Background: Nonadherence to medication compromises the effectiveness of psychiatric treatments in patients with serious mental illness (SMI). A newly developed digital medicine system (DMS) offers an opportunity to objectively assess and report patient medication adherence. DMS includes a wearable sensor that receives a data signal from a medication tablet with an embedded ingestible sensor after ingestion of the medication and transmits that data to the patient’s mobile device to display health care information for the patient and treatment team.
Methods/Results: Development of a DMS requires a program that investigates safety, tolerability, and usability of the system in patients with SMI. It necessitates rapid design adaptation of the individual components and the integrated system and human factors studies with the intended users. This article describes the program’s methodology and shows results from 3 early studies, conducted in 2013 and 2014, to illustrate diversity of the programs’ methodology. First, a standard 28-day study showed minimal skin irritation and demonstrated acceptable wearability of the wearable sensor. Second, a 16-week study provided usability feedback from patients with SMI and caregivers to improve the mobile application. Third, end-to-end bench-level integrated system testing led to multiple substudies of a master protocol (ClinicalTrials.gov identifier: NCT02091882) to investigate various aspects of the system (eg, ingestible sensor detection and latency).
Conclusions: To develop a DMS in psychiatry, the system’s multiple components must be considered simultaneously using various methodologies. A focus on usability, along with agile evaluation and feedback across studies, provides an optimal strategy for ensuring patient acceptance and successful regulatory review.
Optimization of a Digital Medicine System in Psychiatry
ABSTRACT
Background: Nonadherence to medication compromises the effectiveness of psychiatric treatments in patients with serious mental illness (SMI). A newly developed digital medicine system (DMS) offers an opportunity to objectively assess and report patient medication adherence. DMS includes a wearable sensor that receives a data signal from a medication tablet with an embedded ingestible sensor after ingestion of the medication and transmits that data to the patient’s mobile device to display health care information for the patient and treatment team.
Methods/Results: Development of a DMS requires a program that investigates safety, tolerability, and usability of the system in patients with SMI. It necessitates rapid design adaptation of the individual components and the integrated system and human factors studies with the intended users. This article describes the program’s methodology and shows results from 3 early studies, conducted in 2013 and 2014, to illustrate diversity of the programs’ methodology. First, a standard 28-day study showed minimal skin irritation and demonstrated acceptable wearability of the wearable sensor. Second, a 16-week study provided usability feedback from patients with SMI and caregivers to improve the mobile application. Third, end-to-end bench-level integrated system testing led to multiple substudies of a master protocol (ClinicalTrials.gov identifier: NCT02091882) to investigate various aspects of the system (eg, ingestible sensor detection and latency).
Conclusions: To develop a DMS in psychiatry, the system’s multiple components must be considered simultaneously using various methodologies. A focus on usability, along with agile evaluation and feedback across studies, provides an optimal strategy for ensuring patient acceptance and successful regulatory review.
J Clin Psychiatry
dx.doi.org/10.4088/JCP.16m10693
© Copyright 2016 Physicians Postgraduate Press, Inc.
aOtsuka Pharmaceutical Development & Commercialization, Inc, Princeton, New Jersey
bODH, Inc, Princeton, New Jersey
*Corresponding author: Shashank Rohatagi, PhD, MBA, Otsuka Pharmaceutical Development & Commercialization, Inc, 508 Carnegie Center Blvd, Princeton, NJ 08540 ([email protected]).
