Abstract
Proton pump inhibitors (PPIs) are the most prescribed gastric acid suppressant drugs; the category includes omeprazole, esomeprazole, lansoprazole, dexlansoprazole, pantoprazole, and rabeprazole. In 2015, a study suggested that PPI use was associated with an increased risk of dementia. An early meta-analysis confirmed this concern, but the findings were inconsistent in subsequent meta-analyses. Also problematic is that these meta-analyses used questionable approaches, and their findings were characterized by very high heterogeneity. Notably, the high heterogeneity appeared to be driven by large studies with widely different outcomes. Nonetheless, one finding stands out in the body of research examined: older subjects who initiated and continued PPIs (implying chronic use) were at a significantly increased risk of dementia and mild cognitive impairment. Although there are causal and non-causal pathways that associate PPI use with dementia, for reasons that are explained in this article, a cause-effect relationship cannot at present be presumed; so, PPI use is best considered to be a marker of future dementia risk. However, because chronic use of PPIs has been associated with many adverse medical outcomes (eg, disturbances of the gut microbiome, orthopedic complications), and because some PPIs are associated with pharmacokinetic drug interactions (mainly inhibition of CYP2C19), it would be wise to limit the use of PPIs to the shortest duration necessary and to deprescribe PPIs when there does not appear to be need for their continuation.
J Clin Psychiatry 2026;87(2):26f16420
Author affiliations are listed at the end of this article.
The most commonly prescribed categories of gastric acid suppressant drugs are the proton pump inhibitors (PPIs) and the histamine H2 receptor antagonists (H2RAs). The PPIs have a stronger inhibitory effect on gastric acid secretion and a longer duration of action and are therefore widely preferred over the H2RAs in clinical practice.1,2
Proton Pump Inhibitors
The first PPI released was omeprazole, which received US Food and Drug Administration marketing approval in 1989.3 Other PPIs followed, including esomeprazole, lansoprazole, dexlansoprazole, pantoprazole, and rabeprazole. The most important difference among these PPIs is perhaps pharmacokinetic; omeprazole is most likely to cause metabolic drug interactions (CYP2C19 and CYP3A4 inhibition), pantoprazole is least likely to cause metabolic drug interactions, and rabeprazole is least likely to be affected by metabolic drug interactions.4
The PPIs are used for a variety of indications, including treatment of acid peptic disease and eradication of Helicobacter pylori infection, treatment of gastroesophageal reflux disease (GERD), and prevention of acid peptic disease associated with use of nonsteroidal anti-inflammatory drugs, glucocorticoids, and others.
Proton Pump Inhibitors and Psychiatry
There are many reasons why PPIs are of actual or potential relevance in psychiatry. For example, depression and ischemic heart disease (IHD) commonly coexist,5 and patients with IHD often require treatment with aspirin and clopidogrel. Both these drugs, as well as selective serotonin reuptake inhibitors (SSRIs) that are used to treat depression, increase the risk of gastrointestinal bleeding; PPIs reduce the bleeding risk. Of additional interest, the SSRIs not only treat the depression associated with IHD but also reduce cardiovascular risks.6–8
Major mental illnesses, and the medications used in their treatment, are commonly associated with weight gain, and obesity is associated with an increased risk of GERD and the complications thereof9; patients with mental health conditions who are overweight or obese and have GERD are likely to receive a PPI. GERD is common during pregnancy, and PPIs are used to treat GERD10; there is concern that the use of PPIs during pregnancy may increase the risk of seizure disorder11 or affect neurodevelopment among exposed offspring.12 The use of PPI can adversely change the gut microbiome13,14; disturbances of the gut-brain axis may adversely affect mental health.15
Dementia is the acquired global impairment of intelligence, memory, and personality. Dementia compromises work ability, activities of daily living, and quality of life; it burdens caregivers; and because of its high prevalence among older subjects, it is a public health burden, as well. During the last decade, concern has arisen that PPI use may be associated with an increased risk of dementia. This concern is examined in the present article.
