Find more articles on this and other psychiatry and CNS topics:
The Journal of Clinical Psychiatry
The Primary Care Companion for CNS Disorders
CME Background
Original material is selected for credit designation based on an assessment of the educational needs of CME participants, with the purpose of providing readers with a curriculum of CME activities on a variety of topics from volume to volume.
To obtain credit, read the material and go to PrimaryCareCompanion.com to complete the Posttest and Evaluation online.
CME Objective
After studying this case, you should be able to:
- Recognize and correctly diagnose MS, especially during the early stages
- Develop an individualized, evidence-based treatment plan that includes a disease-modifying treatment and any other appropriate interventions to maintain optimal functioning and quality of life
- Educate patients about their disease and foster their involvement in the treatment process
Accreditation Statement
The University of North Texas Health Science Center at Fort Worth is accredited by the American Osteopathic Association to award continuing medical education to physicians.
This activity has been planned and implemented in accordance with the Essential Areas and Policies of the Accreditation Council for Continuing Medical Education through the joint sponsorship of The University of North Texas Health Science Center and the CME Institute of Physicians Postgraduate Press, Inc. The University of North Texas Health Science Center is accredited by the ACCME to provide continuing medical education for physicians.
Credit Designation
The University of North Texas Health Science Center has requested that the AOA Council on Continuing Medical Education approve this program for 1.0 hour of AOA Category 2B CME credits. Approval is currently pending.
The University of North Texas Health Science Center designates this enduring material for a maximum of 1.0 AMA PRA Category 1 Creditâ„¢. Physicians should claim only the credit commensurate with the extent of their participation in the activity.
Date of Original Release/Review
This educational activity is eligible for AMA PRA Category 1 Creditâ„¢ through October 31, 2013. The latest review of this material was September 2012.
Financial Disclosure
The faculty for this CME activity, the CME Institute staff, and the University of North Texas Health Science Center staff were asked to complete a statement regarding all relevant personal and financial relationships between themselves or their spouse/partner and any commercial interest. The CME Institute and the University of North Texas Health Science Center have resolved any conflicts of interest that were identified. No member of the CME Institute staff or the University of North Texas Health Science Center staff reported any relevant personal financial relationships. Faculty financial disclosure appears with the article.
Many clinicians are not confident in their ability to diagnose multiple sclerosis (MS), and patients often receive an incorrect diagnosis due to having diverse and vague symptoms and an unpredictable disease course. Timely recognition is critical because the progression of MS can be delayed, and clinically definite MS can possibly be prevented if treatment with a disease-modifying drug is initiated early. Despite the benefits of these agents and guidelines recommending them for MS, only some patients with the most common form of MS receive a disease-modifying therapy. Also, most patients with MS prefer an active role in their treatment and need to be informed about their illness and available treatments. Unfortunately, cognitive deficits common in MS may make informed decision-making difficult. Emmanuelle Waubant, MD, PhD, who is from the Department of Neurology at the University of California San Francisco Multiple Sclerosis Center, presented information for primary care physicians on the importance of recognizing MS in its early stages, making an accurate and timely diagnosis, educating patients about MS and its treatments, implementing disease-modifying therapy, and developing a treatment plan to help patients maintain functioning and experience optimal quality of life.
![]()
This Commentary is derived from the planning teleconference “Improving Outcomes in Multiple Sclerosis Through Early Diagnosis and Effective Management,” which was held on March 19, 2012, and was independently developed by the University of North Texas Health Science Center and the CME Institute of Physicians Postgraduate Press, Inc., also an accredited provider, pursuant to an educational grant from Pfizer.
Financial disclosure: Dr Waubant is a consultant for Actelion and Chugai; has received grant/research support from Sanofi Aventis, Roche, Teva, and Biogen Idec; and has provided 3 educational talks for Teva and Biogen Idec in the past year.
The opinions expressed herein are those of the faculty and do not necessarily reflect the opinions of the CME provider, publisher, or the commercial supporter.
Prim Care Companion CNS Disord 2012;14(5):doi:10.4088/PCC.11016co2cc
© Copyright 2012 Physicians Postgraduate Press, Inc.
Published online: October 25, 2012.
Multiple sclerosis (MS) is one of the most prevalent diseases of the nervous system, affecting about 400,000 people in the United States.1 MS appears more frequently in women, in people aged 20 to 50 years, and in people living farther from the equator. As a chronic autoimmune disorder, MS results in demyelination and neurodegeneration. Although the cause is unknown, white blood cells (or T cells) are activated, leave the bloodstream, and infiltrate the blood-brain barrier. In the central nervous system (CNS), the T cells release proinflammatory cytokines, which attract other cells to attack and damage myelin sheaths that protect neuronal fibers, leading to scarring and axonal injury. This damage can affect patients’ mobility, vision, and/or cognitive functioning, especially if left untreated, which underscores the importance of the early recognition of MS.
The overall etiology of MS is unclear, but researchers have studied several genes and environmental factors that may increase the risk of this condition. Although MS is not directly hereditary, having a family member with MS does appear to increase the risk.1 Environmental factors may include low exposure to sunlight and vitamin D deficiency, which could explain why areas farther from the equator have more cases of MS. Exposure to certain viruses, such as measles or Epstein-Barr, may also predispose people to developing MS.
