Background: A digital medicine system (DMS) has been developed to measure and report adherence to an atypical antipsychotic, aripiprazole, in psychiatric patients. The DMS consists of 3 components: ingestible sensor embedded in a medication tablet, wearable sensor, and secure mobile and cloud-based applications. An umbrella study protocol was designed to rapidly assess the technical performance and safety of the DMS in multiple substudies to guide the technology development.
Methods: Two sequential substudies enrolled 30 and 29 healthy volunteers between March-April 2014 and February-March 2015, respectively, to assess detection accuracy of the ingestible sensor by the DMS and the latency period between ingestion and detection of the ingestion by the wearable sensor or the cloud-based server.
Results: The first substudy identified areas for improvement using early versions of the wearable sensor and the mobile application. The second substudy tested updated versions of the components and showed an overall ingestion detection rate of 96.6%. Mean latency times for the signal transmission were 1.1-1.3 minutes (from ingestion to the wearable sensor detection) and 6.2-10.3 minutes (from the wearable sensor detection to the server detection). Half of transmissions were completed in < 2 minutes, and ~90% of ingestions were registered by the smartphone within 30 minutes of ingestion. No serious adverse events, discontinuations, or clinically significant laboratory/vital signs findings were reported.
Conclusions: The DMS implementing modified versions of the smartphone application and the wearable sensor has the technical capability to detect and report tablet ingestion with high accuracy and acceptable latency time.
Trial Registration: ClinicalTrials.gov identifier: NCT02091882
Developing a Digital Medicine System in Psychiatry:
Ingestion Detection Rate and Latency Period
ABSTRACT
Background: A digital medicine system (DMS) has been developed to measure and report adherence to an atypical antipsychotic, aripiprazole, in psychiatric patients. The DMS consists of 3 components: ingestible sensor embedded in a medication tablet, wearable sensor, and secure mobile and cloud-based applications. An umbrella study protocol was designed to rapidly assess the technical performance and safety of the DMS in multiple substudies to guide the technology development.
Methods: Two sequential substudies enrolled 30 and 29 healthy volunteers between March–April 2014 and February–March 2015, respectively, to assess detection accuracy of the ingestible sensor by the DMS and the latency period between ingestion and detection of the ingestion by the wearable sensor or the cloud-based server.
Results: The first substudy identified areas for improvement using early versions of the wearable sensor and the mobile application. The second substudy tested updated versions of the components and showed an overall ingestion detection rate of 96.6%. Mean latency times for the signal transmission were 1.1–1.3 minutes (from ingestion to the wearable sensor detection) and 6.2–10.3 minutes (from the wearable sensor detection to the server detection). Half of transmissions were completed in < 2 minutes, and ~90% of ingestions were registered by the smartphone within 30 minutes of ingestion. No serious adverse events, discontinuations, or clinically significant laboratory/vital signs findings were reported.
Conclusions: The DMS implementing modified versions of the smartphone application and the wearable sensor has the technical capability to detect and report tablet ingestion with high accuracy and acceptable latency time.
Trial Registration: ClinicalTrials.gov identifier: NCT02091882
J Clin Psychiatry
dx.doi.org/10.4088/JCP.16m10643
© Copyright 2016 Physicians Postgraduate Press, Inc.
aClinical Research & Development, Otsuka Pharmaceutical Development & Commercialization, Inc, Princeton, New Jersey
bODH, Inc, Princeton, New Jersey
*Corresponding author: Deborah Profit, PhD, Otsuka Pharmaceutical Development & Commercialization, Inc, 508 Carnegie Center Blvd, Ste 300, Princeton, NJ 08540
([email protected]).