PPIs and Dementia: Possible Explanations for an Association
As explained in the previous section, PPIs may be prescribed for depression that is treated with SSRIs, IHD that is treated with aspirin and clopidogrel, and obesity with GERD. Depression, IHD, and obesity are all risk factors for dementia.16–19 PPIs may thus be associated with dementia through non-causal pathways.
Long-term use of PPIs may result in micronutrient deficiency, such as of vitamin B12, iron, and magnesium, all of which have roles to play in brain metabolism. PPIs may alter the gut microbiome and disturb the gut-brain axis, affecting brain functioning. PPIs may also increase the synthesis of amyloid and decrease its breakdown.20 PPIs may thus be associated with dementia through these hypothetical causal pathways.
PPIs and Dementia: Origins of the Concern
An early study of the clinical correlates of PPI use in residents of nursing homes found that PPIs were associated with a reduced risk of dementia (odds ratio [OR], 0.67; 95% CI, 0.59–0.76).21 However, this was a cross-sectional study, so causal effects cannot be postulated, and 29 variables were examined for strength of association with PPIs in an exploratory analysis, so a false positive statistical error cannot be ruled out.
The first study that credibly associated PPIs with an increased risk of dementia was probably published in 2015. The authors22 studied 3,327 community-dwelling subjects aged 75 years and older, drawn from the German Study on Aging, Cognition, and Dementia in Primary Care Patients. These subjects were followed for up to 6 years. In a time-varying adjusted Cox regression, PPI use was associated with an increased risk of Alzheimer’s disease (hazard ratio [HR], 1.44; 95% CI, 1.01–2.06) as well as an increased risk of any dementia (HR, 1.38; 95% CI, 1.04–1.83).
Many studies were subsequently performed and were pooled in meta-analyses. These are considered in the next sections.
PPIs and Dementia: Early Meta-Analyses
Several meta-analyses have examined the association between PPI use and dementia. These have differed in approach to study selection and in methods of data analysis. Three representative meta-analyses are summarized.
Five years after the appearance of the first report,22 a systematic review and meta-analysis (SRMA) of 6 cohort studies (pooled N=166,146) found that PPIs were associated with an increased risk of dementia (HR, 1.29, 95% CI, 1.12–1.49).23 However, one study in this meta-analysis based dementia diagnosis on cognitive tests and not on clinical diagnostic assessment.
In 2022, Wang et al24 described an SRMA of 17 studies (pooled N=1,251,562). They found that PPIs were not associated with an increased risk of dementia (HR, 0.98; 95% CI, 0.85–1.13; I 2, 99%; 14 studies; N, 1,082,875); H2RAs were not associated with increased risk, either (HR, 1.20; 95% CI, 0.98–1.47; I 2, 86%; 7 studies; N, 168,687). The source of the high heterogeneity remained undetected in subgroup analyses. Of serious concern, this meta-analysis indiscriminately pooled data from cohort, case-control, cross-sectional, and randomized controlled studies, presenting an HR as the estimate.
In 2023, Ahn et al25 described a focused SRMA of adjusted estimates from 9 prospective observational studies (pooled N=3,302,778; subjects with dementia, N =204,108). The authors used statistical methods to convert ORs and HRs for a common outcome to risk ratios (RRs). In these 9 studies, the RR for the association between PPIs and dementia just escaped statistical significance (RR, 1.16; 95% CI, 1.00–1.35; I 2, 99%). In subgroup analyses, only studies with lower risk of bias and studies with <10,000 dementia events were associated with negligible heterogeneity; notably, and unexpectedly, the large studies were dissimilar rather than similar in their point estimates. When only Alzheimer’s disease was examined as the outcome, the risk remained nonsignificant (RR, 1.15; 95% CI, 0.89–1.50; I 2, 97%; 5 studies). H2RAs were also not associated with risk of dementia (RR, 1.03; 95% CI, 0.66–1.62; I 2, 72%; 3 studies).