By following guidelines and completing diagnostic tests to accurately recognize the disorder as early as possible and by initiating appropriate treatments or referring to a specialist, clinicians can greatly reduce the damaging and irreversible course of MS.
Accurate Diagnosis
The signs and symptoms of MS vary among patients and can even fluctuate in the same person. Therefore, making an accurate diagnosis is challenging, and misdiagnosis is common.2,3 To ensure an accurate diagnosis, primary care clinicians can be alert to recognize the symptoms of MS, understand the clinical subtypes of MS and their course of illness, use diagnostic criteria, and conduct diagnostic tests and a differential diagnosis to rule out other medical conditions.
Recognize Symptoms
MS symptoms are typically caused by lesions in the CNS. The first symptom episode is usually called a clinically isolated syndrome (CIS). Symptoms most often seen in a CIS are those related to lesions or inflammation in the optic nerve, the brainstem, or the spinal cord. Less typical are CIS presentations affecting the cerebral hemispheres (Table 1).4-6
Embarrassed Employee
Mr A, a 55-year-old male, limps into your office with a noticeable foot drag. When questioned, he cannot remember when his limp began. He also admits to loss of bladder control, which has occurred twice in the past week and has caused him embarrassment.
Which area of the CNS is most likely affected?
Optic nerve symptoms. A CIS that is often seen in patients with MS is optic neuritis, or inflammation of the optic nerve of one eye.4 Symptoms include pain upon moving the eye, blurred vision, or reduced or lost vision. These symptoms are usually temporary (ie, last a few days or weeks).
Brainstem/cerebellum symptoms. Nerve damage in the brainstem or cerebellum can cause patients to experience symptoms such as imbalance, tremor, incoordination, vertigo, and ataxia, a swaying type of gait. Imbalance and incoordination can lead to increased falls, injury, and reduced activity. Although ataxia is associated with damage in the cerebellum, one study7 suggested that balance deficits in people with MS are actually caused by slowed spinal somatosensory conduction rather than by cerebellar involvement. Other difficulties walking may be the result of muscle weakness, due to cord injury but also to reduced activity, which can lead to deconditioning.5
Click figure to enlarge
Other symptoms resulting from lesions in the brainstem and cerebellum include spasms and impaired swallowing or speech,6 such as dysarthria, a speech disorder caused by damage to facial muscle control.
Spinal cord symptoms. Patients with myelopathy can experience a motor deficit of 1 or more limbs or sensory deficits, which may be accompanied by a tingling or burning sensation in various parts of the body.5
Other symptoms include bladder, bowel, or sexual dysfunctions. Because MS lesions disrupt the transmission of nerve signals that control the bladder and urinary sphincter, at least 80% of patients with MS suffer from bladder dysfunction.5 Symptoms include urination frequency, urgency, or hesitancy, as well as incontinence and nocturia.5
Like bladder dysfunction, bowel dysfunction can cause patients embarrassment and exacerbate other symptoms. Bowel dysfunction includes constipation, diarrhea, or loss of bowel control. For severe symptoms, consider referring patients to a gastroenterologist.
Sexual dysfunction is often ignored by patients and clinicians but should be discussed. Patients may report problems such as reduced or heightened sensation, difficulty achieving orgasm or erection, or loss of libido. Clinicians should be aware that these problems are common in the general public and are not necessarily indicative of MS.

- Patients with MS may present clinically with eye problems, mobility issues, bowel and bladder problems, cognitive deficits, muscle weakness, and fatigue.
- The revised diagnostic criteria for MS require the presence of more than 2 silent lesions with dissemination in space and time.
- In addition to using diagnostic criteria, clinicians must take a thorough patient history and complete a differential diagnosis.
- A referral to a neurologist is necessary if the patient presents with new neurologic symptoms.
- Medications are available to manage the symptoms of MS and to slow the disability and prevent exacerbations associated with the disease progression, but at this time there is no cure for MS.
Cerebral hemisphere symptoms. Patients with MS may experience a hemispheric onset of symptoms, although this occurrence is not common. Hemispheric symptoms include executive function deficits, depression, visual field defects, and hemiparesis (weakness on 1 side of the body), and, rarely, difficulty speaking.4,6
Nonspecific symptoms. Two common symptoms that are not associated with a specific CNS area but may accompany MS onset and subsequent flare-ups are fatigue and cognitive changes. Over 50% of patients with MS experience fatigue and/or cognitive dysfunction.5 These 2 symptoms contribute substantially to patients’ declined functioning and inability to work, making them key treatment targets.
Fatigue can be caused by conditions such as depression or interrupted sleep, but it can also be a symptom unique to MS. Researchers are characterizing distinguishing features of MS fatigue, or lassitude, which tends to occur on a daily basis, may have a sudden onset, and generally worsens throughout the day.5 MS fatigue can be aggravated by heat and is likely to interfere with daily responsibilities.
