Abstract
Persons with mental health disorders are at increased risk of dental disease, including lost teeth. Dental implants are the preferred option for most persons who have lost teeth. Recent studies suggest that antidepressant drugs, especially the selective serotonin reuptake inhibitors, are associated with an increased risk of dental implant failure. This article provides a background about the epidemiology of loss of teeth, the causes of tooth loss, the need to replace lost teeth, and the use of dental implants to replace lost teeth. Two meta-analyses of retrospective cohort studies of the association between antidepressant use and implant failure are examined in detail. One meta-analysis included 6 studies and the other, 10 studies. An additional retrospective cohort study, published after the meta-analyses, is also examined. In summary, there is consistent evidence for a higher risk of implant failure in patients taking antidepressants, and for a higher number of implants failing in patients taking antidepressants, relative to patients not taking antidepressants. Broad findings were that, at the patient level, implant failure occurred in 6%–23% of antidepressant users vs 2%–8% of nonusers, and at the implant level, implant failure occurred in 6%–22% of antidepressant users vs 2%–9% of nonusers. Because unadjusted risks were more than doubled in antidepressant users, it implies that, in the real world, antidepressant use is a clinically important marker for risk of implant failure; it is hard to draw cause and effect inferences from the studies reviewed because of inadequacies in study designs and statistical methods. Action points are that antidepressant users should be educated about the risk of implant failure, and vigorous efforts should be made to identify and negate, to the extent possible, other risk factors for implant failure in these patients. Suggestions are offered for future research in the field.
J Clin Psychiatry 2026;87(2):26f16375
Author affiliations are listed at the end of this article.
Oral health and dental health may be poor in persons with mental health disorders, especially persons with major mental illness.1–3 Adding to the burden, medications used to treat mental health disorders may carry oral health risks; as an example, antidepressant drugs have long been associated with dry mouth and dental caries.4
People with oral health disorders are at increased risk of tooth loss, and those who lose teeth may opt for dental implants. People with depression, poor oral health, and resultant loss of teeth may also opt for dental implants. During the past decade, studies have suggested that antidepressant drugs may increase the dental implant failure risk.5,6 This article therefore examines the current status of the association between antidepressant use (especially selective serotonin reuptake inhibitor [SSRI] use) and the risk of dental implant failure. The article focuses on 2 recent meta-analyses5,6 and on 1 observational study7 that was published after the meta-analyses.
Tooth Loss
People lose permanent teeth for various reasons, such as trauma, dental decay, and gum disease. Risk factors for loss of teeth include older age, poor oral hygiene, smoking, nutritional disorders, diabetes mellitus, other chronic medical conditions, and osteoporosis.8–10 Drugs may contribute to the risk. As examples, anticholinergic drugs that cause dry mouth can predispose to dental decay, periodontal disease, and tooth loss.11
People lose teeth at all ages. A little over 2 decades ago, in a population-representative metropolitan sample in Brazil, 94% of 974 subjects aged 30–103 (mean, 49) years were found to have lost a mean of 11 teeth. Subjects had lost a mean of 5.5 teeth in the 30–39 years age group and a mean of 20.2 teeth in the >60 years age group.12 A survey in the US (2011–2012) found that 52% of adults aged 20–64 years had lost at least 1 tooth. This figure was 66% vs 33% for adults aged 40–64 years vs those aged 20–39 years.13 More recently, in a 2018–2019 population-representative urban and rural sample in a northeastern Indian district, 30.6% of 1,540 adults aged 20–40 years were found to have lost at least 1 tooth.14
Disadvantages of Lost Teeth
Lost teeth are cosmetically displeasing. More importantly, lost teeth result in poorer masticatory function, resorption of alveolar bone, and shifting of adjacent teeth; downstream consequences include overuse and wearing out of the remaining teeth, developmental of new dental problems, and development of temporomandibular joint problems related to chewing more on one side than on the other. The larger the number of teeth lost, the poorer the quality of diet and quality of life, and the higher the risk of nutritional disorders, metabolic disturbances, and earlier mortality.15–18
Dental Implants
Dental implants to replace lost teeth had been attempted for millennia. Although many experiments with dental implants were described from 1913 onward, the first osseointegrated implant was probably placed in 1965.19 There were progressive improvements and innovations in the field, subsequently, and currently dental implants are considered to be a more efficient, stronger, and longer lasting solution for lost teeth than dental bridges and removable dentures. Dental implants also offer better masticatory function and gustatory experience than removable dentures.20
Implant Failure
Dental implant failure is usually defined as any event resulting in the removal of the implant. Implants fail in a small but clinically significant proportion of patients; the overall failure rate expectedly increases across time. In a study of 1,611 patients, implants failed in 119 (7.4%) patients at a 1-year follow-up.7 Among 5,456 consecutive patients who had received dental implants and who were followed for a median of 5.3 years, 529 (9.7%) patients experienced implant failure.21 In a smaller study (n=112), the implant failure rate was 4.2% at a 5-year follow-up and 7.3% at a 10-year follow-up.22 In a study of 916 implants in 490 patients who were followed for 0.3 to 5.6 years, 48 (5.2%) implants failed.23 A review and consensus report stated the failure rate to range from 0% to 13.3%, depending on the type of implant, across 1–5 years of follow-up.24
Risk factors for dental implant failure are similar to those for tooth loss. Older age, smoking, alcohol use, diabetes mellitus, debilitation, proton pump inhibitor use, and bisphosphonate use have all been associated with implant failure.7,25 Antidepressant treatment, with SSRIs in particular, has also been associated with implant failure.