Serious mental illness (SMI) is one of the leading causes of long-term disability worldwide. Major depressive disorder (MDD), schizophrenia, and bipolar disorder were ranked second, 11th, and 17th, respectively, on the list of global causes of long-term disability surveyed in 188 countries by the Global Burden of Disease Study 2013.1 SMI affects a large proportion of the US population; in 2012, the estimated prevalence of mental illness and SMI among adults was 18.5% and 4.2%, respectively, based on the National Survey on Drug Use and Health.2 Pharmacologic treatment interventions reduce the severity of SMI and improve patient outcomes. For example, meta-analyses of results from 65 and 72 placebo-controlled clinical trials in schizophrenia and MDD, respectively, showed that treatment with antipsychotics or antidepressants significantly reduces rates of patient relapse.3,4 However, medication is effective only when taken as prescribed, and nonadherence to treatment of SMI is often associated with suboptimal response as indicated by psychiatric hospitalization, arrests, violence, increased risk of suicide attempt, and poor occupational and social functioning.5–7 It is estimated that 40%–50% of patients with SMI are nonadherent to medication,8,9 and the rates further increase with longer observation time. For example, in a large, 4-year, cross-sectional study, 36% of patients with schizophrenia were found to be poorly adherent in each year, but 61% had adherence problems at some point during the study period.10 Assessment of nonadherence often relies on subjective patient self-report or clinician assessment.11 Studies comparing self-report or clinician judgment to more objective measures of adherence indicate that the former methods lead to overestimating patient adherence by health care providers.12 Numerous modalities currently available for direct or objective assessment of adherence, including pill counts, Medication Event Monitoring System (MEMS) bottle caps, pharmacy refill records, and biological assays from bodily fluids, have limitations, and none provide an actual measure of medication ingestion.13 Therefore, the ability to precisely and objectively assess medication adherence in patients with SMI remains a significant unmet need.
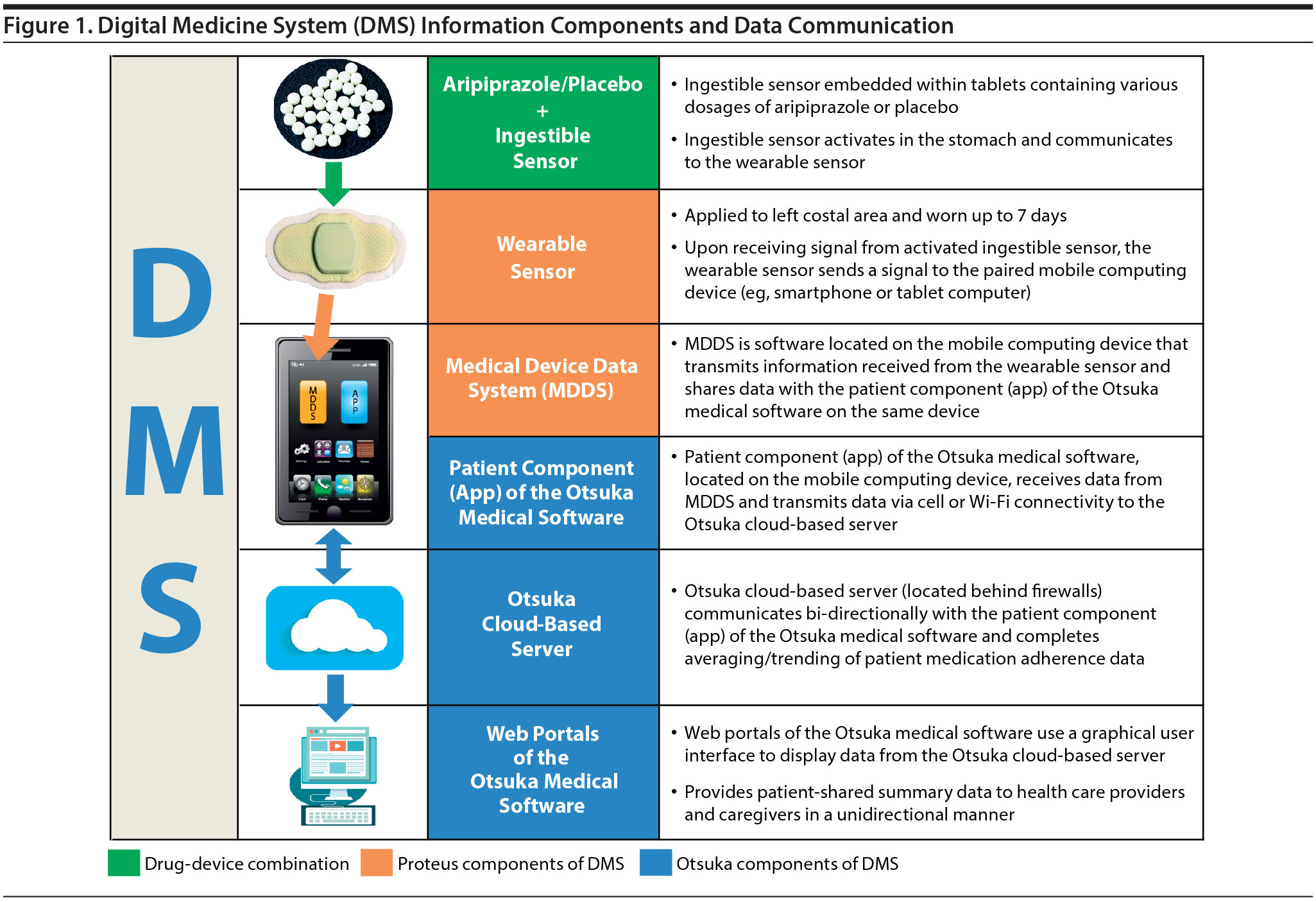
A newly developed digital medicine system (DMS) offers an innovative opportunity to objectively measure and report actual patient medication adherence. The DMS includes a wearable sensor that receives a data signal from a medication tablet with an embedded ingestible sensor activated in the stomach following medication ingestion. The design and performance of the ingestible sensor have been previously reviewed.14 Results from a trial that assessed medication adherence in patients with bipolar I disorder and schizophrenia using a prototype of a DMS were published in 2013 and demonstrated utility and good tolerability of the system for patients with psychiatric conditions.15 DMS is now being developed as a drug-device combination to assess adherence to aripiprazole, an atypical antipsychotic indicated for the treatment of schizophrenia, bipolar disorder, and MDD.16 The DMS enables confirmation of ingestion and electronic feedback to the patient and health care provider (HCP), as well as the elected caregiver, family member, or friend. The system is an integrated product with 3 distinct components: ingestible sensor embedded in a medication tablet, wearable sensor, and mobile- and cloud-based software (Figure 1). The development of an integrated technology that comprises pharmaceutical, medical device, and mobile application components and has the added complexity of involving multiple participants (ie, patient, HCP, caregiver) necessitates a number of empirical considerations and requires an evidence-based program that differs from the traditional development of a pharmaceutical agent.
