Catatonia remains a subject of ongoing debate, whether it represents a purely motoric syndrome, a separate distinct neuropsychiatric entity, or a symptom cluster within broader psychiatric conditions, characterized by features such as stupor, mutism, and negativism. The pathophysiology remains poorly understood, but multiple neurotransmitter systems seem to be involved in catatonia, including γ-aminobutyric acid (GABA) and glutamate.1 First-line treatment is the GABAA agonist lorazepam, with response rates varying between 66% and 100%, and second-line treatment is electroconvulsive therapy (ECT).2 Patients nonresponsive to treatment remain challenging. Recent evidence suggests that N-methyl-D-aspartate (NMDA) receptor antagonists, such as (es)ketamine, may offer benefit. We conducted a systematic review to evaluate the efficacy and safety of (es)ketamine for catatonia.
Methods
We searched 14 databases (eg, PubMed) through February 26, 2025, using terms related to “ketamine” and “catatonia.” All abstracts and titles were independently screened by 2 authors (P.B.v.d.M. and S.V.), who also independently reviewed the full-text manuscripts for inclusion in the systematic review when deemed relevant. Inclusion criteria required adults (≥18 years); diagnosed with catatonia (using Diagnostic and Statistical Manual of Mental Disorders [DSM] or International Classification of Diseases [ICD] criteria or validated rating scales); treated with racemic ketamine, arketamine, or esketamine; an outcome assessing severity of catatonia; and manuscript language of English, Spanish, Portuguese, Dutch, German, or French. Nonhuman studies, reviews, and reports on anesthetic/recreational ketamine use were excluded. Quality assessment of case reports was done with the Joanna Briggs Institute critical appraisal checklist consisting of 8 aspects.
Results
A total of 998 unique records were identified, of which 24 full-text articles were screened, and 9 articles reporting 10 unique patient cases were included. Patient characteristics are shown in Table 1. Most patients were female (n = 9), were aged 23–81 years, and had a mood disorder, most commonly major depressive disorder (n = 5). Catatonic symptoms frequently included mutism (n = 7), stupor (n = 7), and withdrawal (n = 8). Most patients had failed lorazepam treatment (n = 6), while ECT was attempted in only 3 patients.