Patients with serious mental illness (SMI) such as schizophrenia, bipolar disorder, or major depressive disorder (MDD) are often poorly adherent to prescribed medication.1–3 For example, a retrospective analysis of adherence to second-generation antipsychotics at 6 months after hospital discharge reported mean medication possession ratios (MPRs) of 55.1% and 37.3% among patients with schizophrenia and bipolar disorder, respectively.4 MPR is the ratio of the total number of days supplied with medication within the follow-up refill period to the total number of days in the follow-up. Further, a systematic review of 10 studies in schizophrenia that defined adherence as “regularly taking medications as prescribed” reported a mean rate of medication nonadherence of 41.2%.5 Poor adherence is associated with suboptimal treatment response that results in a greater risk of relapse6,7; poor functional outcomes including arrests, violence, and impaired mental functioning1; and elevated health resource utilization.2,8 Long-acting injectable (LAI) formulations of oral antipsychotics have the potential to improve adherence; however, broad acceptance of the LAIs as a therapeutic option has been a challenge.9
Measuring adherence is difficult in clinical practice and most often relies on patient self-report (using direct questioning or psychometric instruments) or assessments provided by the health care provider or caregiver.10 These subjective methods can be easily implemented in the clinical setting but have questionable accuracy and tend to underestimate nonadherence.11,12 The currently available objective methods to assess patient adherence include pill counts, electronic devices that capture pill container openings such as Medication Event Monitoring System (MEMS) bottle caps, and pharmacy refill records.13 Electronic bottle caps and smart pill boxes, often considered the gold standard for assessing adherence,14 are limited to reporting the event of container opening. None of these measures can confirm medication ingestion. Biologic assays to detect the presence of a drug or its metabolite in bodily fluids can confirm medication ingestion but require an office visit, invasive collection techniques, and laboratory analysis, which are time-consuming and costly. Therefore, the shortcomings of the currently available methods underscore the unmet need to objectively assess adherence in patients with SMI.
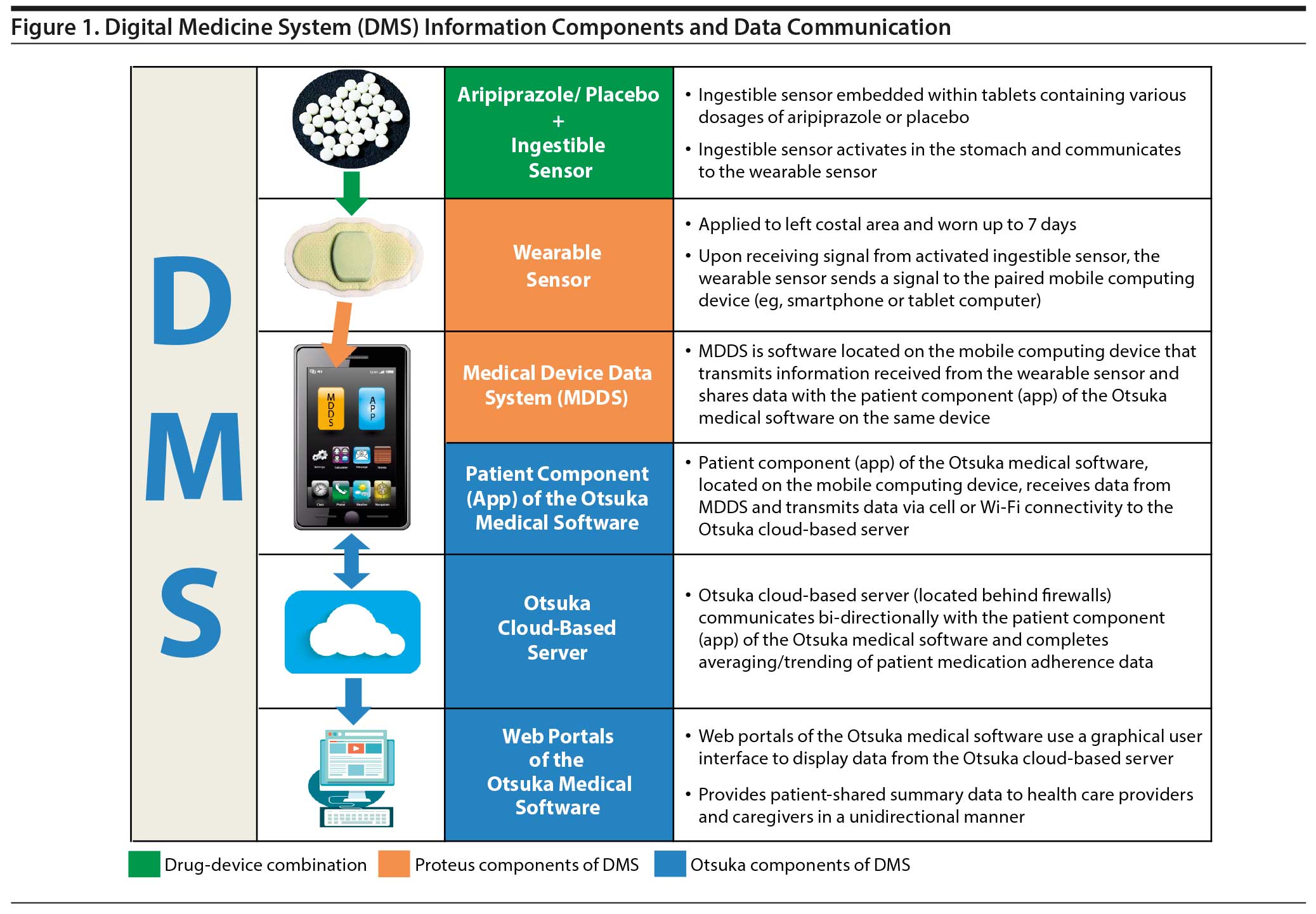
A digital medicine system (DMS) has been developed to measure and report medication adherence in patients with SMI to enable patients to stay on track with prescribed therapy and to assist health care providers with patient insights to enable therapy optimization. The DMS combines the proven safety and efficacy of orally administered aripiprazole, an atypical antipsychotic,15 with the ability to electronically confirm medication ingestion and send feedback to the patient, health care provider, and elected others such as caregivers or family members.