A series of studies is being conducted to (1) identify the safety, tolerability, and usability of each individual component of the system; (2) evaluate safety and tolerability of the whole system; (3) determine human factors (HF) usability; and (4) assess integration of the individual components into the system and information flow. This integrated approach involves a combination of novel designs of clinical studies that adhere to good clinical practice and iterative usability testing using HF studies. Usability testing refers to the user experience of interacting with the system and is key to the development process of mobile applications.17 This method reveals design deficiencies and ensures the application is understandable, usable, and attractive for the targeted end users.18 The trials included in the DMS program are designed to accommodate subjective feedback from patients, caregivers, and HCPs in an iterative process that aims at improving functionality of individual components and also user experience with the overall system. This article outlines the overall DMS development process and then focuses on 3 individual studies as examples of early steps in the development program.
METHODS AND RESULTS
Development Process
The development of a DMS requires a program that investigates the safety, tolerability, and usability of the system in patients with SMI. The program necessitates conducting multiple independent studies that enable rapid refinement and adaptation both on the level of the individual components and as an integrated system. The studies used in the DMS development process are exploratory clinical trials and HF studies that allow DMS optimization and risk assessment. The goal of the clinical trials is to inform HF studies and provide product-related information. The goal of the HF studies is to assess the safe, effective, and correct use of DMS by the intended user for the intended uses. The stepwise process of deploying individual studies within the DMS development program is outlined in Table 1 and Figure 2. Dermal safety (study 316-13-205), iterative application development (study 316-13-204), and iterative detection of ingestion and latency (study 316-14-206a followed by 206b) represent areas investigated in the clinical trials that illustrate the diversity of approaches used during the DMS development.

Dermal Safety
The primary objective of the dermal safety study was to evaluate the wearable sensor for potential skin irritation when applied to normal skin and to determine the overall safety and tolerability of the sensor. The secondary objective was to evaluate adhesiveness of the wearable sensor. The study was conducted according to the US Food and Drug Administration (FDA) guidelines for industry on skin irritation testing.19 The study was approved by the institutional review board (Integreview), and the study participants provided written informed consent.
In this phase 1, open-label, 4-week trial, conducted from June 2013 to July 2013, 30 healthy volunteers were randomly assigned in a 1:1 ratio to receive the wearable sensor on either the right or left side of the body above the lower edge of the rib cage. A control comparator, a 2 × 2 cm Webril pad attached to a nonporous, plastic film adhesive bandage (3M Blenderm), was worn on the opposite side. The sensor and the comparator were worn continuously for 7 days with weekly replacement, for a total of 4 applications in a 28-day period. The demographics, baseline characteristics, and disposition of the study participants are shown in Table 2.