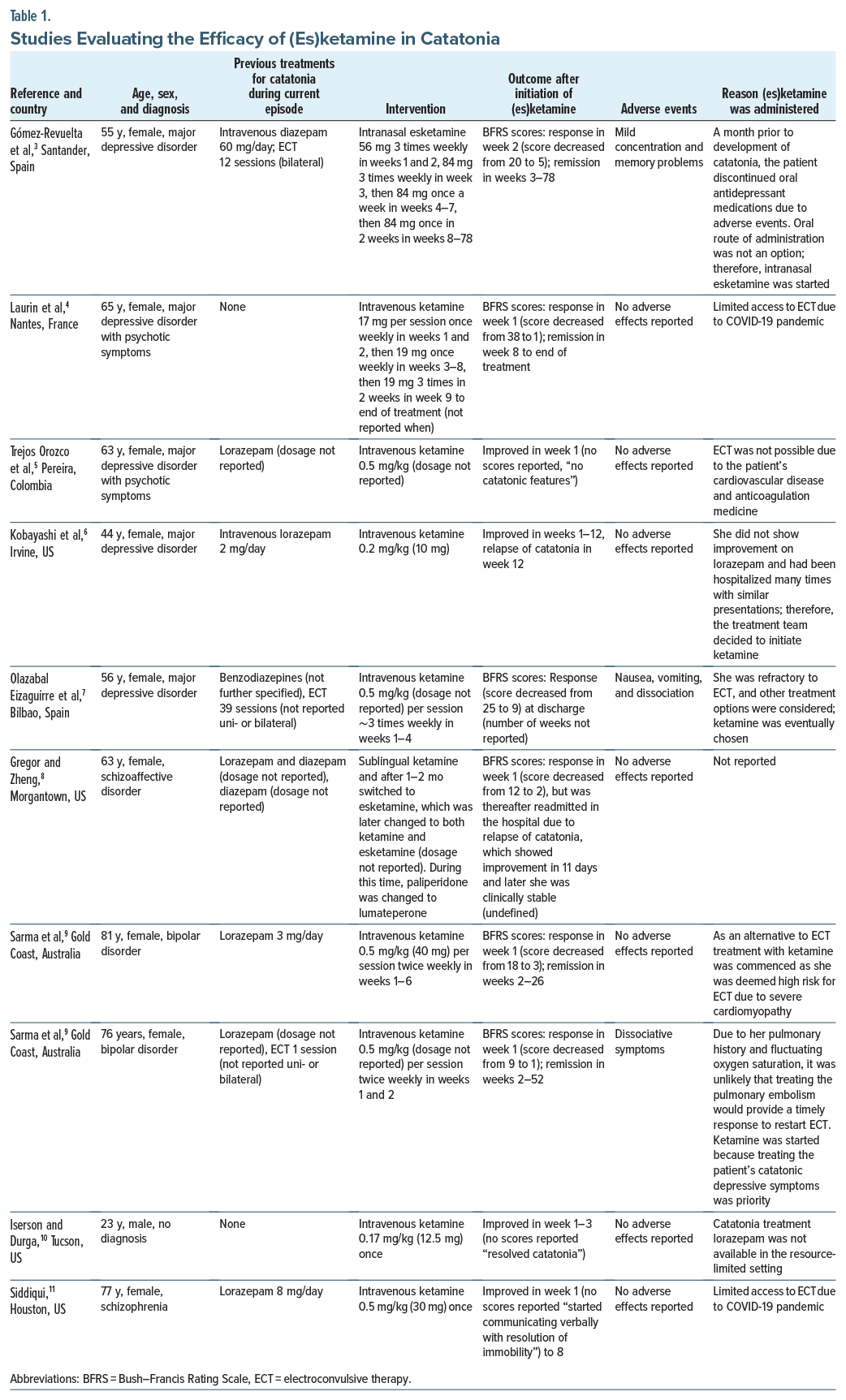
Interventions varied: 9 patients received intravenous, sublingual, or intramuscular racemic ketamine (10–40 mg), while 2 received intranasal esketamine (56–84 mg). Symptom improvement was observed in all patients, often within hours to days after administration. In 6 patients, the Bush–Francis Catatonia Rating Scale was used: 4 patients (of 6) achieved response (≥50% symptom reduction) within 1 week; 1 in the second week; and 1 at discharge. Remission (no symptoms of catatonia) was achieved in 2 patients (of 6) within 2 weeks, and in 2 later during follow-up. Most aspects were relatively well reported by the authors (eg, demographics, patient’s history), except for diagnostic tests and adverse events, which were reported on by less than half of the authors.
Discussion
These findings align with earlier work on NMDA antagonists (eg, amantadine) as third-line options after lorazepam and ECT or as second-line options, especially if ECT is unavailable or severe somatic complications will complicate ECT.12 Notably, (es)ketamine offers diverse administration routes, useful in severely withdrawn or stuporous patients unable to take oral medications. Given its rapid efficacy and tolerability, especially in major depressive disorder, the most common underlying diagnosis, (es)ketamine may offer a dual therapeutic benefit. Importantly, concerns that (es)ketamine may exacerbate mania or psychosis in bipolar or schizophrenia spectrum patients were not supported in a recent systematic review and cohort studies.13–15 This suggests that use of (es)ketamine may be safe in catatonia patients nonresponsive to lorazepam and/or ECT. Nevertheless, limitations include variable dosing, heterogeneity in catatonia severity and etiology, and potential publication bias. While randomized controlled trials are unlikely due to catatonia’s rarity, systematic synthesis of case reports remains vital in guiding treatment for this life-threatening condition.
Article Information
Published Online: October 13, 2025. https://doi.org/10.4088/JCP.25br15940
© 2025 Physicians Postgraduate Press, Inc.
J clin Psychiatry 2025;86(4):25br15940
To Cite: van der Meer PB, Verboeket S, Slooter AJC, et al. Treatment with (es)ketamine in catatonia: a systematic review of case reports. J Clin Psychiatry 2025;86(4): 25br15940.