The DMS is an integrated product with 3 distinct components: an ingestible sensor embedded in a medication tablet (digital medicine), a wearable sensor, and secure mobile and cloud-based computing applications (Figure 1). The characteristics of the ingestible sensor have been previously described.16 Briefly, after digital medicine is ingested, a signal generated by the ingestible sensor following activation in the stomach is received by the wearable sensor. The wearable sensor communicates the data to the mobile application on the patient’s smartphone, which transmits the data to the cloud-based server. Finally, the server transmits the data to health care provider and caregiver web portals. This technology has been tested in pilot studies with healthy volunteers17 and in patients with tuberculosis,17,18 heart failure,17 and hypertension,17 as well as schizophrenia or bipolar disorder.19 The development of such a multicomponent system requires an evidence-based program that includes a series of studies aimed at assessing performance and safety and tolerability of the individual components. An umbrella master study, OSMITTER (Otsuka Study of Marker Ingested to Trigger Event Recorder; ClinicalTrials.gov identifier: NCT02091882), was designed as a unique protocol for studies enrolling healthy subjects to rapidly assess the technical performance, safety, and user satisfaction of the 3 components of the DMS, with the goal being to efficiently guide agile technology product development. This article reports results from 2 substudies of the master protocol. The aim of the substudies was to test the hypothesis that the DMS is able to track medication ingestion with accuracy > 95%, a latency time < 5 minutes between ingestion and registration by the wearable sensor, and a latency time < 120 minutes between ingestion and detection by the DMS patient application.
METHODS
OSMITTER was a nonrandomized, prospective, single-site clinical trial. The protocol was approved by the institutional review board, and informed consent was obtained from subjects prior to participation. A subject can theoretically be enrolled in 24 substudies conducted sequentially within 1 year assuming that studies are not longer than 1 day and separated by mandatory 15-day intervals. Two sequential substudies of the OSMITTER protocol (206A and 206B) were conducted from March 2014 to April 2014 and February 2015 to March 2015, respectively, to assess the ingestion sensor detection rate and latency period. Substudy A identified areas for improvement using early versions of the wearable sensor and the mobile application. Following refinement of the components, the accuracy of ingestion detection was examined in a substudy B, which tested updated versions of the wearable sensor and the mobile application and used a trial design slightly modified from that of substudy A. The 2 substudies were conducted using the same methodology with several modifications implemented into the design of substudy B. Methods for substudy B are described in detail, and differences between the substudies are noted in the individual sections.
