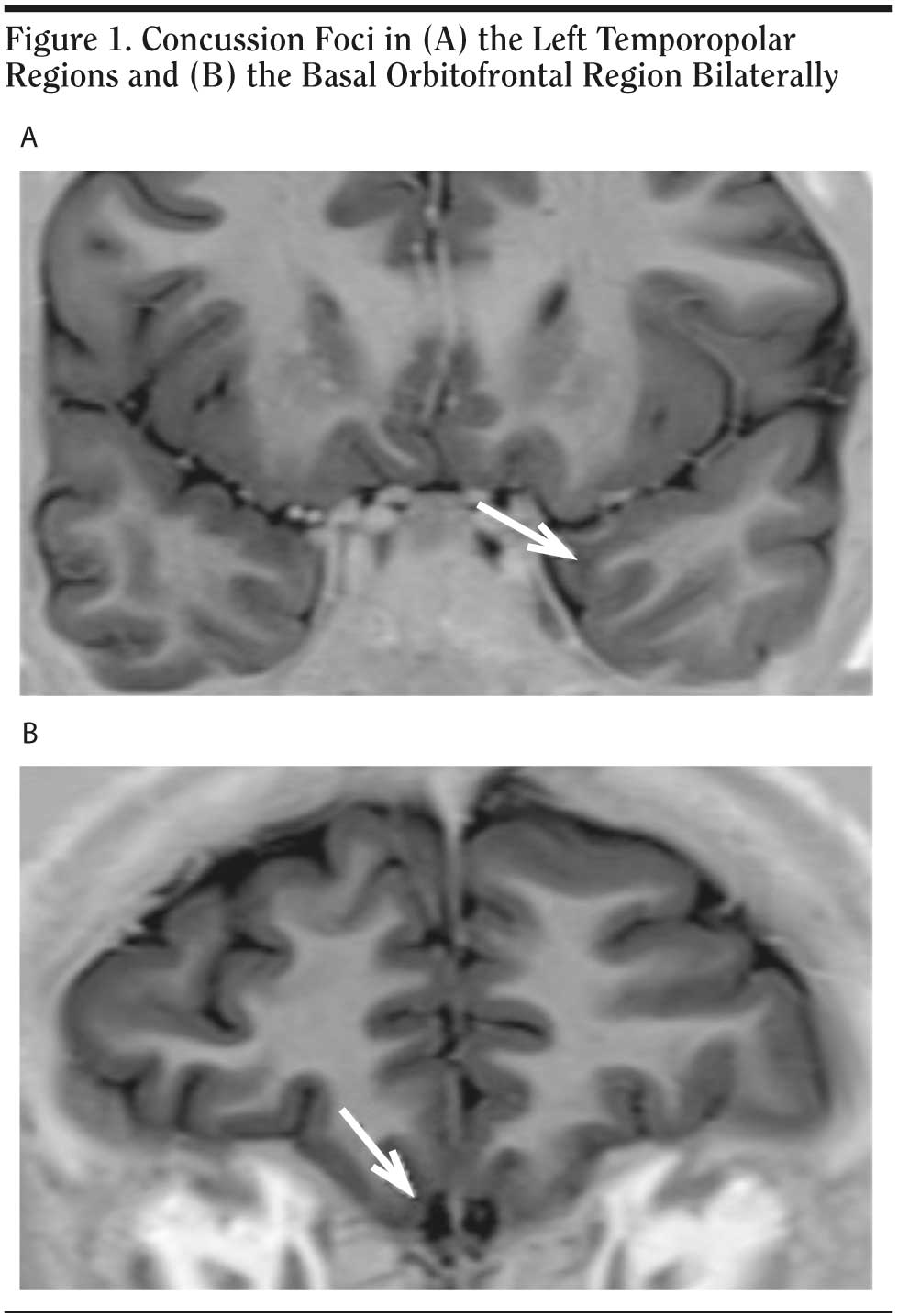
At 11 years old, the patient was the victim of head injury with a loss of consciousness of less than 30 minutes after falling from his bicycle. Approximately 7 months later, his behavior changed and his academic results decreased dramatically. Upon admission to our child and adolescent unit in 2008, 4 months after his behavior changed, he presented with euphoria, grandiosity, flight of ideas, and racing thoughts. Treatment with olanzapine was initiated (10 mg/d). Two months later, treatment with zonisamide adjunct to olanzapine was introduced after he suffered a generalized tonicoclonic seizure. Electroencephalography monitoring showed generalized spikes and waves prevailing in the frontocentral region bilaterally, compatible with partial seizures of the medial orbitofrontal cortex rather than drug-induced seizure. Brain magnetic resonance imaging (MRI) revealed concussion foci in the left temporopolar and medial orbitofrontal regions bilaterally (see Figure 1). Mean score on the Positive and Negative Syndrome Scale2 was 66 as assessed every 2 weeks during a 6-month period following olanzapine initiation. Mean score on the Young Mania Rating Scale,3 rated each week during the same period, was 26. Auditory hallucinations disappeared with antipsychotic treatment, but mania and delusions remained.
In light of the literature,4 this case report provides the first report of a clear time course between TBI and psychosis, suggesting a relationship between TBI and onset of illness; documents a biologically plausible neural correlate (with concussion foci on the MRI); and shows a possible unfavorable role of the family’s genetic background. It has been shown in adults that the presence of temporopolar lesions secondary to TBI is significantly associated with secondary mania.5 Furthermore, gray matter loss in the orbitofrontal cortex,6 which plays a role in the processing of affect and emotion, has been found in adolescents with bipolar disorder. This case report emphasizes the importance of systematically searching for a history of TBI in psychosis and further draws attention to the orbitofrontal cortex in the physiopathology of manic symptoms.