Antidepressants and Bone Health: Clinical Data
The survival of dental implants depends on osseointegration and the stability thereof; so, any variable that predisposes to osteoporosis or otherwise weakens bone could increase the risk of implant failure. In this context, serotonin has been found to have a complex effect on bone resorption and bone remodeling; central serotonergic mechanisms increase bone formation, whereas peripheral serotonergic mechanisms increase bone loss.26 What do the clinical data show?
A systematic review and meta-analysis (SRMA) of observational studies found that SSRIs were associated with reduced bone mineral density in the lumbar spine (standardized mean difference, –0.40; 95% CI, –0.79 to 0.00) but not at the femoral neck or of the total hip.27 In another SRMA, in randomized, placebo-controlled trials conducted in stroke survivors, SSRIs were found to increase the risk of bone fractures (risk ratio [RR], 2.36; 95% CI, 1.64–3.39) without an associated increase in the risk of seizures or falls.28
In an SRMA of observational studies in women aged 40 years and older, antidepressants were associated with an increased risk of fragility fractures (hazard ratio [HR], 1.62; 95% CI, 1.15–2.28). In a subgroup analysis, SSRIs were also observed to be associated with increased risk (HR, 1.36; 95% CI, 1.20–1.55).29
In a large SRMA of 14 case-control and 23 cohort studies that included both men and women, SSRIs were associated with an increased risk of fracture in both case-control (RR, 1.80; 95% CI, 1.58–2.03) and cohort (RR, 1.51; 95% CI, 1.39–1.64) studies. The increased risk was observed regardless of study period, geographical origin of the studies, duration of SSRI use, defined daily dose, and site of the fracture. The risk remained increased after adjusting for age, sex, depression, and physical activity. However, the risk expectedly attenuated in studies that adjusted for bone mineral density and osteoporosis.30
If these findings related to bone health can be generalized to the mandible and maxilla, then antidepressants may also be associated with an increased risk of implant failure. This concern is addressed in the sections that follow.
SSRIs and Implant Failure: Meta-Analysis5
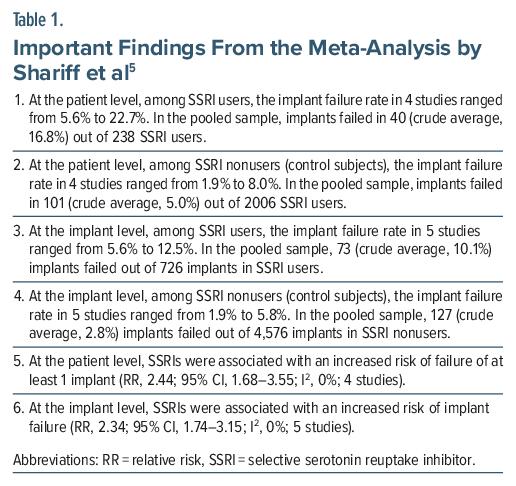
Shariff et al5 described an unregistered SRMA of the association between SSRI use and dental implant failure. These authors searched 3 electronic databases and reference lists of relevant articles and identified 6 retrospective cohort studies that had been conducted in adults and that had at least 6 months of follow-up data.