Objectives
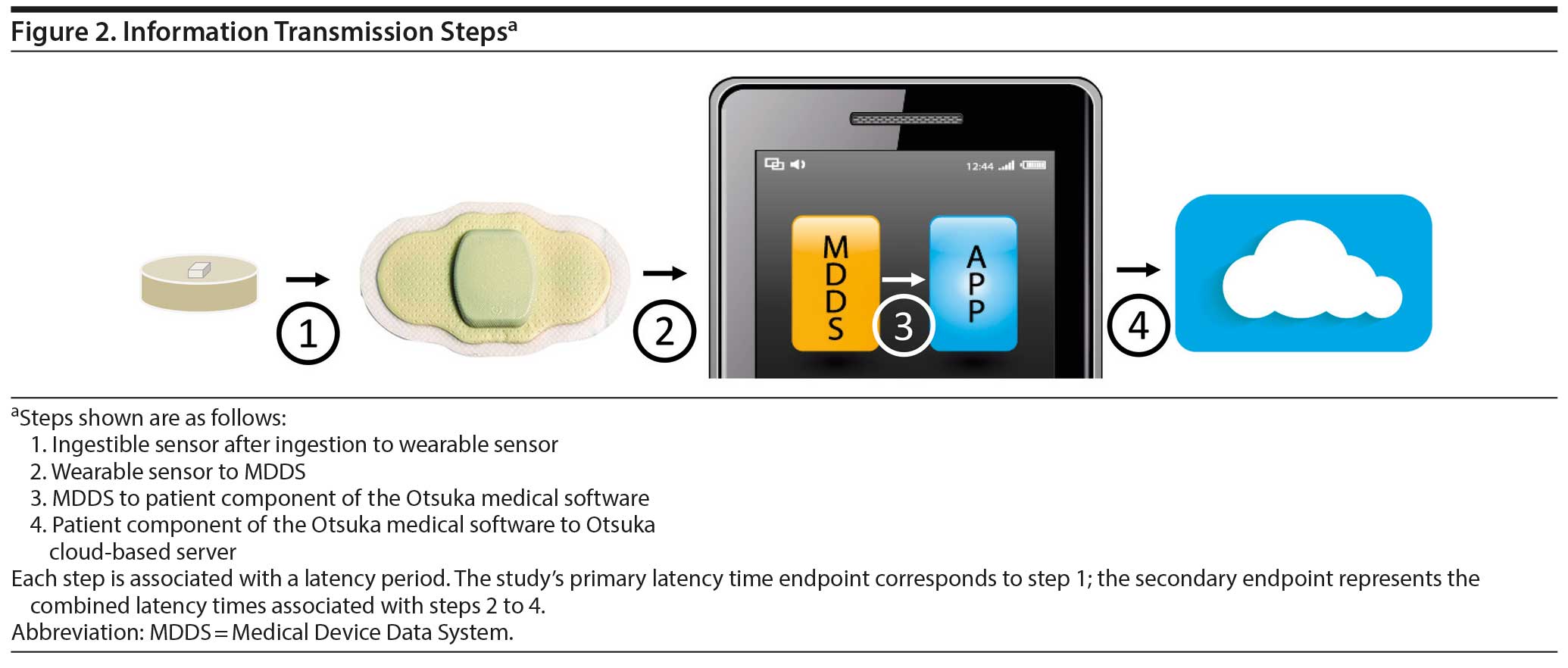
The primary objective was to measure the accuracy of detection of the ingestible sensor by the DMS after ingestion and the latency period between the ingestion time reported by clinical site staff and detection of the ingestion event by the wearable sensor. The secondary objective was to measure the latency period between detection of the ingestion event by the wearable sensor and the event detection by the Otsuka cloud-based server. In addition, safety of the DMS was also evaluated. The information transmission steps are shown in Figure 2.