PPIs and Dementia: Recent Meta-Analysis
The most recent meta-analysis is that by Peng et al.26 These authors presented an updated SRMA of 18 studies (pooled N =6,325,898); the association between PPIs and dementia was not statistically significant (RR, 1.14; 95% CI, 0.98–1.33; I 2, 99%). The association between PPIs and Alzheimer’s disease was also not statistically significant (RR, 1.03; 95% CI, 0.92–1.16; I 2, 95%; 9 studies). The source of high heterogeneity could not be identified in subgroup analyses.
A limitation of this meta-analysis26 is that the authors pooled estimates from cohort studies, case-control studies, and randomized controlled studies. They stated that they “carefully handled” HRs, ORs, RRs, or incidence rate ratios (IRRs) to “avoid inappropriate pooling.” However, they used a “rare-outcome assumption,” and dementia is not a rare outcome in elderly populations. In any case, risk estimates (HRs, ORs, RRs, and IRRs) have different meanings and are interpreted differently in studies of different designs, and so pooling estimates from different study designs is questionable. This is especially so for outcomes that are not rare.
PPIs and Dementia: The “Starting and Adhering” Effect
Huang et al27 used trajectory modeling to identify short-term (n=7,406), intermittent (n=1,528), and long-term (n=1,599) PPI users across a 3-year period. They examined the risk of dementia in intermittent and long-term users, relative to short-term users, across a 5-year follow-up. They found that neither intermittent PPI use (HR, 0.91; 95% CI, 0.76–1.09) nor long-term PPI use (HR, 0.99; 95% CI, 0.93–1.17) was associated with risk of dementia. This study had not been included in any of the meta-analyses summarized in earlier sections of this article.
In contrast with the study by Huang et al,27 in the meta-analysis by Ahn et al,25 discussed earlier, starting and adhering to PPIs was associated with an increased risk of dementia (RR, 1.38; 95% CI, 1.20–1.58; 5 studies), whereas baseline assignment alone was not associated with increased risk (RR, 0.97; 95% CI, 0.89–1.05; 4 studies). The meta-analysis by Peng et al26 also found increased risk associated with starting and adhering to treatment (RR, 1.26; 95% CI, 0.98–1.62; 11 studies) but not with baseline assignment (RR, 0.99; 95% CI, 0.89–1.10; 7 studies). It is possible that the negative finding in the Huang et al27 study arose from insufficient separation in PPI exposure across groups.
PPIs and Dementia: The German Study28
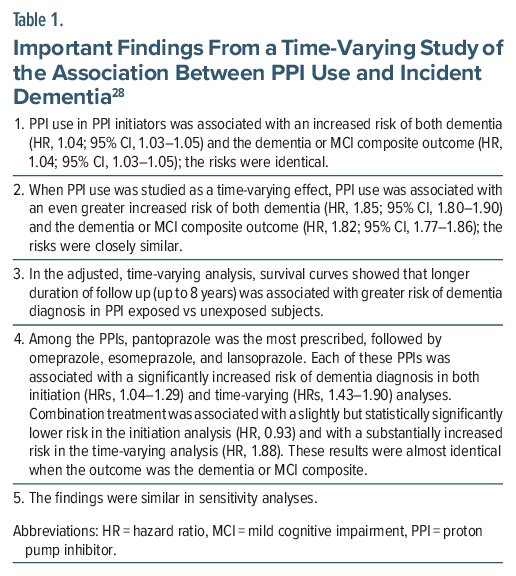
In another study not included in the meta-analyses, Ahn et al28 used data of subjects aged >40 years, drawn from the Association of Statutory Health Insurance Physicians in Bavaria database for the period 2009–2018. The sample comprised PPI initiators (n =2,886,733) and an equal number of non-initiators, matched with initiators using inverse probability of treatment weighting. The median age of the sample was 58 years. The sample was 56% female.