Cognitive problems that are most often associated with MS include storing and recalling new information, concentrating, processing sensory information, planning and prioritizing, and word-finding. Visuospatial function, such as depth perception, may also be affected; however, general intellect, long-term memory, conversational skills, and reading comprehension may remain unaffected. Although cognitive changes may be present at the onset of MS, patients usually experience dysfunction later in the disease course.5
Embarrassed Employee Diagnosis
Mr A demonstrates symptoms consistent with spinal cord damage, which include motor deficits and bladder dysfunction. When he is assessed for MS, he will likely have a negative cerebrospinal fluid result, unless tested for oligoclonal bands and IgG index, but will show characteristic findings of lesions on MRI.
Managing MS symptoms. Although no treatments currently exist for some symptoms like cognitive problems, clinicians can provide treatment to alleviate other MS symptoms (Table 2).8
Click figure to enlarge
Understand Clinical Subtypes
Four subtypes of MS have been identified and are defined by the clinical course at onset and over time. Clinicians should be aware that, regardless of the subtype of MS the patient has, the course of MS is unpredictable. The frequency, number, and severity of exacerbations are different for each patient, and clinicians must understand the fear and anxiety this uncertainty causes patients.
Relapsing-remitting MS. Relapsing-remitting MS is the most common form of MS at onset, with about 85% of patients presenting with this type.1 Patients with relapsing-remitting MS typically experience a rapid onset of symptoms over a matter of hours or days followed by a period of improvement over a few days or weeks. After a period of remission of months or years, new symptoms return (known as an exacerbation, relapse, or attack).
Primary progressive MS. Primary progressive MS is characterized by a steady and gradual worsening in function with no periods of distinct exacerbations or improvement. About 10% of patients are diagnosed with this subtype of MS.9
Secondary progressive MS. Secondary progressive MS begins as relapsing-remitting MS but transitions into a course of illness with worse and more frequent exacerbations followed by little or no improvement. About 50% of patients who have relapsing-remitting MS and do not receive treatment will transition to secondary progressive MS after about 10 years.9
Progressive relapsing MS. The rarest course of MS is progressive relapsing MS, which affects about 5% of patients.9 Progressive relapsing MS has the initial insidious onset of primary progressive MS with a steady onset but is also characterized by an additional small number of acute exacerbations with or without improvement. The progressive course of the disease is without remissions.
Once clinicians understand the different presentations and courses of MS, diagnostic criteria can provide a practical tool to help establish a firm and accurate diagnosis of MS.
Use Diagnostic Criteria
The McDonald Criteria integrate imaging assessments with clinical methods to simplify and expedite making an accurate diagnosis.10 The criteria are centered around collectively assessing and evaluating clinical evidence, establishing the presence of demyelinating lesions on the brain or spinal cord using magnetic resonance imaging (MRI) scans, conducting other diagnostic tests as needed, and excluding alternative diagnoses.11
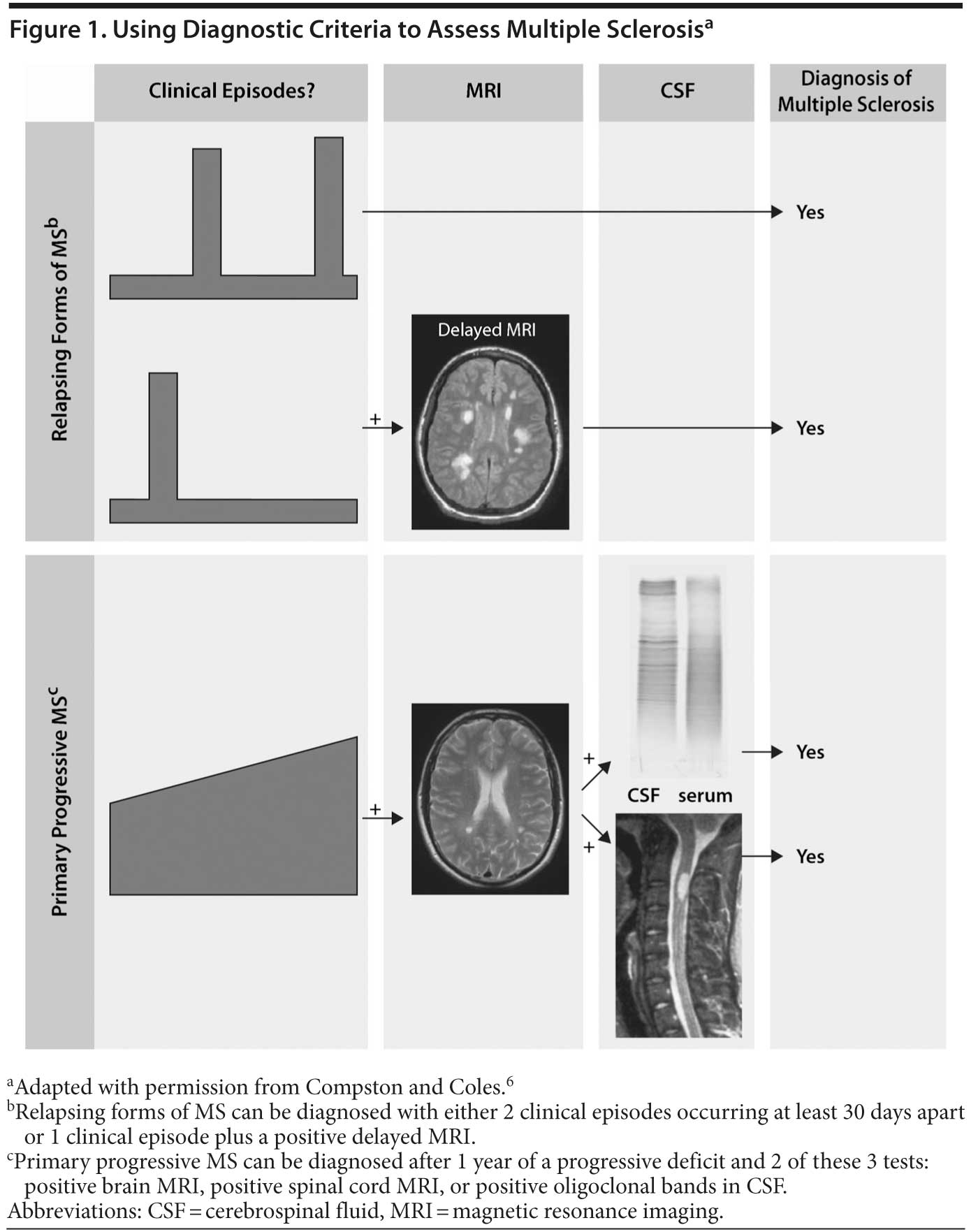
To meet the diagnostic criteria for MS, dissemination of lesions in space and in time must be shown. This means that the patient must have evidence of lesions in more than 1 area of the CNS on more than 1 occasion (Figure 1).6 Lesions are confirmed through MRI testing, but imaging is not required for a diagnosis if the patient has already had 2 or more attacks.