Subjects and Procedures
The studies were conducted during a 1-day visit at a single clinic site with healthy volunteers, men and nonpregnant women aged 18–65 years with a body mass index of 19–32 kg/m2. Persons with a history of skin sensitivity to adhesive medical tape or metals or a history of acute or chronic dermatitis were excluded from the study. Also excluded were persons with cognitive impairments or a history of drug/alcohol dependence. Each subject was provided 1 wearable sensor and received 4 placebo tablets each embedded with an ingestible sensor. In substudy A, the ingestible sensor was embedded in a 10-mg aripiprazole tablet (taken at the initial time point) or a placebo tablet (taken at 3 following time points). The wearable sensor was paired with a compatible mobile computing device (smartphone) and placed on the subject’s torso by the clinic staff just above the left costal margin between the xyphoid to the left midaxillary line. The sensor was replaced only if improper skin contact was detected by clinic staff or the mobile device. In substudy A, the wearable sensor was replaced before each ingestion event. Subjects were instructed to ingest the tablet embedded with an ingestible sensor with approximately 240 mL of water every 2 hours (hours 0, 2, 4, and 6) for a total of 4 ingestions. The type and quantity of food consumed during the study were not specified or limited, and the subjects were not restricted in their water consumption. In substudy A, the aripiprazole tablet (hour 0) and the placebo tablets administered at hours 2 and 6 were ingested without food; the placebo tablet administered at hour 4 was ingested with a high-fat meal (fat representing ~50% of total caloric content of the meal). The protocol of substudy B required turning off personal cell phones to reduce potential Bluetooth interference and restricted placement of the study smartphone to a 3-m radius from the subject. Following the final ingestion, the subjects remained at the clinic site until the ingestion was detected by the smartphone but not for longer than 2 hours. Information about adverse events (AEs) was collected from the study participants by telephone a week after the clinic site visit.
Endpoints
The primary endpoint was accuracy of detection of the ingestible sensor by the wearable sensor; this was measured as the proportion of subjects for whom the tablet-embedded sensor was detected after directly observed ingestion by the clinic staff at each time point. The sensor ingestion detection was recorded in a timeline of an icon displayed on the smartphone and observed by the clinic staff after each scheduled ingestion event. An additional primary endpoint was the latency time between the actual ingestion and detection of the ingestion event by the wearable sensor (step 1 in Figure 2). The secondary endpoint was the latency time between detection of an ingestion event by the wearable sensor and detection of that ingestion event in the cloud-based server (combined steps 2 to 4 in Figure 2) measured as a sum of 3 signal transmissions: (a) from the wearable sensor to the medical device data system (MDDS) in the smartphone; (b) from the MDDS to the patient component of the Otsuka medical software within the smartphone; and (c) from the patient component of the Otsuka medical software to the Otsuka cloud-based server. Safety and tolerability of the system components were additional endpoints. Safety variables included assessment of the frequency of AEs, device-related AEs, serious AEs, AEs leading to discontinuation, unanticipated device-associated AEs, clinical laboratory tests (hematology, serum chemistry and urinalysis), heart rate, and blood pressure.
Statistical Analyses
The efficacy (ingestion detection accuracy and latency) and safety endpoint data were analyzed in the intent-to-treat population, which included all subjects who ingested at least 1 tablet embedded with the ingestible sensor, regardless of successful ingestion detection. The proportion of detected ingestions was calculated for each scheduled ingestion timepoint (hours 0, 2, 4, and 6) and presented with a 2-sided 95% confidence interval (CI) using the exact Clopper-Pearson Binomial method. The latency periods were summarized using descriptive statistics for each scheduled ingestion time point. AEs were coded by system organ class and Medical Dictionary for Regulatory Activities (version 17.0, www.meddra.org). All safety variable data were summarized using descriptive statistics.
RESULTS AND DISCUSSION
Substudy A
Thirty-eight subjects were screened and 30 were enrolled in the study. All 30 subjects completed the study and were included in both the endpoint and safety analyses. The subjects’ baseline characteristics are presented in Table 1.
The overall accuracy of ingestion detection, that is, the overall proportion of subjects with detected ingestion at the 4 time points, was 78.3% (94/120). Consumption of a high-fat meal 30 minutes before ingestion did not affect the accuracy of ingestion detection or the latency time (data not shown). A post hoc analysis of ingestion detection accuracy at each stage of information transmission showed a much higher rate of detection by the wearable sensor (118/120; 98.3%) that suggested a disruption in communication between the wearable sensor and the smartphone application. The analysis revealed that an early version of the smartphone application used in the study did not properly check for a complete data transfer from the wearable sensor to the application. In addition, the protocol for the substudy A did not draw attention to the option of forced data upload from the wearable sensor before removal of the sensor after each ingestion event. The combination of these 2 factors resulted in suboptimal accuracy of ingestion detection reported in the study. An updated version of the smartphone application corrected deficiencies of the early version and was designed to communicate with an updated version of the wearable sensor.