These studies had been conducted in the US, Canada, Sweden, Turkey, and India and were published between 2014 and 2021. The mean/median age of the samples in the studies ranged from 51 to 67 years. The mean/ median follow-up duration ranged from 1.8 to 7.5 years. The studies included a total of 2,959 patients who had received 7,122 implants.
Important findings from the study are presented in Table 1. In summary, relative to SSRI nonusers, SSRI users were more than twice as likely to experience at least 1 implant failure (implant failure at the patient level), and, relative to implants in SSRI nonusers, implants in SSRI users were more than twice as likely to fail (implant failure at the implant level).
Antidepressants and Implant Failure: Meta-Analysis6
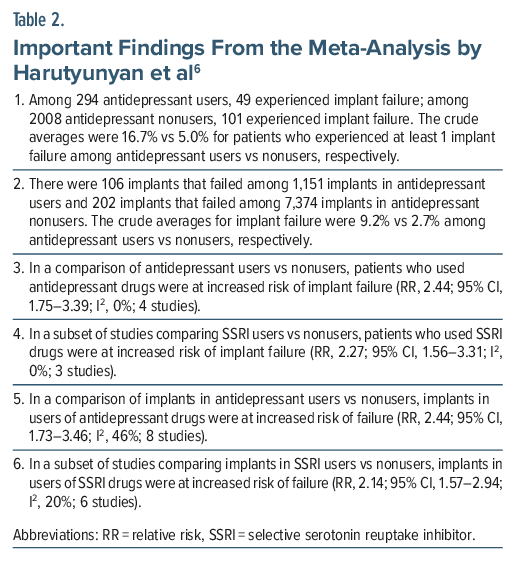
Harutyunyan et al6 described a PROSPERO-registered SRMA of the association between antidepressant use and dental implant failure. These authors searched 3 electronic databases, reference lists of relevant articles, and contents of relevant journals and identified 1 prospective and 9 retrospective cohort studies, published between 2008 and 2021, that were relevant to their objectives. There was only partial overlap between the studies examined in the previous meta-analysis5 and this meta-analysis.
In this meta-analysis, in 4 studies in the patient-level analysis, there were 294 antidepressant users and 2008 antidepressant nonusers. In 8 studies in the implant-level analysis, there were 1,151 implants in antidepressant users and 7,374 implants in antidepressant nonusers. Most of the patients in most of the studies appeared to be >50 years old, but an accurate number could not be obtained from the data presented. The mean/median follow-up duration, where stated, ranged from 21.5 months to 7.5 years.
Important findings from the study are presented in Table 2. The conclusions were similar to those of the meta-analysis by Shariff et al5: Antidepressants (and SSRIs) were associated with a more than doubled risk of implant failure in both patient-level and implant-level analyses.
Antidepressants and Implant Failure: Cohort Study7
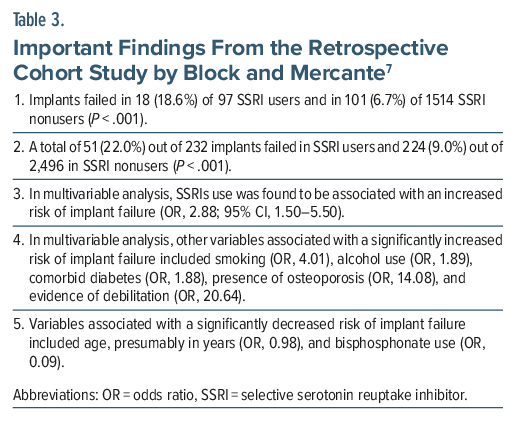
Block and Mercante7 described a retrospective cohort study of the relationship between SSRI use and dental implant failure. This study is described because it was published after the meta-analyses described above (Shariff et al, 20235; Harutyunyan et al, 20246) and so had not been included in the meta-analyses.
These authors7 extracted data of all patients seen in a private clinic between 2007 and 2020 who had received dental implants and for whom 1-year follow-up data were available. The sample comprised 1,611 patients among whom 97 (6%) had been exposed to SSRIs. The mean age of the sample was 57 years. The sample was 45% male. These patients had received a mean of 2 implants, each.