Of the 30 individuals randomized, 23 (76.7%) completed the study. Total cumulative and mean skin irritation scores were assessed for each participant using the modified Draize method.21 Pruritus was measured using the Visual Analog Scale that evaluates itch on a scale of 0 (no itch) to 100 mm (worst imaginable itch).22 Results of the trial showed that the wearable sensor caused little to no irritation (cumulative and mean skin irritation scores: 0–0.1) and mild increase in pruritus (mean change from baseline at all visits: 14.2–18.6 mm). The wearable sensor was well tolerated, with no adverse events reported during the trial. The participants wore the sensor for an average of 6 days per week, and the period of wearability increased over the course of the trial.
Iterative Application Development
The primary objective of this application development study was to obtain descriptive feedback from patients with bipolar I disorder or MDD and their caregivers about updates made iteratively to the Otsuka medical software mobile phone application used in an early prototype of the DMS. The secondary objective was to assess safety of the DMS components. An additional objective was to summarize patient adherence based on ingestible sensor detection reported by the DMS prototype.
The study was a 16-week, open-label, single-arm, clinical usability phase 4/exploratory observational trial conducted from August 2013 to February 2014 in 58 stable patients with a diagnosis of bipolar I disorder (n = 35) or MDD (n = 23) based on Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition (DSM-IV) criteria and 22 patient-designated caregivers. Written informed consent was obtained from the study participants, and the protocol was approved by the institutional review board (Copernicus Group). Patients took placebo embedded with the ingestible sensor in addition to their regular medication. All users were scheduled to provide regular feedback via in-person, one-on-one, biweekly interviews and computer-administered questionnaires on usability of the mobile and the web software. The feedback was used to continuously update versions of the application. The study design enabled an innovative, multistep iterative refinement of the DMS prototype functions. In addition, patients also regularly assessed ease of wear and the comfort level of the wearable sensor.
Of the 58 enrolled participants, 47 completed the study (Table 2). The feedback from study participants yielded positive results regarding usability and safety of the DMS prototype. By the end of the study, 83% of patients (48/58) felt very confident using the patient component of the Otsuka medical software, and 79% of patients (46/58) agreed that the wearable sensor is comfortable to wear by selecting a rating of ≥ 5 on a scale of 1 (strongly disagree) to 7 (strongly agree). At the end of the study, 60% of patients (18/30) were very or extremely satisfied with the system, and 74% of patients (22/30) indicated that they would likely use the DMS in the future by selecting a rating of ≥ 5 on a scale of 1 (extremely unlikely) to 7 (extremely likely). The study was a first controlled test of an early version of the patient smartphone application that guided a series of subsequent trials to further investigate and refine functionality and usability of the DMS.
Iterative Detection of Ingestion and Latency
The primary objective of the ingestion detection study was to measure the accuracy of ingestible sensor detection by the DMS using tablets containing either aripiprazole or placebo and to determine the latency period between tablet ingestion and detection by the wearable sensor for both types of the ingested tablets. The secondary objective was to evaluate safety of the DMS. The ingestible sensor is safe and has been cleared for use by the FDA.23
The study examining ingestion and latency was a 1-day, nonrandomized, prospective, single-site, phase 4 clinical trial with 30 healthy volunteers conducted from March 2014 to April 2014 as a substudy of the Otsuka Study of Marker Ingested to Trigger Event Recorder (OSMITTER; ClinicalTrials.gov identifier: NCT02091882) umbrella protocol. The protocol was approved by the institutional review board (Copernicus Group), and participants provided signed informed consent. This master protocol was designed to rapidly test the technical performance, safety, and user satisfaction of the DMS components with healthy volunteers who could theoretically enroll into 24 feasibility substudies over a 12-month period.