Substudy B
Thirty-five subjects were screened and 29 were enrolled in the study. All 29 subjects completed the study and were included in both the efficacy endpoint and safety analyses. The subjects’ baseline characteristics are presented in Table 1.
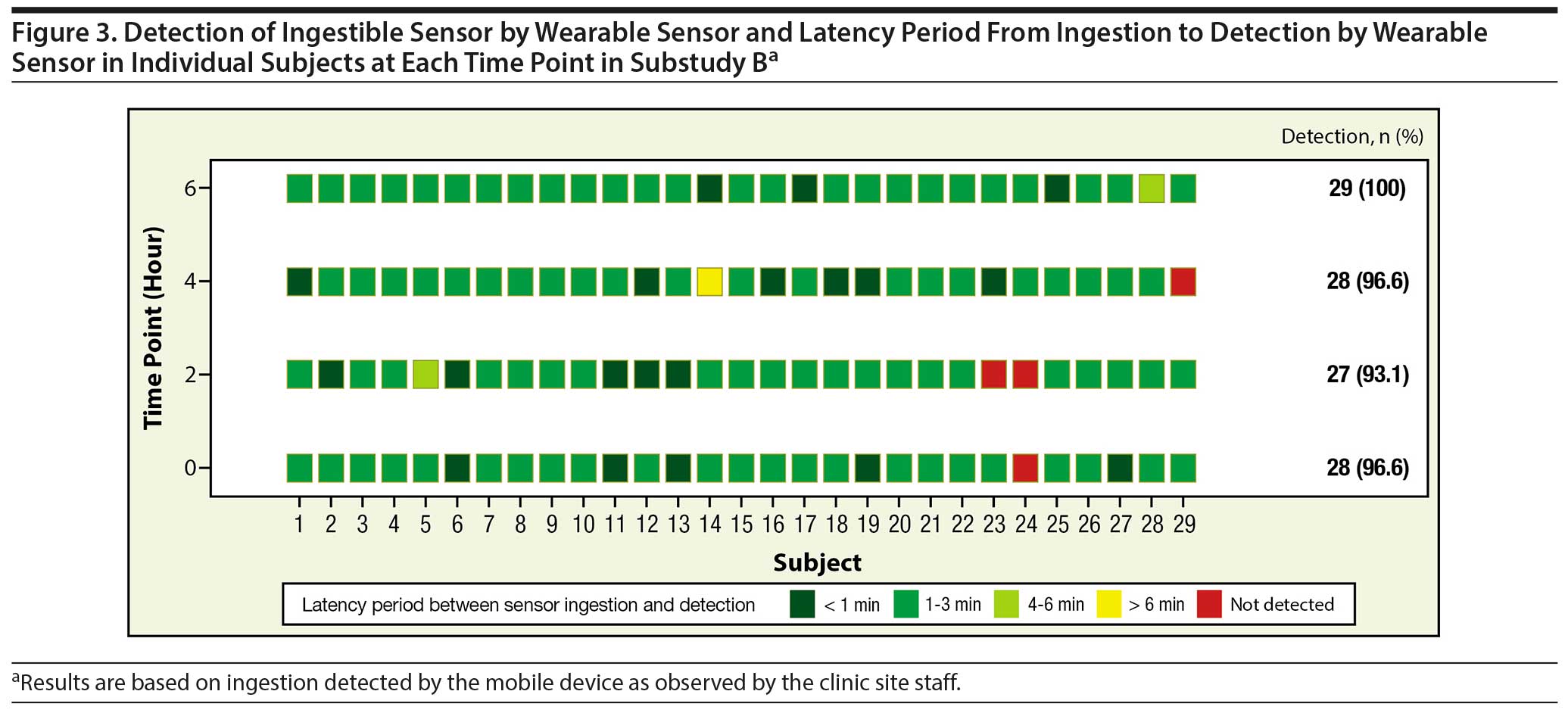
The accuracy of ingestion detection by the wearable sensor at the 4 time points was between 93.1% and 100% (Table 2). Overall, ingestion was detected in 112 of 116 (96.6%) events. This is consistent with detection accuracy reported for the ingestible sensor in previous studies.17–19 The mean latency time from actual ingestion to signal detection by the wearable sensor at the 4 time points was between 1.1 and 1.3 minutes (Table 2). The majority of ingestions (90/116; 77.6%) were detected between 1 and 3 minutes; 16.4% (19/116) of ingestions were detected in < 1 minute (Figure 3).