PPI initiators and non-initiators were followed for a median of 5.4 and 5.8 years, respectively. During follow-up (but after a 1-year lag period), dementia was diagnosed in 105,220 (3.6%) vs 74,697 (2.6%) of PPI initiators vs non-initiators, respectively. PPI initiation was studied as a time-varying risk factor after adjustment for important covariates and confounds such as age, sex, obesity, diabetes, hypertension, cardiovascular and cerebrovascular diseases, respiratory disease, cancer, depression, psychosis, other disorders associated with dementia, and a range of medication categories.
Important findings from the study are presented in Table 1. In summary, in both PPI initiation analyses and PPI time-varying analyses, PPIs were associated with an increased risk of dementia or mild cognitive impairment diagnoses. Whereas the risks were very low in the initiation analyses, they were high in the time-varying analyses, which could be expected to provide more trustworthy estimates. Importantly, this exposure-related increase in risk grew stronger as follow-up duration increased.
PPIs and Dementia: Other Studies
One more study that was not included in the meta-analysis is briefly examined. Zhang et al29 sampled 501,002 subjects from the UK Biobank for the period 2006–2010, followed up to 2018. The age of the subjects ranged from 40 to 70 (mean, 57) years. The sample was 54% female. The median duration of follow-up was 9.0 years. After adjusting for confounding variables, PPI use at baseline (in 10.7% of the sample) was associated with an increased risk of a new diagnosis of all-cause dementia (HR, 1.20; 95% CI, 1.07–1.35), as well as of Alzheimer’s disease (HR, 1.23; 95% CI, 1.02–1.49) and vascular dementia (HR, 1.32; 95% CI, 1.05–1.67). The cumulative risk of a dementia diagnosis in PPI users increased disproportionately (relative to non-users) with longer duration of follow-up. The findings were closely similar in a propensity score–matched subsample.
In exploratory subgroup analyses, the PPI-associated risk of all-cause dementia was significantly elevated in women but not in men, and in those aged 65 and older but not in those who were <65 years old. However, surprisingly, the risks were significantly elevated in those without obesity, in never smokers, in those who had not experienced stroke, and in those who were not depressed; the risks were not elevated in those who did have these risk factors for dementia. These findings suggest that PPIs elevate the risk, but not in those who are already at elevated risk.
Nonpsychiatric Risks Associated With Long-Term PPI Use
Long-term PPI use has been associated with many other risks.20 For example, the chronically decreased gastric acidity could compromise the absorption of micronutrients such as vitamin B12, iron, and magnesium.20 No clinical significance of these effects has been found to date.
The chronic gastric hypoacidity could alter the stomach and intestinal microbiome. Small intestinal bacterial overgrowth and Clostridioides difficile infections are possible outcomes.20 A systematic review and qualitative synthesis endorsed the possibility of small intestinal bacterial overgrowth; however, a quantitative synthesis (meta-analysis) of 8 randomized controlled trials (RCTs) found no association of PPIs with Clostridium difficile relative to either non-users or to users of other acid suppressant drugs.30
The PPI-induced chronic gastric hypoacidity could trigger hypergastrinemia and hyperplasia of enterochromaffin cells, possibly increasing the risk of gastric cancer.20 Whereas a meta-analysis suggested increased risk,31 a more recent, large, influential study identified sources of bias and found the association between PPI use and gastric cancer to be close to null.32
PPI use has been associated with reduced absorption of calcium and with an increased risk of bone fracture.20 More specifically, PPI use has been associated with bone non-union and non-fusion after orthopedic surgery,33,34 and with an increased risk of fracture, including fragility fracture, in children, adults, postmenopausal women, and elderly samples.35–38
PPIs have been suggested to increase the risk of acute kidney injury39; however, the quality of the evidence has been questioned.40 PPIs, however, may worsen renal and survival outcomes in patients receiving immune checkpoint inhibitors.41,42
Some PPIs may cause pharmacokinetic drug interactions. Omeprazole, esomeprazole, and lansoprazole inhibit CYP2C19, and omeprazole may inhibit CYP3A4, as well. The most widely cited drug interaction here is that related to the prevention of activation of clopidogrel (clopidogrel is a prodrug which is activated predominantly by CYP2C19). Whereas the clinical significance of this interaction has been questioned,43 it would be prudent to err on the side of caution and prefer pantoprazole in patients receiving clopidogrel.