The participants ingested a tablet embedded with the ingestible sensor every 2 hours for a total of 4 ingestions and were administered a new wearable sensor at each time point. The tablet ingested at hour 0 contained 10 mg of aripiprazole, and the tablets ingested at hours 2, 4, and 6 contained placebo. In this trial, ingestible sensor detection by the wearable sensor was 98.3%. A subsequent substudy (316-14-206b, Figure 2) that used a slightly modified protocol and tested updated versions of the phone application and the wearable sensor showed an overall ingestion detection rate of 96.6%. Results of the modified substudy are reported in detail elsewhere.20 The mean times of latency between ingestible sensor ingestion and detection by the wearable sensor were 1.1 and 5.1 minutes for sensors embedded in the placebo and aripiprazole tablets, respectively. The most common trial medication-associated adverse event (AE) was nausea, which was reported in 5 patients (16.7%). No serious medication-associated or device-associated AEs were reported.
DISCUSSION
The widespread use of mobile technologies such as cellular phones and smartphones has led to the rapid development of numerous applications in support of health care and the emergence of digital health aimed to deliver actionable health care information to patients, practitioners, and researchers. Digital medicine is intended to monitor health status and improve health outcomes, a service that is particularly useful in mental health.24 A recent review of 46 studies reporting outcomes from digital health interventions in psychiatry found that emerging mobile technologies are highly feasible and acceptable for use among patients with SMI.25
Unfortunately, digital health technologies are often developed without adequate evaluation of their validity and effectiveness.26 A rigorous scientific approach to developing a new system based on formative and qualitative research with target users is time-consuming and often impractical to conduct in the field, considering the rapid evolution of technologies and their continuously changing role in daily life. Consequently, reports describing processes and outcomes from development of digital health technologies are scarce.27 Nevertheless, it is essential to ensure that the intended users can properly use the technology. Devices that fail to meet users’ behavioral and cognitive needs impose risks of adverse events resulting from user errors and increase frustration for the user. For example, designs used in common websites are poorly suited for patients with SMI whose neurocognitive deficits impose a barrier to effectively navigating and searching within standard websites.28 Therefore, interfaces intended for patients with SMI must be designed for, and have their usability tested in, the SMI patient population. Deployment of a user-centered program is particularly critical when deficits associated with SMI may compromise not only usability but also safety of the system. The process of development of the DMS included safety studies and extensive iterative HF studies directed at patients with SMI, their caregivers, and their health care providers. HF testing led to numerous modifications of the patient mobile application.
The 3 clinical trials outlined in this article were implemented early in the process of development of DMS and represent examples of different study designs: a traditional safety and tolerability study (dermal safety of the wearable sensor), an innovative formative usability study (iterative application development in patients with SMI), and a combined traditional and iterative study (detection of ingestion and latency in healthy volunteers). The results from these studies provided important feedback to the development team on early deficiencies in the design of individual components and led to multiple subsequent revisions in the patient mobile application, improvements in the wearable sensor, and simplifications in patient instructions for use. The early modifications, tested and further refined in subsequent clinical trials and HF studies, substantially improved the function and usability of the system.
The studies described here have some limitations. The dermal study and the study on detection of ingestion and latency were conducted in healthy volunteers. However, this was necessary to isolate the effects of disease symptoms from the ability to use the technology associated with the DMS. In addition, the studies were performed under conditions that sought to minimize influence of factors that might exist in a real world setting, such as interference from other mobile devices.
DMS has potential advantages over other measures of assessing medication adherence.13 Unlike adherence assessment interviews or questionnaires, DMS does not rely on HCP perception or patient self-reporting, but instead provides an objective assessment by directly measuring medication ingestion. An automated adherence report generated by the DMS may overcome the drawback of possible incongruity between the number of electronically recorded bottle openings and the number of times the medication is ingested when using MEMS as an objective method for assessing adherence. Additionally, unlike biologic measures, DMS does not require blood sampling to measure adherence. Finally, unlike pharmacy records, DMS does not rely on the assumption that fulfillment of medication prescription indicates medication ingestion. Monitoring of objective adherence data with the DMS is anticipated to increase compliance and thereby potentially improve treatment outcomes.
CONCLUSIONS
The DMS represents a novel drug-device combination, and its rigorous development in psychiatry requires simultaneous use of various methodologies such as safety and tolerability studies, end-to-end bench testing, and HF studies capable of assessing data from diverse sources (ingestible sensor, wearable sensor, mobile application, clinical and human factors) and formats (qualitative and quantitative). A user-centric focus on usability, along with agile evaluation and feedback across studies, provides an optimal strategy for ensuring adequate patient acceptance and successful regulatory meetings in the emerging era of digital medicine.