The mean latency time from ingestion signal detection by the wearable sensor to ingestion detection by the cloud-based server at the 4 time points was between 6.2 and 10.3 minutes (Table 2). The mean values are affected by several latency times longer than 30 minutes; it is important to note that 50% of transmissions from the wearable sensor to the server were completed in < 2 minutes, and approximately 90% (105/116) of all ingestion events were registered by the smartphone within 30 minutes from the actual ingestion. The measured latency time is a sum of 3 signal transmissions (steps 2 to 4, Figure 2). An additional analysis of latency time at each of the 3 steps showed that greatest latency occurred during signal transfer from the wearable sensor to the MDDS.
Safety analysis reported no AEs including device-related effects, no study discontinuations because of AEs, and no clinically significant laboratory or vital signs findings.
Study Limitations
The study assessed technical performance of the DMS components under experimental conditions that aimed to minimize potential interference by factors of a real world setting. The study was conducted in healthy subjects using placebo instead of medication tablets and followed a protocol that required assisted administration of the wearable sensor and its pairing to a smartphone; in the real world, patients are expected to use the system after initial training independently and/or with assistance of a caregiver. Studies testing the usability of the DMS in the intended user population have been conducted. Preliminary results indicate that ~80% of patients with schizophrenia are able to apply the wearable sensor and pair it with the smartphone application independently or with minimal assistance.20 Lastly, the experimental setting restricted distance between the subject and the smartphone and reduced potential interference from other mobile devices. It should be noted that the interference between personal mobile devices and the study smartphones observed during substudy A that led to protocol modification of substudy B will likely be reduced in real-world settings because patients will be able to download the application on their personal smartphones. It is also expected that technical improvements of the system will further reduce interference.
CONCLUSIONS
Accuracy of ingestion detection and latency period are critical parameters of the DMS that required a creative approach implementing a unique study design to rapidly assess and optimize performance of the system’s components. The results demonstrate that updated versions of the smartphone application and the wearable sensor substantially improved accuracy of ingestion detection by the DMS when compared with that using the original versions. The wearable sensor of the DMS detected ingestion events effectively (~97%) and with a minimal average delay (~1 min). The data transmission from the wearable sensor to the cloud-based server was associated with an average delay of approximately 6 to 10 minutes, and the signal transfer from the wearable sensor to the MDDS on the patient smartphone represented the majority of the overall latency time. Approximately 90% of ingestion events were registered by the smartphone within 30 minutes from the actual ingestion, indicating that delays beyond 30 minutes were uncommon. No safety issues were reported, demonstrating good tolerability of the DMS components. Overall, the results show that the DMS has the technical capability to detect and report tablet ingestion with high accuracy and acceptable latency time.
Submitted: January 6, 2016; accepted April 29, 2016.
Online first: July 5, 2016.
Drug names: aripiprazole (Abilify).
Potential conflicts of interest: Drs Profit, Rohatagi, Zhao, and Peters-Strickland are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. Drs Hatch and Docherty are employees of ODH, Inc.
Funding/support: The study was funded by Otsuka Pharmaceutical Development & Commercialization, Inc.
Role of the sponsor: The funder is fully responsible for the conduct, interpretation, and reporting of this study.
Acknowledgments: Editorial support for development of this manuscript was provided by C4 MedSolutions, LLC (Yardley, PA), a CHC Group company, and was funded by Otsuka Pharmaceutical Development & Commercialization, Inc.