Click figure to enlarge
Conduct Evaluation and Tests
Fatigued Female
Mrs B, a 29-year-old female patient, is newly married and wants to get pregnant. Her past medical history includes a brief episode of double vision 2 years ago when she was completing her graduate studies. She is now experiencing pain with movement in her left eye. She is concerned about her vision and reports tiredness throughout the day, which worsens when she is hot. She worries that she does not have the energy for pregnancy and child rearing.
What assessment tools would best confirm or rule out an MS diagnosis?
Risk factors. Many risk factors are possible contributors to MS. Some already mentioned include vitamin D deficiency and decreased sunlight exposure, as well as certain viruses, but no definitive proof currently exists to determine if viruses such as measles, herpes, and Epstein-Barr are a direct or indirect contributing factor.5
Evidence suggests that MS susceptibility pertains to multifaceted and currently undefined interactions between genes and environmental factors. Heritability plays a small factor, and several genes have been found to be implicated in the risk of MS. The human leukocyte antigen (HLA) gene region is estimated to account for much of the genetic susceptibility in MS.12 Most of the genetic risk factors identified with MS are on the immune response pathway. Until genetic testing for MS is well defined and available, clinicians must rely on recognizing symptoms of MS and using them to guide decisions for testing or referral.
Referral. Referral to a neurologist is recommended if patients present with new neurologic symptoms. Patients need referral if they report difficulty with balance or gait, focal numbness or weakness, or unilateral visual blurring and retro-orbital pain. Symptoms of fatigue, cognitive changes, depression, and sexual or bladder dysfunction should raise suspicion of MS, but, if they occur in isolation, the patient may not need referral unless MRI results indicate brain, optic nerve, or spinal cord lesion involvement.
Patient history. The clinical evaluation should start with a thorough patient history. Information about the presenting neurologic symptom should include the mode of onset, duration, precipitating factors, and accompanying features. Neurologic symptoms that developed over hours or days should be suspect. Querying patients for previous symptoms is critical because they may have dismissed transient problems or pain or they may already have had a CIS without realizing it, meaning that the current symptom is actually a second attack.
Physical examination. In addition to taking the patient’s history, clinicians should perform a physical examination and look for red flags associated with CNS problems, such as motor deficits, increased reflexes, or sensory symptoms. Compromised vision or eye pain should raise suspicion for optic neuritis.
MRI. Obtaining a brain or spinal cord MRI is one of the most important early steps for clinicians to establish a diagnosis of MS.11 MRI reveals focal or confluent abnormalities in white matter in more than 95% of patients with MS (although nonspecific T2-bright lesions may also be present in people without MS, especially after age 50 years).6 MS lesions are usually larger than 3 mm, ovoid, often perpendicular to the lateral ventricle, and focused in the corpus callosum, brainstem, cerebellum, and posterior cervical spinal cord. Newer lesions will enhance with gadolinium, an agent used for image contrast, which may help distinguish MS lesions from lesions caused by other conditions. Due to the disruption of the blood-brain barrier that occurs in patients with MS, lesions can be enhanced for 1 to 4 weeks before enhancement disappears, but T2-bright footprints are left on the MRI, distinguishing the presence of abnormalities after the lesions have healed.