Submitted: January 21, 2016; accepted May 2, 2016.
Online first: August 2, 2016.
Drug names: aripiprazole (Abilify).
Potential conflicts of interest: Drs Rohatagi, Profit, Zhao, and Peters-Strickland are employees of Otsuka Pharmaceutical Development & Commercialization, Inc. Drs Hatch and Docherty are employees of ODH, Inc.
Funding/support: Supported by Otsuka Pharmaceutical Development & Commercialization, Inc.
Previous presentation: American Society of Clinical Psychopharmacology Annual Meeting, June 22–25, 2015, Miami, Florida; and American Psychiatric Association 168th Annual Meeting, May 16–20, 2015, Toronto, Ontario, Canada.
Role of the sponsor: The sponsor is fully responsible for design, conduct, and reporting of the study.
Acknowledgments: Editorial support for development of this manuscript was provided by C4 MedSolutions, LLC (Yardley, PA), a CHC Group company, and was funded by Otsuka Pharmaceutical Development & Commercialization, Inc.
REFERENCES
1. Global Burden of Disease Study 2013 Collaborators. Global, regional, and national incidence, prevalence, and years lived with disability for 301 acute and chronic diseases and injuries in 188 countries, 1990–2013: a systematic analysis for the Global Burden of Disease Study 2013. Lancet. 2015;386(9995):743–800. doi:10.1016/S0140-6736(15)60692-4 PubMed
2. Substance Abuse and Mental Health Services Administration. Results from the 2013 National Survey on Drug and Health: Mental Health Findings. NSDUH Series H-49, HHS Publication No (SMA) 14-4887. Rockville, MD: Substance Abuse and Mental Health Services Administration; 2014.
3. Leucht S, Tardy M, Komossa K, et al. Antipsychotic drugs versus placebo for relapse prevention in schizophrenia: a systematic review and meta-analysis. Lancet. 2012;379(9831):2063–2071. doi:10.1016/S0140-6736(12)60239-6 PubMed
4. Sim K, Lau WK, Sim J, et al. Prevention of relapse and recurrence in adults with major depressive disorder: systematic review and meta-analyses of controlled trials. Int J Neuropsychopharmacol. 2015;19(2):pyv076. doi:10.1093/ijnp/pyv076 PubMed
5. Ascher-Svanum H, Faries DE, Zhu B, et al. Medication adherence and long-term functional outcomes in the treatment of schizophrenia in usual care. J Clin Psychiatry. 2006;67(3):453–460. doi:10.4088/JCP.v67n0317 PubMed
6. Hong J, Reed C, Novick D, et al. Clinical and economic consequences of medication non-adherence in the treatment of patients with a manic/mixed episode of bipolar disorder: results from the European Mania in Bipolar Longitudinal Evaluation of Medication (EMBLEM) study. Psychiatry Res. 2011;190(1):110–114. doi:10.1016/j.psychres.2011.04.016 PubMed
7. Scott J, Pope M. Self-reported adherence to treatment with mood stabilizers, plasma levels, and psychiatric hospitalization. Am J Psychiatry. 2002;159(11):1927–1929. doi:10.1176/appi.ajp.159.11.1927 PubMed
8. Lacro JP, Dunn LB, Dolder CR, et al. Prevalence of and risk factors for medication nonadherence in patients with schizophrenia: a comprehensive review of recent literature. J Clin Psychiatry. 2002;63(10):892–909. doi:10.4088/JCP.v63n1007 PubMed
9. Sajatovic M, Valenstein M, Blow FC, et al. Treatment adherence with antipsychotic medications in bipolar disorder. Bipolar Disord. 2006;8(3):232–241. doi:10.1111/j.1399-5618.2006.00314.x PubMed
10. Valenstein M, Ganoczy D, McCarthy JF, et al. Antipsychotic adherence over time among patients receiving treatment for schizophrenia: a retrospective review. J Clin Psychiatry. 2006;67(10):1542–1550. doi:10.4088/JCP.v67n1008 PubMed
11. Velligan DI, Lam YW, Glahn DC, et al. Defining and assessing adherence to oral antipsychotics: a review of the literature. Schizophr Bull. 2006;32(4):724–742. doi:10.1093/schbul/sbj075 PubMed
12. Velligan DI, Wang M, Diamond P, et al. Relationships among subjective and objective measures of adherence to oral antipsychotic medications. Psychiatr Serv. 2007;58(9):1187–1192. doi:10.1176/ps.2007.58.9.1187 PubMed
13. Sajatovic M, Velligan DI, Weiden PJ, et al. Measurement of psychiatric treatment adherence. J Psychosom Res. 2010;69(6):591–599. doi:10.1016/j.jpsychores.2009.05.007 PubMed
14. Hafezi H, Robertson TL, Moon GD, et al. An ingestible sensor for measuring medication adherence. IEEE Trans Biomed Eng. 2015;62(1):99–109. doi:10.1109/TBME.2014.2341272 PubMed
15. Kane JM, Perlis RH, DiCarlo LA, et al. First experience with a wireless system incorporating physiologic assessments and direct confirmation of digital tablet ingestions in ambulatory patients with schizophrenia or bipolar disorder. J Clin Psychiatry. 2013;74(6):e533–e540. doi:10.4088/JCP.12m08222 PubMed