REFERENCES
1. Ascher-Svanum H, Faries DE, Zhu B, et al. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 2006;67(3):453–460. doi:10.4088/JCP.v67n0317 PubMed
2. Hong J, Reed C, Novick D, et al. Clinical and economic consequences of medication non-adherence in the treatment of patients with a manic/mixed episode of bipolar disorder: results from the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) study. Psychiatry Res. 2011;190(1):110–114. doi:10.1016/j.psychres.2011.04.016 PubMed
3. Liu X, Chen Y, Faries DE. Adherence and persistence with branded antidepressants and generic SSRIs among managed care patients with major depressive disorder. Clinicoecon Outcomes Res. 2011;3:63–72. PubMed
4. Berger A, Edelsberg J, Sanders KN, et al. Medication adherence and utilization in patients with schizophrenia or bipolar disorder receiving aripiprazole, quetiapine, or ziprasidone at hospital discharge: a retrospective cohort study. BMC Psychiatry. 2012;12(1):99. doi:10.1186/1471-244X-12-99 PubMed
5. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909. doi:10.4088/JCP.v63n1007 PubMed
6. Caseiro O, Pérez-Iglesias R, Mata I, et al. Predicting relapse after a first episode of non-affective psychosis: a three-year follow-up study. J Psychiatr Res. 2012;46(8):1099–1105. doi:10.1016/j.jpsychires.2012.05.001 PubMed
7. Novick D, Haro JM, Suarez D, et al. Predictors and clinical consequences of non-adherence with antipsychotic medication in the outpatient treatment of schizophrenia. Psychiatry Res. 2010;176(2–3):109–113. doi:10.1016/j.psychres.2009.05.004 PubMed
8. Ascher-Svanum H, Zhu B, Faries DE, et al. The cost of relapse and the predictors of relapse in the treatment of schizophrenia. BMC Psychiatry. 2010;10(1):2. doi:10.1186/1471-244X-10-2 PubMed
9. Waddell L, Taylor M. Attitudes of patients and mental health staff to antipsychotic long-acting injections: systematic review. Br J Psychiatry suppl. 2009;52(52):S43–S50. doi:10.1192/bjp.195.52.s43 PubMed
10. Velligan DI, Lam YW, Glahn DC, et al. Defining and assessing adherence to oral antipsychotics: a review of the literature. Schizophr Bull. 2006;32(4):724–742. doi:10.1093/schbul/sbj075 PubMed
11. Byerly MJ, Thompson A, Carmody T, et al. Validity of electronically monitored medication adherence and conventional adherence measures in schizophrenia. Psychiatr Serv. 2007;58(6):844–847. doi:10.1176/ps.2007.58.6.844 PubMed
12. Acosta FJ, Bosch E, Sarmiento G, et al. Evaluation of noncompliance in schizophrenia patients using electronic monitoring (MEMS) and its relationship to sociodemographic, clinical and psychopathological variables. Schizophr Res. 2009;107(2-3):213–217. doi:10.1016/j.schres.2008.09.007 PubMed
13. Sajatovic M, Velligan DI, Weiden PJ, et al. Measurement of psychiatric treatment adherence. J Psychosom Res. 2010;69(6):591–599. doi:10.1016/j.jpsychores.2009.05.007 PubMed
14. Riley W, Velligan D, Sajatovic M, et al. Adherence to psychiatric treatments. CML Psychiatry. 2009;20(4):89–96.
15. Abilify [package insert]. Tokyo, Japan: Otsuka Pharmaceutical Co, Ltd; 2014.
16. Hafezi H, Robertson TL, Moon GD, et al. An ingestible sensor for measuring medication adherence. IEEE Trans Biomed Eng. 2015;62(1):99–109. doi:10.1109/TBME.2014.2341272 PubMed
17. Au-Yeung KY, Moon GD, Robertson TL, et al. Early clinical experience with networked system for promoting patient self-management. Am J Manag Care. 2011;17(7):e277–e287. PubMed
18. Belknap R, Weis S, Brookens A, et al. Feasibility of an ingestible sensor-based system for monitoring adherence to tuberculosis therapy. PLoS ONE. 2013;8(1):e53373. doi:10.1371/journal.pone.0053373 PubMed
19. Kane JM, Perlis RH, DiCarlo LA, et al. First experience with a wireless system incorporating physiologic assessments and direct confirmation of digital tablet ingestions in ambulatory patients with schizophrenia or bipolar disorder. J Clin Psychiatry. 2013;74(6):e533–e540. doi:10.4088/JCP.12m08222 PubMed
20. Peters-Strickland T, Pestreich L, Hatch A, et al. A multicenter, 8-week, open-label study to assess usability of a digital health feedback system in adult patients with schizophrenia treated with oral aripiprazole. American Psychiatric Association 169th Annual Meeting. May 14–18, 2016; Atlanta, GA.
This PDF is free for all visitors!