Author Affiliations: Department of Neurology, Leiden University Medical Center, Leiden University, Leiden, The Netherlands (van der Meer); Department of Psychiatry, University Medical Center Utrecht Brain Center, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands (van der Meer, Slooter, Somers, Batalla, Dols); Department of Research and Jellinek, Arkin Mental Health Care, Amsterdam, University of Amsterdam, Amsterdam, The Netherlands (Verboeket); Department of Intensive Care Medicine, University Medical Center Utrecht Brain Center, University Medical Center Utrecht, Utrecht University, Utrecht, The Netherlands (Slooter); Department of Research Policy, Leiden University Medical Center, Leiden University, Leiden, The Netherlands (Schoones); Department of Psychiatry, Leiden University Medical Center, Leiden University, Leiden, The Netherlands (Noorden).
Corresponding Author: Pim B. van der Meer, MD, PhD, University Medical Centre Utrecht, Heidelberglaan 100, 3584 CX, Utrecht, The Netherlands ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
References (15)

- Hirjak D, Rogers JP, Wolf RC, et al. Catatonia. Nat Rev Dis Primers. 2024;10(1):49. PubMed CrossRef
- Pelzer ACM, van der Heijden FMMA, den Boer E. Systematic review of catatonia treatment. Neuropsychiatr Dis Treat. 2018;14:317–326. PubMed CrossRef
- Gómez-Revuelta M, González JR, Liebo PAH, et al. Intranasal esketamine monotherapy for ultra-resistant catatonia: a case report. Psychiatry Res. 2024;337:115923. PubMed
- Laurin A, Capelle N, Bukowski N, et al. Kétamine et lorazépam : un traitement de la dépression catatonique du sujet âgé. Encephale. 2023;49(5):535–536. PubMed CrossRef
- Trejos OE, Guriérrez Segura J, Ochoa Orozco S. Safety and efficacy of ketamine in a patient with psychotic depression, cardiovascular disease, and starvation risk. Rev Médica Risaralda. 2022;28:151–154.
- Kobayashi B, Wright C, Burns M, et al. Ketamine for acute catatonia: a case report. Curr Psychiatry. 2021;20(6):24–28.
- Olazabal Eizaguirre N, Bustamante Madariaga S, Osa Fernández L, et al. Depresión psiótica y catatonía crónica resistentes a terapia electroconvulsiva. Descripción de un caso de tratamiento con ketamina. Psiquitría Biológica. 2016;23(1):36–39.
- Gregor EA, Zheng W. Oral and intranasal ketamine use in treatment-resistant catatonia: a clinical case report. Am J Case Rep. 2023;24:e939530. PubMed CrossRef
- Sarma S, Arunachalam A, Kamara M, et al. Ketamine as an alternative to ECT in catatonia in elderly women with bipolar disorder: a case report. Front Psychiatry. 2023;14:1138772. PubMed CrossRef
- Iserson KV, Durga D. Catatonia-like syndrome treated with low-dose ketamine. J Emerg Med. 2020;58(5):771–774. PubMed CrossRef
- Siddiqui A. Intravenous ketamine successfully treats treatment-resistant catatonia in schizophrenia: a case report. Pharmacotherapy. 2024;44(10):822–824. PubMed CrossRef
- Beach SR, Gomez-Bernal F, Huffman JC, et al. Alternative treatment strategies for catatonia: a systematic review. Gen Hosp Psychiatry. 2017;48:1–19. PubMed CrossRef
- Veraart JKE, Smith-Apeldoorn SY, Spijker J, et al. Ketamine treatment for depression in patients with a history of psychosis or current psychotic symptoms: a systematic review. J Clin Psychiatry. 2021;82(4):20r13459. PubMed CrossRef
- Santucci MC, Ansari M, Nikayin S, et al. Efficacy and safety of ketamine/esketamine in bipolar depression in a clinical setting. J Clin Psychiatry. 2024;85(4):24m15376. PubMed CrossRef
- Fancy F, Rodrigues NB, Di Vincenzo JD, et al. Real-world effectiveness of repeated ketamine infusions for treatment-resistant bipolar depression. Bipolar Disord. 2023;25(2):99–109. PubMed CrossRef
This PDF is free for all visitors!