References
1. Max JE, Robin DA, Lindgren SD, et al. Traumatic brain injury in children and adolescents: psychiatric disorders at one year. J Neuropsychiatry Clin Neurosci. 1998;10(3):290-297. PubMed
2. Kay SR, Fiszbein A, Opler LA. The positive and negative syndrome scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261-276. PubMed
3. Young RC, Biggs JT, Ziegler VE, et al. A rating scale for mania: reliability, validity and sensitivity. Br J Psychiatry. 1978;133(5):429-435. doi:10.1192/bjp.133.5.429PubMed
4. Kim E, Lauterbach EC, Reeve A, et al; ANPA Committee on Research. Neuropsychiatric complications of traumatic brain injury: a critical review of the literature (a report by the ANPA Committee on Research). J Neuropsychiatry Clin Neurosci. 2007;19(2):106-127. PubMed
5. Jorge RE, Robinson RG, Starkstein SE, et al. Secondary mania following traumatic brain injury. Am J Psychiatry. 1993;150(6):916-921. PubMed
6. Wilke M, Kowatch RA, DelBello MP, et al. Voxel-based morphometry in adolescents with bipolar disorder: first results. Psychiatry Res. 2004;131(1):57-69. PubMed doi:10.1016/j.pscychresns.2004.01.004
Notice of Correction 6/16/2011: A hyphen has been added to the first author’s name, ie, Mehdi Bennouna-Greene, MD.
Author affiliations: H×´pitaux Universitaires de Strasbourg and Université de Strasbourg (all authors); and UMR-7191: LINC Laboratoire d’ Imagerie et de Neurosciences Cognitives, Université Louis Pasteur (Dr Kremer), Strasbourg, France. Author contributions: Dr Bennouna-Greene and Mr Frank contributed equally to this work. All authors have approved the manuscript. Potential conflicts of interest: The authors report no competing interests. Funding/support: None reported.
doi:10.4088/JCP.09l05685yel
© Copyright 2010 Physicians Postgraduate Press, Inc.