Spinal tap. A lumbar puncture, or spinal tap, can show an abnormal autoimmune response via an excess of white blood cells or antibodies in the cerebrospinal fluid (CSF). If MS is suspected, analyzing CSF can establish the presence of oligoclonal bands or increased immunoglobulin G (IgG) index.11 Although most people with MS have oligoclonal bands in the CSF, this measurement can also be indicative of other autoimmune disorders; therefore, the spinal tap alone cannot confirm or rule out an MS diagnosis.13
Evoked potential test. Evoked potential tests record the nerves’ response to electric stimulation. Although evoked potential tests can be used to test hearing, vision, and other sensory functioning, the most common evoked potential test for MS is the visual evoked response, which can reveal optic nerve demyelination that may not appear on the MRI scan. When necessary, this test may identify a second demyelinating event, which sometimes has been “silent,” needed to confirm an MS diagnosis.
Fatigued Female Diagnosis
To confirm or rule out a diagnosis of MS, clinicians should use a neurologic exam to evaluate Mrs B’s vision, mobility, and reflexes. Then, conduct a brain MRI to assess lesion activity and size.
The results reveal that her double vision 2 years ago was likely her first MS flare. The MRI scan shows 2 ovoid T2 lesions in the deep white matter and, coupled with her current symptoms of eye pain and fatigue, as well as her history, meets the diagnostic criteria of dissemination in time and space.
Conduct Differential Diagnosis
When completing a differential diagnosis for MS, clinicians should be aware that many illnesses can mimic symptoms of MS and should be ruled out to ensure an accurate diagnosis.14 Infectious diseases to exclude are Lyme disease, syphilis, human immunodeficiency virus, and, depending on the patient’s risk factors, progressive multifocal leukoencephalopathy. Other mimicking conditions include rheumatologic or inflammatory illnesses such as lupus erythematosus, rheumatoid arthritis, Sjögren’s syndrome, neurosarcoidosis, Behçet’s disease, and Wegener’s syndrome. Metabolic, neoplastic, and genetic disorders such as vitamin B12 deficiency, lymphoma, and adrenoleukodystrophy must also be ruled out, especially in patients with progressive onset. Other demyelinating pathologies that present similarly to MS are neuromyelitis optica and acute disseminated encephalomyelitis.
In addition to conditions that can mimic symptoms of relapsing-remitting MS, clinicians must know the more degenerative illnesses that can mimic progressive forms of MS, such as neoplasm, tuberculosis, and neurosyphilis, as well as spinal cord syndromes including human T-cell lymphotropic virus 1 and 2 and hereditary spastic paraparesis.
Clinicians should always tailor the differential diagnosis to each individual patient. Most of the conditions similar to MS can be diagnosed with appropriate tests, such as blood tests, spinal taps, or biopsies.
Importance of Early Recognition and Treatment
Because disability accumulates over time, the diagnosis of MS needs to be accurate and occur as early as possible. Patients can accumulate disability in 2 ways: 1 way is related to attacks and the other way is independent of relapses. After an exacerbation of new MS symptoms, patients develop irreversible CNS deficits. Even at the CIS stage, patients already show attack-related and unrelated CNS damage (from MRI scans and sometimes clinically); however, a certain amount of tissue injury/loss must occur in a clinically relevant area before an attack is detected clinically. If patients in the early stages of MS are imaged regularly, clinicians can document brain atrophy independent of new lesions developing and new lesions developing faster than relapses occur. Early detection enables clinicians to initiate early therapy, which has been to shown to delay the onset of disability,15 and can possibly slow the accumulation of disability and prevent or delay exacerbations.
Early recognition can also help to alleviate some patient anxiety. Many symptoms of MS are painful, debilitating, or embarrassing. Reaching a diagnosis can take away the patient’s anxiety about the unknown cause of symptoms. Clinicians should establish a dialogue with patients to prepare them for additional diagnostics or a referral, to address symptom management, and to involve them in treatment decisions. Clinicians should also encourage lifestyle changes, such as exercising, eating a healthy diet, and stopping smoking. Physicians may want to suggest individual or family counseling to address coping with a new diagnosis or—because MS can be unpredictable—adjusting to changes in symptoms.
Early Treatment Overview
Although current treatments are available for the relapsing forms of MS and specific symptoms, no treatment has been shown to improve the primary progressive form of MS. Additionally, no treatment will reverse the extent of neurologic damage caused by the disease, especially when the disability has been present for over 12 months. To determine the extent of disability the patient has experienced, clinicians can use the Expanded Disability Status Scale.
This overview of treatment options provides a working knowledge for primary care physicians. Because no cure for MS exists, available treatments are known as disease-modifying therapy. Treatment should be customized for the patient to optimize adherence and tolerability.
Relapse Prevention Treatment
Interferon β-1a (IFNβ-1a), interferon β-1b (IFNβ-1b), glatiramer acetate, and fingolimod are approved by the US Food and Drug Administration (FDA) to slow the accumulation of physical disability and to decrease the frequency of MS exacerbations and may be considered first-line treatments for patients with relapsing forms of MS. Interferons and glatiramer acetate have been on the market for more than 15 years, while fingolimod was approved in 2010.
Interferon β. Interferons, which are administered by either an intramuscular or subcutaneous injection, work by increasing anti-inflammatory cytokines, interfering with T cells crossing the blood-brain barrier, and decreasing T-cell activation. With subcutaneous IFNβ-1a, some data16 suggest that high-dose IFNβ has greater efficacy than low-dose; however, 1 study17 did not demonstrate a statistically significant difference in efficacy between the 2 doses.