The relationship between SSRI exposure (presumably at the time of implant placement) and implant failure on or before the 1-year follow-up date was examined after adjusting for age, sex, implant location, smoking, diabetes, hypertension, peripheral vascular disease, depression, opioid use, alcohol use, osteoporosis, bisphosphonate use, and an index of frailty.
Important findings from the study are presented in Table 3. In summary, the implant failure rate in SSRI users vs nonusers was 18.6% vs 6.7% at the patient level and 22.0% vs 9.0% at the implant level. SSRI use was associated with nearly trebled odds of implant failure.
Limitations of the Meta-Analyses5,6
The meta-analyses5,6 suffered from 3 major limitations. First, implant failure would have occurred at different times in different persons, perhaps after a few months in some, after a few years in others, and never in still others. Also, different patients would have been followed for different durations, and some might have dropped out before the occurrence of an implant failure event. The appropriate approach in such situations is to use time-to-event analysis and to obtain a hazard ratio after adjusting for covariates and confounds in a Cox regression.31 However, the authors of both meta-analyses extracted only number of events and total events (eg, number of patients with implant failures and total number of patients with implants in antidepressant users and nonusers) and calculated RRs. In such analyses, important data are lost.
Second, the RRs thus calculated for each study (and pooled in meta-analyses) were not adjusted for covariates and confounds. The results of the meta-analyses, consequently, only provide information about crude (“real world”) associations between antidepressant use and implant failure. The results do not provide information about the unique relationship between antidepressant use and implant failure, as would have emerged in pooling of adjusted risks. Therefore, the results do not have any implications whatsoever for potential cause-effect relationships between antidepressant use and implant failure.
As a side note here, many studies adjusted for implant failure risk factors through study selection criteria. For example, some studies excluded patients with diabetes, patients with other endocrine disorders, patients with osteoporosis, patients receiving corticosteroids, etc, making it unnecessary to adjust for these variables. However, in all studies many risk factors remained unaddressed.
Third, using the RR for the implant-level analysis is especially fallacious because different patients would have contributed different numbers of implants to both total implants and failed implants categories; so, the implant units in each category were not independent of each other. That is, it is likely that, within a category, patients with many risk factors for implant failure might have contributed more units of data to the failed implants tally than patients with few risk factors. This bias would not have been captured by the RR. The data should have been analyzed using Poisson regression, and this analysis should have been performed at the source study level. If Poisson regression analyses were unavailable in the source studies, implant-level meta-analysis should not have been conducted.
Limitations of the Cohort Study7
The cohort study by Block and Mercante7 did not present a time-to-event analysis for patient-level implant failure; why this is important was explained in the previous section. The study presented a χ2 P value for the implant-level analysis; why this is fallacious can also be inferred from the explanation in the previous section.
The study presented a multivariable logistic regression analysis (which is not a time-to-event analysis) that included many risk factors for a patient-level implant failure analysis. This is a matter of concern. Of further concern is that the regression was run as a backward stepwise procedure. Such a procedure obtains inaccurate odds ratios (ORs) because clinically relevant risk factors would have been left out of the regression merely because their association with implant failure did not reach statistical significance in the sample. Stepwise regressions are generally discouraged in research.
The multivariable logistic regression analysis threw up an unexpected finding: that bisphosphonate use was associated with an extraordinarily large protective effect against implant failure. The OR was 0.091, which translates to an E-value of 21.47. This E-value suggests that the finding is valid because a confound, or set of confounds, would need to be associated with both bisphosphonate use and implant failure by an OR of at least 21.47, each, to bring the OR for bisphosphonates to null (OR=1.00), given the set of risk factors identified in the final iteration of the stepwise analysis.32 Curiously, the risk for implant failure with bisphosphonates was actually null (RR = 1.0) in bivariate analysis. Furthermore, 2 recent meta-analyses obtained findings in the opposite direction. Lin et al33 found that bisphosphonates were associated with implant failure at the implant level (RR, 1.74; 95% CI, 1.10–2.75) but not at the patient level (RR, 1.01; 95% CI, 0.35–2.91) and Pishan et al,34 studying postmenopausal women, found that bisphosphonates were associated with implant failure at the implant level (RR, 1.73; 95% CI, 1.03–2.83). The cohort study finding for bisphosphonates therefore weakens the reader’s confidence in the analysis. A possible mitigating explanation is that bisphosphonates were protective after adjusting for the presence of osteoporosis, which is an indication for bisphosphonate use.