Finally, PPIs have been associated with adverse cardiovascular outcomes in observational studies but not in RCTs.44
Take-Home Message
About 20 studies have examined the association between PPI use and new onset dementia. Most of these studies examined older subjects (e.g. aged 60 years and older) and followed subjects for 5-10 years.These studies were pooled in methodologically problematic meta-analyses, and the results were characterized by very high statistical heterogeneity and inconsistent conclusions. One finding, however, does seem salient: older subjects who initiate and continue PPIs (implying chronic use) are at a significantly increased risk of dementia and MCI.
One concern in postulating a cause-effect relationship between PPI use and dementia is that the mechanisms suggested in an early section of this article seem speculative. Another concern is that the relationship, detected in observational studies, may merely reflect residual confounding and longer exposure to confounds; more specifically, chronic confounds that are risk factors for dementia.
These reservations notwithstanding, given that many medical conditions have also been associated with long-term use of PPIs, it would be prudent to limit the use of PPIs to the shortest duration necessary, and to deprescribe PPIs when there does not appear to be need for their continuation.
Article Information
Published Online: April 13, 2026. https://doi.org/10.4088/JCP.26f16420
© 2026 Physicians Postgraduate Press, Inc.
To Cite: Andrade C. Proton pump inhibitors and the risk of dementia. J Clin Psychiatry 2026;87(2):26f16420.
Author Affiliations: Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India; Department of Psychiatry, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
Corresponding Author: Chittaranjan Andrade, MD, Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore 560029, India ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
 Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India. Please contact Chittaranjan Andrade, MD, at Psychiatrist.com/contact/andrade.
References (44)

- Richardson P, Hawkey CJ, Stack WA. Proton pump inhibitors. Pharmacology and rationale for use in gastrointestinal disorders. Drugs. 1998;56(3):307–335. PubMed CrossRef
- Brett S. Science review: the use of proton pump inhibitors for gastric acid suppression in critical illness. Crit Care. 2005;9(1):45–50. PubMed CrossRef
- Vanderhoff BT, Tahboub RM. Proton pump inhibitors: an update. Am Fam Physician. 2002;66(2):273–280. PubMed
- Tan CM, Juurlink DN. Navigating drug interactions with proton pump inhibitors. JAMA Netw Open. 2024;7(7):e2419818. PubMed CrossRef
- Glassman AH, Shapiro PA. Depression and the course of coronary artery disease. Am J Psychiatry. 1998;155(1):4–11. PubMed CrossRef
- Andrade C, Sandarsh S, Chethan KB, et al. Serotonin reuptake inhibitor antidepressants and abnormal bleeding: a review for clinicians and a reconsideration of mechanisms. J Clin Psychiatry. 2010;71(12):1565–1575. PubMed CrossRef
- Andrade C, Sharma E. Serotonin reuptake inhibitors and risk of abnormal bleeding. Psychiatr Clin North Am. 2016;39(3):413–426. PubMed CrossRef
- Sumner JA, Dennis PA, Alvarez CA, et al. Antidepressant medication prescription and incident cardiovascular disease in women veterans. J Clin Psychiatry. 2025;86(2):24m15647. PubMed CrossRef