The most common side effects with interferons are flu-like symptoms ranging from a mild headache and tiredness to enervation and fever. Injection site reactions can be pre-treated with a nonsteroidal anti-inflammatory drug or acetaminophen. Other possible side effects include depression, transaminitis, and decreased white blood cell count, which is why clinicians should monitor white blood cell count and liver function in patients receiving interferon therapy.
Glatiramer acetate. Glatiramer acetate is a subcutaneous injection that induces antigen-specific suppressor T cells, inhibits antigen presentation, and causes an immune deviation in T cells from a Th1 to a Th2 phenotype. It does not produce flu-like symptoms or require laboratory monitoring, like with the interferons, but glatiramer acetate can cause reactions at the injection site or, much less frequently, very transient chest tightness or discomfort.
One study18 found similar efficacy and tolerability among 2 different doses of subcutaneous IFNβ-1b and glatiramer acetate, with both agents limiting relapse risk in patients with relapsing-remitting MS.
Fingolimod. Fingolimod, an oral medication, reduces pathogenic lymphocytes. Recent studies19,20 have demonstrated that fingolimod improved relapse rate and MRI outcomes compared with interferons and placebo, but safety concerns remain to be resolved and possible long-term risks are yet to be determined. Bradycardia and atrioventricular conduction block may occur at treatment initiation, while a few cases of systemic viral infections (possibly fatal) have occurred. Due to potential liver toxicity, this treatment also necessitates liver enzyme monitoring.
For patients who experience frequent relapse, disability progression, or changes on MRIs, switching between first-line medications or even considering a second-line therapy are options. For example, one study21 found that relapse rates improved in patients failing initial therapy who switched to another first-line treatment.
Second-Line Relapse Prevention Treatments
For patients with worsening MS, clinicians may decide to proceed with treatment using a second-line agent for breakthrough disease. Two FDA-approved second-line treatments for this patient population are the intravenous agents natalizumab and mitoxantrone.
Natalizumab. Natalizumab, a monoclonal antibody, is used for breakthrough relapsing-remitting MS. One study22 found that natalizumab decreased clinical relapse at 1 year by 68% and reduced MRI activity over 2 years by 83%. Although effective and well-tolerated, natalizumab carries the risk for allergic reaction (less than 5%) and, more rarely, progressive multifocal leukoencephalopathy (PML), a brain infection with no available treatment. A new blood test for JC virus antibodies helps to identify patients at risk of PML.
Mitoxantrone. Mitoxantrone is an immunosuppressant used for worsening MS but is not indicated for use in primary progressive MS. Because mitoxantrone carries risks for bone marrow suppression and cardiotoxicity, patients taking this agent should have cardiac, liver, and white blood cell count monitoring. Treatment is limited over a 2-year period.
Progressive MS Treatment
While no drugs are approved for progressive MS, specialists may consider trying off-label drugs including pulse steroids, such as cyclophosphamide, and rituximab.23 Exercise is often not emphasized enough, but it may help patients to strengthen muscle power and improve mobility as well as mood.24 Exercise may also help prevent osteoporosis, for which patients with MS should be screened.25
Exacerbation Treatment
Mild MS exacerbations are usually not treated with drugs. If a patient presents with an acute relapse with escalating or significant symptoms that are affecting daily function, treatment options are available. For patients currently taking medication to manage MS, short-term high-dose intravenous corticosteroids such as methylprednisolone26 or oral dexamethasone can reduce inflammation as well as shorten the duration of the attack.27 If pulse steroids are not effective and the exacerbation is severe, specialists may try plasmapheresis, or plasma exchange, to decrease residual MS symptoms.28,29
Additional and Future Treatments
More treatments for MS are being tested, and some look promising. Vitamin D3 supplementation is tested for decreasing subsequent relapses in patients with CIS or MS,30 and a placebo-controlled study31 found a reduction in T1-enhancing lesions over 1 year in those receiving vitamin D3 supplementation. Other off-label options may include mycophenolate mofetil,32 daclizumab,33 and alemtuzumab.33 Drugs that may become available in the future are fumaric acid, laquinimod, teriflunomide, and ocrelizumab.33
Patients’ Role in Treatment
For all MS treatment plans, patient involvement is critical because patients need to understand the benefits, risks, side effects, and probable outcomes associated with various therapies, especially those requiring injection training or regular monitoring. Empathy toward patients’ fears and preferences and customization of treatment will help to optimize patients’ outcomes.
Conclusion
Early recognition and accurate diagnosis of MS are crucial to delay disease progression as much as possible and improve patients’ outcomes. If treatment is not initiated within an early window, disability can accumulate and patients can experience irreversible neurologic damage. By taking a thorough patient history, using diagnostic criteria, conducting imaging and other diagnostic tests, and completing a differential diagnosis, clinicians can make an accurate diagnosis of MS. Patients with suspected MS that cannot be confirmed by evaluation and testing should be referred to a neurologist.