A possible strength of the cohort study is that the authors adjusted for depression; however, depression was operationalized by self-report or by “medications.” Presumably, SSRIs were excluded from the definition of medications, because 71% vs 8% of SSRI users vs nonusers were classified as having depression.
General Limitations of the Studies5–7
SSRI or antidepressant use ought to have been ascertained at the time of first implant, but this was not explicitly stated in any of the studies. No study presented analyses for dose of drug (in defined daily dose units) or duration of exposure prior to the first implant. No study presented data on the nature, severity, or duration of depression, or whether the implant procedures were conducted during the acute or maintenance phase of antidepressant therapy. Additionally, no study examined study site, type and quality of the implant, and surgeon skills as risk modifying variables.
Interpretation
The descriptive statistics data show a consistently higher risk of implant failure in patients taking antidepressants and a higher number of implants failing in patients taking antidepressants, relative to patients not taking antidepressants.5,6 At the patient level, implant failure occurred in 6%–23% of antidepressant users vs 2%–8% of nonusers. And, at the implant level, implant failure occurred in 6%–22% of antidepressant users vs 2%–9% of nonusers. Given that unadjusted risks were more than doubled in antidepressant users, it implies that, in the real world, antidepressant use is a clinically important marker for risk of dental implant failure. It is hard to draw stronger conclusions (eg, cause and effect inferences) from the meta-analyses, and the other data reviewed in this article, because when study designs and methods of analysis are suboptimal, valid inferences cannot be drawn.
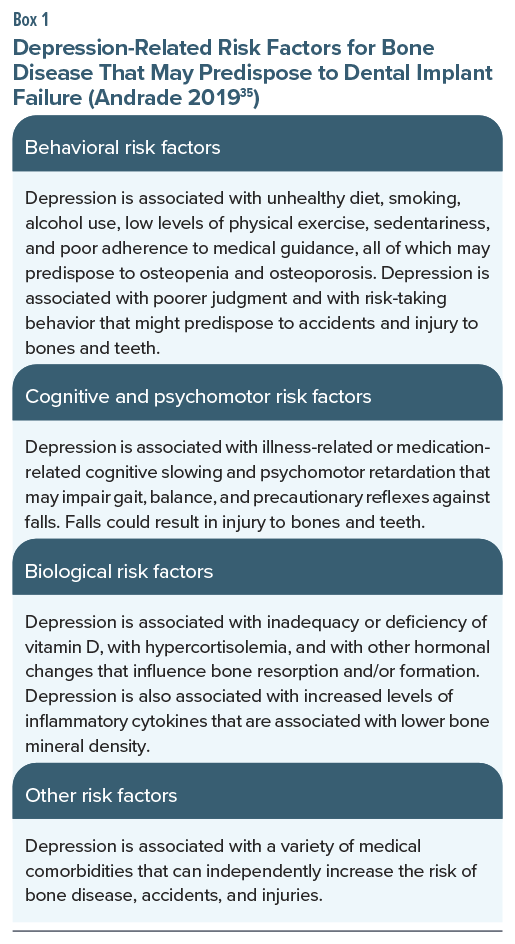
If the association between antidepressant use and dental implant failure is not cause and effect, what explains the association? One explanation is that antidepressant use is a marker for other risk factors for implant failure; examples of such risk factors are alcohol use and frailty.7 Another explanation is that antidepressants are most commonly used to treat depression, and depression is itself associated with a large number of risk factors for bone disease and hence dental implant failure (Box 1).35
The above notwithstanding, a causal role for antidepressants cannot be ruled out because a meta-analysis of 4 randomized controlled trials (RCTs) found that, after 6 months of treatment, fluoxetine and citalopram were associated with a more than doubled risk of bone fractures.28 Because the RCT is a gold standard research design for drawing causal inferences, this finding suggests that antidepressants, or at least SSRIs, predispose to bone disease and may thereby directly increase the implant failure risk.
Implications
From the perspective of the psychiatrist, the best-case scenario is that antidepressant use is merely a marker for dental implant failure. The worst-case scenario is that antidepressant drugs, especially SSRIs, directly predispose to dental implant failure.
If antidepressant use is no more than a marker, all that is necessary is that patients should be alerted about the risk of implant failure, and vigorous efforts should be made to identify and negate, to the extent possible, other risk factors for implant failure.