- Xie M, Deng L, Fass R, et al. Obesity is associated with higher prevalence of gastroesophageal reflux disease and reflux related complications: a global healthcare database study. Neurogastroenterol Motil. 2024;36(4):e14750. PubMed CrossRef
- Gerson LB. Treatment of gastroesophageal reflux disease during pregnancy. Gastroenterol Hepatol. 2012;8(11):763–764. PubMed
- Gudnadottir U, Wickström R, Gunnerbeck A, et al. Prenatal and early childhood exposure to antibiotics or gastric acid inhibitors and increased risk of epilepsy: a nationwide population-based study. Clin Pharmacol Ther. 2025;118(1):206–217. PubMed CrossRef
- Hong S, Lee S, Kim H, et al. Prenatal exposure to acid-suppressive medications and risk of neuropsychiatric disorders in children. JAMA. 2026;335(7):609–618. PubMed CrossRef
- Imhann F, Bonder MJ, Vich Vila A, et al. Proton pump inhibitors affect the gut microbiome. Gut. 2016;65(5):740–748. PubMed CrossRef
- Fossmark R, Olaisen M. Changes in the gastrointestinal microbiota induced by proton pump inhibitors—a review of findings from experimental trials. Microorganisms. 2024;12(6):1110. PubMed CrossRef
- Doenyas C, Clarke G, Cserjési R. Gut-brain axis and neuropsychiatric health: recent advances. Sci Rep. 2025;15(1):3415. PubMed CrossRef
- Elser H, Horváth-Puhó E, Gradus JL, et al. Association of early-middle-and late-life depression with incident dementia in a Danish cohort. JAMA Neurol. 2023;80(9):949–958. PubMed CrossRef
- Fernández Fernández R, Martín JI, Antón MAM. Depression as a risk factor for dementia: a meta-analysis. J Neuropsychiatry Clin Neurosci. 2024;36(2):101–109. PubMed CrossRef
- Imahori Y, Vetrano DL, Ljungman P, et al. Association of ischemic heart disease with long-term risk of cognitive decline and dementia: a cohort study. Alzheimers Dement. 2023;19(12):5541–5549. PubMed CrossRef
- Ma Y, Ajnakina O, Steptoe A, et al. Higher risk of dementia in English older individuals who are overweight or obese. Int J Epidemiol. 2020;49(4):1353–1365. PubMed CrossRef
- Chinzon D, Domingues G, Tosetto N, et al. Safety of long-term proton pump inhibitors: facts and myths. Arq Gastroenterol. 2022;59(2):219–225. PubMed CrossRef
- de Souto Barreto P, Lapeyre-Mestre M, Mathieu C, et al. Prevalence and associations of the use of proton-pump inhibitors in nursing homes: a cross-sectional study. J Am Med Dir Assoc. 2013;14(4):265–269. PubMed CrossRef
- Haenisch B, von Holt K, Wiese B, et al. Risk of dementia in elderly patients with the use of proton pump inhibitors. Eur Arch Psychiatry Clin Neurosci. 2015;265(5):419–428. PubMed CrossRef
- Zhang Y, Liang M, Sun C, et al. Proton pump inhibitors use and dementia risk: a meta-analysis of cohort studies. Eur J Clin Pharmacol. 2020;76(2):139–147. PubMed CrossRef
- Wang H, Tian L, Yan X. No association between acid suppressant use and risk of dementia: an updated meta-analysis. Eur J Clin Pharmacol. 2022;78(3):375–382. PubMed CrossRef
- Ahn N, Nolde M, Krause E, et al. Do proton pump inhibitors increase the risk of dementia? A systematic review, meta-analysis and bias analysis. Br J Clin Pharmacol. 2023;89(2):602–616. PubMed CrossRef
- Peng TR, Lin HH, Yang LJ, et al. Inconsistency in the association between proton pump inhibitor use and dementia risk: an updated meta-analysis. Brain Sci. 2026;16(2):159. PubMed CrossRef
- Huang ST, Tseng LY, Chen LK, et al. Does long-term proton pump inhibitor use increase risk of dementia? Not really! results of the group-based trajectory analysis. Clin Pharmacol Ther. 2019;106(3):616–622. PubMed CrossRef