Using first- and second-line treatments, clinicians can help patients with MS prevent exacerbations and slow disease progression. Exercise and patient involvement are also important factors in MS treatment. Establishing open communication and a strong therapeutic alliance allows clinicians to help alleviate patients’ fears and incorporate their preferences into the comprehensive treatment plan.
Disclosure of off-label usage: Dr Waubant has determined that, to the best of her knowledge, alemtuzumab, cyclophosphamide, daclizumab, dexamethasone, mycophenolate mofetil, rituzimab, laquinomod, ocrelizumab, and teriflunomide are not approved by the US Food and Drug Administration for the treatment of multiple sclerosis; bupropion, amantadine, and pemoline are not approved for the treatment of fatigue; gabapentin is not approved for the treatment of spasticity; and papaverine is not approved for the treatment of sexual dysfunction.
Drug names: alemtuzumab (Campath), alprostadil (Caverject, Edex, and others), baclofen (Gablofen, Lioresal, and others), bupropion (Wellbutrin, Aplenzin, and others), clonazepam (Klonopin and others), cyclophosphamide (Cytoxan and others), daclizumab (Zenapax), dantrolene (Dantrium and others), dexamethasone (Maxidex, Ozurdex, and others), diazepam (Valium, Diastat, and others), fingolimod (Gilenya), gabapentin (Gralise, Neurontin, and others), glatiramer acetate (Copaxone), interferon β-1a (Avonex, Rebif), interferon β-1b (Betaseron, Extavia), methylprednisolone (Medrol, DepoMedrol, and others), modafinil (Provigil and others), mycophenolate mofetil (Cellcept and others), natalizumab (Tysabri), oxybutynin (Anturol, Ditropan, and others), rituximab (Rituxan), sildenafil (Revatio, Viagra), tizanidine (Zanaflex and others), tolterodine (Detrol), trospium (Sanctura and others), vardenafil (Levitra, Staxyn, and others).
References
1. National Multiple Sclerosis Society. Who gets Multiple Sclerosis? http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-about-ms/who-gets-ms/index.aspx. Accessed June 18, 2012.
2. Trojano M, Paolicelli D. The differential diagnosis of multiple sclerosis: classification and clinical features of relapsing and progressive neurological syndromes. Neurol Sci. 2001;22(suppl 2):S98-S102. PubMed doi:10.1007/s100720100044
3. Solomon AJ, Klein EP, Bourdette D. “Undiagnosing” multiple sclerosis: the challenge of misdiagnosis in MS. Neurology. 2012;78(24):1986-1991. PubMed doi:10.1212/WNL.0b013e318259e1b2
4. Miller DH, Weinshenker BG, Filippi M, et al. Differential diagnosis of suspected multiple sclerosis: a consensus approach. Mult Scler. 2008;14(9):1157-1174. PubMed doi:10.1177/1352458508096878
5. National Multiple Sclerosis Society. Symptoms. http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-about-ms/symptoms/index.aspx. Accessed May 29, 2012.
6. Compston A, Coles A. Multiple sclerosis. Lancet. 2008;372(9648):1502-1517. PubMed doi:10.1016/S0140-6736(08)61620-7
7 Cameron MH, Horak FB, Herndon RR, et al. Imbalance in multiple sclerosis: a result of slowed spinal somatosensory conduction. Somatosens Mot Res. 2008;25(2):113-122. PubMed doi:10.1080/08990220802131127
8. Crayton HJ, Rossman HS. Managing the symptoms of multiple sclerosis: a multimodal approach. Clin Ther. 2006;28(4):445-460. PubMed doi:10.1016/j.clinthera.2006.04.005
9. National Multiple Sclerosis Society. What is Multiple Sclerosis? http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-about-ms/what-is-ms/index.aspx. Accessed May 25, 2012.
10. Polman CH, Reingold SC, Edan G, et al. Diagnostic criteria for multiple sclerosis: 2005 revisions to the “McDonald Criteria.” Ann Neurol. 2005;58(6):840-846. PubMed doi:10.1002/ana.20703
11. Polman CH, Reingold SC, Banwell B, et al. Diagnostic criteria for multiple sclerosis: 2010 revisions to the McDonald criteria. Ann Neurol. 2011;69(2):292-302. PubMed doi:10.1002/ana.22366
12. Link J, Kockum I, Lorentzen AR, et al. Importance of human leukocyte antigen (HLA) class I and II alleles on the risk of multiple sclerosis. PLoS ONE. 2012;7(5):e36779. PubMed doi:10.1371/journal.pone.0036779
13. National Multiple Sclerosis Society. Diagnosing Multiple Sclerosis. http://www.nationalmssociety.org/about-multiple-sclerosis/what-we-know-about-ms/diagnosing-ms/index.aspx. Accessed June 14, 2012.