16. Abilify [package insert]. Tokyo, Japan: Otsuka Pharmaceutical Co, Ltd; 2014.
17. Bastien JM. Usability testing: a review of some methodological and technical aspects of the method. Int J Med Inform. 2010;79(4):e18–e23. doi:10.1016/j.ijmedinf.2008.12.004 PubMed
18. Mohr DC, Burns MN, Schueller SM, et al. Behavioral intervention technologies: evidence review and recommendations for future research in mental health. Gen Hosp Psychiatry. 2013;35(4):332–338. doi:10.1016/j.genhosppsych.2013.03.008 PubMed
19. Guidance for Industry (Draft): Skin Irritation and Sensitization Testing of Generic Transdermal Drug Products. US Food and Drug Administration Web site. http://www.fda.gov/ohrms/dockets/98fr/990236Gd.pdf. December 1999.
20. Profit D, Rohatagi S, Zhao C, et al. Developing a digital medicine system in psychiatry: ingestion detection rate and latency period [published online July 5, 2016]. J Clin Psychiatry. doi:10.4088/JCP.16m10643
21. Draize JH, Woodard G, Calvery HO. Methods for the study of irritation and toxicity of substances applied topically to the skin and mucous membranes. J Pharmacol Exp Ther. 1944;82:377–390.
22. Phan NQ, Blome C, Fritz F, et al. Assessment of pruritus intensity: prospective study on validity and reliability of the visual analogue scale, numerical rating scale and verbal rating scale in 471 patients with chronic pruritus. Acta Derm Venereol. 2012;92(5):502–507. doi:10.2340/00015555-1246 PubMed
23. 510(k) Premarket Notification K131009. US Food and Drug Administration Web site. http://www.accessdata.fda.gov/scripts/cdrh/cfdocs/cfpmn/pmn.cfm?ID=K131009. Updated May 7, 2013. Accessed November 6, 2015.
24. Harrison V, Proudfoot J, Wee PP, et al. Mobile mental health: review of the emerging field and proof of concept study. J Ment Health. 2011;20(6):509–524. doi:10.3109/09638237.2011.608746 PubMed
25. Naslund JA, Marsch LA, McHugo GJ, et al. Emerging mHealth and eHealth interventions for serious mental illness: a review of the literature. J Ment Health. 2015;24(5):321–332. doi:10.3109/09638237.2015.1019054 PubMed
26. Nilsen W, Kumar S, Shar A, et al. Advancing the science of mHealth. J Health Commun. 2012;17(suppl 1):5–10. doi:10.1080/10810730.2012.677394 PubMed
27. Whittaker R, Merry S, Dorey E, et al. A development and evaluation process for mHealth interventions: examples from New Zealand. J Health Commun. 2012;17(suppl 1):
11–21. doi:10.1080/10810730.2011.649103 PubMed
28. Rotondi AJ, Sinkule J, Haas GL, et al. Designing websites for persons with cognitive deficits: design and usability of a psychoeducational intervention for persons with severe mental illness. Psychol Serv. 2007;4(3):202–224. doi:10.1037/1541-1559.4.3.202 PubMed
This PDF is free for all visitors!