- Ahn N, Wawro N, Baumeister SE, et al. Time-varying use of proton pump inhibitors and cognitive impairment and dementia: a real-world analysis from Germany. Drugs Aging. 2023;40(7):653–663. PubMed CrossRef
- Zhang P, Li Z, Chen P, et al. Regular proton pump inhibitor use and incident dementia: population-based cohort study. BMC Med. 2022;20(1):271. PubMed CrossRef
- Floria DE, Obeidat M, Váncsa S, et al. Proton pump inhibitors are not associated with an increased risk of Clostridioides difficile infection: a systematic review and meta-analysis of randomized controlled trials. Gut Microbes. 2025;17(1):2562341. PubMed CrossRef
- Zhang H, Meng X, Gou D, et al. A meta-analysis of the effects of proton pump inhibitors on the risk of gastric cancer. Medicine (Baltim). 2025;104(28):e43053. PubMed CrossRef
- Duru O, Santoni G, Holmberg D, et al. Long term use of proton pump inhibitors and risk of stomach cancer: population based case-control study in five Nordic countries. BMJ. 2026;392:e086384. PubMed CrossRef
- Romoff M, Kim MS, Spitzer C, et al. Proton pump inhibitors are associated with increased risk of site-specific nonunion after open reduction internal fixation. J Orthop Trauma. 2025;9(4):203–211. PubMed CrossRef
- Chang Y, Lin YS, Huang CY, et al. The impact of proton pump inhibitor use on fusion rates following single-level lumbar spinal fusion surgery. Eur Spine J. 2025;34(9):4083–4087. PubMed CrossRef
- Poly TN, Islam MM, Yang HC, et al. Proton pump inhibitors and risk of hip fracture: a meta-analysis of observational studies. Osteoporos Int. 2019;30(1):103–114. PubMed CrossRef
- Liu J, Li X, Fan L, et al. Proton pump inhibitors therapy and risk of bone diseases: an update meta-analysis. Life Sci. 2019;218:213–223. PubMed CrossRef
- Yang J, Zhou TJ, Yang J, et al. Use of acid-suppressive drugs and risk of fracture in children and young adults: a meta-analysis of observational studies. Eur J Clin Pharmacol. 2022;78(3):365–373. PubMed CrossRef
- Robert V, Papailhau C, Lesclide E, et al. Proton pump inhibitors and risk of fracture in older adults: a systematic review and meta-analysis. Geriatr Nurs. 2025;66(Pt A):103596. PubMed CrossRef
- Yang Y, George KC, Shang WF, et al. Proton-pump inhibitors use, and risk of acute kidney injury: a meta-analysis of observational studies. Drug Des Devel Ther. 2017;11:1291–1299. PubMed CrossRef
- Weir MR. Proton pump inhibitors and kidney disease: fact or fiction? Am J Nephrol. 2024;55(4):499–508. PubMed CrossRef
- Okamoto K, Saito Y, Yamaguchi A, et al. Acid suppressants reduce the therapeutic effect of immune checkpoint inhibitors and increase the risk of acute kidney injury: a meta-analysis. Int J Clin Oncol. 2023;28(10):1343–1353. PubMed CrossRef
- Mohan A, Krisanapan P, Tangpanithandee S, et al. Association of proton pump inhibitor use and immune checkpoint inhibitor-mediated acute kidney injury: a meta-analysis and a review of related outcomes. Am J Nephrol. 2024;55(4):439–449. PubMed CrossRef
- Wołowiec Ł, Osiak-Gwiazdowska J, Jaśniak A, et al. Pharmacodynamics, pharmacokinetics, interactions with other drugs, toxicity and clinical effectiveness of proton pump inhibitors. Front Pharmacol. 2025;16:1507812. PubMed CrossRef
- Padhi BK, Khatib MN, Zahiruddin QS, et al. Adverse cardiovascular outcomes associated with proton pump inhibitor use after percutaneous coronary intervention: a systematic review and meta-analysis. BMC Cardiovasc Disord. 2024;24(1):372. PubMed CrossRef
This PDF is free for all visitors!