14. Rolak LA, Fleming JO. The differential diagnosis of multiple sclerosis. Neurologist. 2007;13(2):57-72. PubMed doi:10.1097/01.nrl.0000254705.39956.34
15. Kappos L, Freedman MS, Polman CH, et al, for the BENEFIT Study Group. Effect of early versus delayed interferon beta-1b treatment on disability after a first clinical event suggestive of multiple sclerosis: a 3-year follow-up analysis of the BENEFIT study. Lancet. 2007;370(9585):389-397. PubMed doi:10.1016/S0140-6736(07)61194-5
16. Schwid SR, Panitch HS. Full results of the Evidence of Interferon Dose-Response-European North American Comparative Efficacy (EVIDENCE) study: a multicenter, randomized, assessor-blinded comparison of low-dose weekly versus high-dose, high-frequency interferon beta-1a for relapsing multiple sclerosis. Clin Ther. 2007;29(9):2031-2048. PubMed doi:10.1016/j.clinthera.2007.09.025
17. Minagar A, Murray TJ; PROOF Study Investigators. Efficacy and tolerability of intramuscular interferon beta-1a compared with subcutaneous interferon beta-1a in relapsing MS: results from PROOF. Curr Med Res Opin. 2008;24(4):1049-1055. PubMed doi:10.1185/030079908X280545
18. O’ Connor P, Filippi M, Arnason B, et al, for the BEYOND Study Group. 250 microg or 500 microg interferon beta-1b versus 20 mg glatiramer acetate in relapsing-remitting multiple sclerosis: a prospective, randomised, multicentre study. Lancet Neurol. 2009;8(10):889-897. PubMed doi:10.1016/S1474-4422(09)70226-1
19. Kappos L, Radue EW, O’ Connor P, et al, for the FREEDOMS Study Group. A placebo-controlled trial of oral fingolimod in relapsing multiple sclerosis. N Engl J Med. 2010;362(5):387-401. PubMed doi:10.1056/NEJMoa0909494
20. Cohen JA, Barkhof F, Comi G, et al, for the TRANSFORMS Study Group. Oral fingolimod or intramuscular interferon for relapsing multiple sclerosis. N Engl J Med. 2010;362(5):402-415. PubMed doi:10.1056/NEJMoa0907839
21. Gajofatto A, Bacchetti P, Grimes B, et al. Switching first-line disease-modifying therapy after failure: impact on the course of relapsing-remitting multiple sclerosis. Mult Scler. 2009;15(1):50-58. PubMed doi:10.1177/1352458508096687
22. Polman CH, O’ Connor PW, Havrdova E, et al, for the AFFIRM Investigators. A randomized, placebo-controlled trial of natalizumab for relapsing multiple sclerosis. N Engl J Med. 2006;354(9):899-910. PubMed doi:10.1056/NEJMoa044397
23. Olek MJ. Treatment of progressive multiple sclerosis in adults. Published 2012. http://www.uptodate.com/contents/treatment-of-progressive-multiple-sclerosis-in-adults?view=print. Accessed September 19, 2012.
24. Rietberg MB, Brooks D, Uitdehaag BM, et al. Exercise therapy for multiple sclerosis. Cochrane Database Syst Rev. 2005;25(1):CD003980. PubMed
25. Kampman MT, Eriksen EF, Holm׸y T. Multiple sclerosis, a cause of secondary osteoporosis? what is the evidence and what are the clinical implications? Acta Neurol Scand Suppl. 2011;124(s191):44-49. PubMed doi:10.1111/j.1600-0404.2011.01543.x
26. La Mantia L, Eoli M, Milanese C, et al. Double-blind trial of dexamethasone versus methylprednisolone in multiple sclerosis acute relapses. Eur Neurol. 1994;34(4):199-203. PubMed doi:10.1159/000117038
27. Repovic P, Lublin FD. Treatment of multiple sclerosis exacerbations. Neurol Clin. 2011;29(2):389-400. PubMed doi:10.1016/j.ncl.2010.12.012
28. Weinshenker BG, O’ Brien PC, Petterson TM, et al. A randomized trial of plasma exchange in acute central nervous system inflammatory demyelinating disease. Ann Neurol. 1999;46(6):878-886. PubMed doi:10.1002/1531-8249(199912)46:6<878::AID-ANA10>3.0.CO;2-Q
29. Keegan M, Pineda AA, McClelland RL, et al. Plasma exchange for severe attacks of CNS demyelination: predictors of response. Neurology. 2002;58(1):143-146. PubMed doi:10.1212/WNL.58.1.143
30. Mowry EM, Krupp LB, Milazzo M, et al. Vitamin D status is associated with relapse rate in pediatric-onset multiple sclerosis. Ann Neurol. 2010;67(5):618-624. PubMed
31. Soilu-Hänninen M, Aivo J, Lindström BM, et al. A randomised, double blind, placebo controlled trial with vitamin D3 as an add on treatment to interferon β-1b in patients with multiple sclerosis. J Neurol Neurosurg Psychiatry. 2012;83(5):565-571. PubMed doi:10.1136/jnnp-2011-301876
32. Frohman EM, Brannon K, Racke MK, et al. Mycophenolate mofetil in multiple sclerosis. Clin Neuropharmacol. 2004;27(2):80-82.
33. Fernandez O, Alvarez-Cermeno JC, Arroyo-Gonzalez R, et al, for the Post-ECTRIMS Group. Review of the novelties presented at the 27th Congress of the European Committee for Treatment and Research in Multiple Sclerosis (ECTRIMS, pt II). Rev Neurol. 2012;54(12):734-749.
multicme=’1605′;