If antidepressant use is causal for implant failure, action points are exactly the same as indicated above. Stopping antidepressant treatment is unlikely to be a good idea because we do not know how long it takes for the antidepressant-related adverse mechanisms (if any, and whatever they may be) to wear off. For the same reason, in the absence of evidence, drug holidays cannot be recommended. Stopping antidepressant treatment is especially unlikely to be a good idea if there is a risk of relapse into depression.
Parting Notes
At the risk of stating the obvious, given that RCTs would be hard to conduct, observational studies of better quality are required. These would need to be large and would need to collect accurate data on a large number of relevant covariates and confounds. The data would need to be analyzed using appropriate models of regression, simple suggestions for which were made in earlier sections. Special study designs could include comparisons of former users of antidepressants with never users and former users with current users.
Article Information
Published Online: March 18, 2026. https://doi.org/10.4088/JCP.26f16375
© 2026 Physicians Postgraduate Press, Inc.
To Cite: Andrade C. Association of selective serotonin reuptake inhibitor and other antidepressant drugs with dental implant failure. J Clin Psychiatry. 2026;87(2):26f16375.
Author Affiliations: Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India; Department of Psychiatry, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
Corresponding Author: Chittaranjan Andrade, MD, Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore 560029, India ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
 Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India. Please contact Chittaranjan Andrade, MD, at Psychiatrist.com/contact/andrade.
References (35)

- Ajwani S, Sureshkumar P, Bhole S, et al. Understanding the oral health status and factors affecting poor oral health in people living with severe mental illness: a cross-sectional study. Aust Dent J. 2025;22.
- Wölfle UC, Beck F, Werner N, et al. Association of psychosis and oral health: case-control study. Clin Oral Investig. 2025;29(9):397. PubMed CrossRef
- Jerjes W. The critical intersection of mental health and oral health in severe mental disorders. Clin Oral Investig. 2024;28(11):627. PubMed CrossRef
- Peeters FP, deVries MW, Vissink A. Risks for oral health with the use of antidepressants. Gen Hosp Psychiatry. 1998;20(3):150–154. PubMed CrossRef
- Shariff JA, Gurpegui Abud D, Bhave MB, et al. Selective serotonin reuptake inhibitors and dental implant failure: a systematic review and meta-analysis. J Oral Implantol. 2023;49(4):436–443. PubMed CrossRef
- Harutyunyan L, Lieuw K, Yang B, et al. The effect of antidepressants on dental implant failure: a systematic review and meta-analysis. Int J Oral Maxillofac Implants. 2024;39(5):665–673. PubMed CrossRef
- Block MS, Mercante D. Selective serotonin reuptake inhibitors May increase implant failure. J Oral Maxillofac Surg. 2025;83(5):585–591. PubMed CrossRef
- Gabiec K, Bagińska J, Łaguna W, et al. Factors associated with tooth loss in general population of Bialystok, Poland. Int J Environ Res Public Health. 2022;19(4):2369. PubMed CrossRef
- Alobaidi F, Heidari E, Sabbah W. Systematic review of longitudinal studies on the association between cluster of health-related behaviors and tooth loss among adults. Acta Odontol Scand. 2024;83:54–68. PubMed CrossRef
- Zhang Y, Leveille SG, Shi L. Multiple chronic diseases associated with tooth loss among the US adult population. Front Big Data. 2022;5:932618. PubMed CrossRef
- Kakkar M, Barmak AB, Arany S. Anticholinergic medication and dental caries status in middle-aged xerostomia patients-a retrospective study. J Dent Sci. 2022;17(3):1206–1211. PubMed CrossRef
- Susin C, Oppermann RV, Haugejorden O, et al. Tooth loss and associated risk indicators in an adult urban population from south Brazil. Acta Odontol Scand. 2005;63(2):85–93. PubMed CrossRef
- Dye B, Thornton-Evans G, Li X, et al. Dental caries and tooth loss in adults in the United States, 2011-2012. NCHS Data Brief. 2015;197:197. PubMed
- Barman J, Kalita C, Baruah R, et al. Tooth loss and its risk factors among the young adults in the Kamrup (Metro) district of Assam: an epidemiological study. J Indian Assoc Public Health Dent. 2022;20(2):159–167. CrossRef
- Craddock HL. Consequences of tooth loss (part 2): dentist considerations-restorative problems and implications. SADJ. 2010;65(7):294–296. PubMed
- Emami E, de Souza RF, Kabawat M, et al. The impact of edentulism on oral and general health. Int J Dent. 2013;2013:498305. PubMed CrossRef
- Koka S, Gupta A. Association between missing tooth count and mortality: a systematic review. J Prosthodont Res. 2018;62(2):134–151. PubMed CrossRef
- Kim SY, Lee CH, Yoo DM, et al. Is the number of missing teeth associated with mortality? A longitudinal study using a national health screening cohort. Front Med. 2022;9:837743. PubMed CrossRef
- Abraham CM. A brief historical perspective on dental implants, their surface coatings and treatments. Open Dent J. 2014;8:50–55. PubMed CrossRef
- Misch CE. The importance of dental implants. Gen Dent. 2001;49(1):38–45. PubMed
- Carr AB, Gonzalez RLV, Jia L, et al. Relationship between selective serotonin reuptake inhibitors and risk of dental implant failure. J Prosthodont. 2019;28(3):252–257. PubMed CrossRef
- Corbella S, Alberti A, Calciolari E, et al. Medium-and long-term survival rates of implant-supported single and partial restorations at a maximum follow-up of 12 years: a retrospective study. Int J Prosthodont (IJP). 2021;34(2):183–191. PubMed CrossRef
- Wu X, Al-Abedalla K, Rastikerdar E, et al. Selective serotonin reuptake inhibitors and the risk of osseointegrated implant failure: a cohort study. J Dent Res. 2014;93(11):1054–1061. PubMed CrossRef
- Jung RE, Al-Nawas B, Araujo M, et al. Group 1 ITI Consensus Report: the influence of implant length and design and medications on clinical and patient-reported outcomes. Clin Oral Implants Res. 2018;29(Suppl 16):69–77. PubMed CrossRef
- Wu X, Al-Abedalla K, Abi-Nader S, et al. Proton pump inhibitors and the risk of osseointegrated dental implant failure: a cohort study. Clin Implant Dent Relat Res. 2017;19(2):222–232. PubMed CrossRef
- Wadhwa R, Kumar M, Talegaonkar S, et al. Serotonin reuptake inhibitors and bone health: a review of clinical studies and plausible mechanisms. Osteoporos Sarcopenia. 2017;3(2):75–81. PubMed CrossRef
- Zhou C, Fang L, Chen Y, et al. Effect of selective serotonin reuptake inhibitors on bone mineral density: a systematic review and meta-analysis. Osteoporos Int. 2018;29(6):1243–1251. PubMed CrossRef
- Jones JS, Kimata R, Almeida OP, et al. Risk of fractures in stroke patients treated with a selective serotonin reuptake inhibitor: a systematic review and meta-analysis. Stroke. 2021;52(9):2802–2808. PubMed CrossRef
- Alsugeir D, John M, Tillyer E, et al. Antidepressant medications in women aged 40 and older and the risk of fragility fractures: a systematic literature review and meta-analysis. Expert Opin Pharmacother. 2024;25(14):1961–1970. PubMed CrossRef
- Kumar M, Bajpai R, Shaik AR, et al. Alliance between selective serotonin reuptake inhibitors and fracture risk: an updated systematic review and meta-analysis. Eur J Clin Pharmacol. 2020;76(10):1373–1392. PubMed CrossRef
- Andrade C. Survival analysis, Kaplan-Meier curves, and Cox regression: basic concepts. Indian J Psychol Med. 2023;45(4):434–435. PubMed CrossRef
- Andrade C. The E-value in regression: a useful, simple, easily understood, and easily applied statistic. J Clin Psychiatry. 2026;87(1):26f16324. PubMed CrossRef
- Lin L, Ren Y, Wang X, et al. Effects of bisphosphonates and denosumab on dental implants: a systematic review with meta-analysis. Oral Dis. 2025;31(10):2835–2847. PubMed CrossRef
- Pishan B, Andrukhov O, Rausch-Fan X. Dental implant failure in post-menopausal women on oral bisphosphonates: a systematic review and meta-analysis. J Oral Implantol. 2024;50(3):288–295. PubMed CrossRef
- Andrade C. Antidepressant drugs and the risk of hip fracture in the elderly: is there more to it than confounding by indication?. J Clin Psychiatry. 2019;80(4):19f12999. PubMed CrossRef
This PDF is free for all visitors!