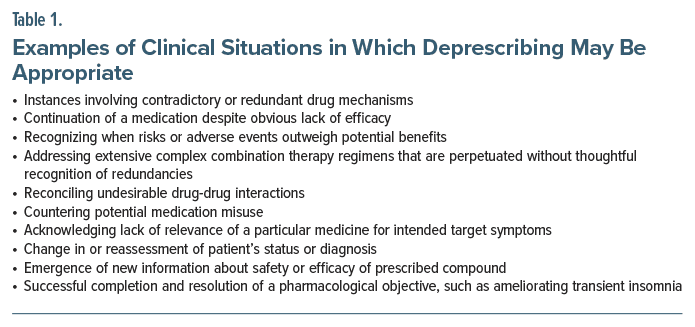
In 2025, the American Society of Clinical Psychopharmacology (ASCP) convened a task force of international experts to develop consensus recommendations, using an iterative Delphi process, about when and under what conditions psychiatric medications should be discontinued. The task force chose the term “deprescribing,” based on its extant use, to describe the process of identifying, modifying, dose-tapering, or discontinuing medications that are deemed inappropriate, ineffective, redundant, obsolete, detrimental, futile, or simply overused for a given patient. Examples of situations where the need for such purposeful dose-tapering and/or discontinuations might arise are described in Table 1 and will be the focus of more extensive discussion in future publications. However, the task force observed a considerable diversity of opinions about the meaning of the word “deprescribing” itself, prompting the current communication focused on the definition and implications of the term.
The term “deprescribing” entered the medical lexicon in 2003 to describe simplifying complex or possibly inappropriate pharmacology regimens in older adults.1 While there is presently no consensus-based or externally validated operational definition of the term, Gupta and Cahill2 proposed “the planned and supervised process of reducing or stopping medication for which existing or potential harms outweigh existing or potential benefits, taking into account the patient’s medical status, current level of functioning, and values and preferences.” Despite its meaning being open to interpretation, the term has become widely adopted throughout all areas of medicine, including cardiology (eg, the elimination of redundant antihypertensives3,4), gastroenterology (eg, halting long-term proton pump inhibitors for gastroesophageal reflux5), endocrinology (eg, “deintensification” of oral hypoglycemic polydrug medicines6), gynecology (eg, gauging risks versus benefits for continuing or discontinuing hormone replacement therapy in women after age 657), neurology (eg, overuse of migraine polypharmacy regimens8), and palliative care (eg, simplifying comfort care pharmacotherapies at end of life9).
In psychiatry, uniquely, controversy surrounds the use of the term “deprescribing” because of implications about its value-laden psychosocial—and perhaps political—meanings rather than the appropriateness of the treatment regimen based on pharmacodynamic, pharmacokinetic, or other clinical grounds. Specifically, the “antipsychiatry” community has made unwarranted accusations about toxicity from all psychiatric medicines, espousing that these compounds should be eliminated (“deprescribed”) because of perceptions that in toto, they do more harm than good.10 The extent to which both patients and some mental health practitioners may associate the term “deprescribing” with this ill-founded effort to eliminate indicated psychiatric medications is unknown. Nevertheless, there was hesitation among some Delphi workgroup members to reify a term that has been misused in the media (“deprescribing”), instead suggesting an alternate term such as “discontinuing.” The task force ultimately opted to retain the word “deprescribing” for the following reasons:
- The decision to prescribe or deprescribe any treatment implies a thoughtful, ongoing process that includes not only its initiation and dosing, as well as monitoring and assessment of beneficial and adverse effects, but also active decisions about when and why to end it.
- “Deprescribing” captures the concepts of dose optimization and tapering, as opposed to medication “cessation” as a categorical step without nuance or implied ongoing clinical monitoring.
- “Deprescribing” may be construed beyond its straightforward meaning that is the act of halting a therapy (“discontinuing a treatment”) and instead be regarded as a less neutral action that is meant to redress a possible decision-making error such as the use of an inappropriate medication for a given condition, failure to recognize a consequential drug-drug interaction within a broader regimen, or overly prolonged continuation of a medication that has outlived its usefulness.
- The term “discontinuation,” when applied to medication, fails to discriminate decisions to stop a medication that are unilateral (either by the patient or the prescriber) versus those that have been arrived at through shared decision-making. For example, prescribers who discontinue a medication as passive acquiescence to patient nonadherence or medication refusal; or, prescriber initiated halting of a controlled substance over the possible objection of a patient who perceives a benefit that the prescriber disputes.
- Prescribers of psychiatric medications have a crucial role to educate the patient comprehensively (and their families as appropriate) on risks and benefits of a treatment, alternatives, and risks of the untreated disorders in order to make collaborative, thoughtful decisions. The patient’s autonomy is a major respected factor in treatment decisions, and treatments should be revisited together over time regarding risks and benefits to the individual.
In our view, deprescribing should not be misconstrued to imply that any medication being tapered or stopped was de facto initially inappropriate, as the antipsychiatry community might wish to imply. Rather, it reflects the dynamic process of clinical oversight as a patient’s clinical condition or therapeutic risk-benefit considerations change over time. A decision to reverse course in a treatment trajectory may reflect evolving knowledge about a disease state or particular patient’s circumstances—as when a patient receiving clozapine develops agranulocytosis, or when tachyphylaxis renders a previously effective medication no longer helpful. Failure to keep pace with changes in a patient’s condition over time could make once appropriate medications no longer appropriate, which could make continuing to prescribe those medications a potential deviation from proper care.
Deprescribing as “curation” thus implies a dynamic evaluative decisional process that occurs over time, which the term “discontinuation” fails to fully capture—for example, tapering rather than stopping a medicine to avoid rebound effects, active symptom monitoring and surveillance after a treatment has ended, restarting a stopped treatment if symptoms recur, or replacing one medication with another if, and when, a better option becomes apparent. The term “deprescribing” also embraces the idea of judging when a course of treatment has reached a logical endpoint (as when terminating antidepressant medications after sustained euthymia following a single episode of major depression), or overseeing the monitored tapering of high-dose benzodiazepines after tolerance becomes apparent. By contrast, the term “medication discontinuation” may not capture that longitudinal process in which nuanced patient-specific decisions inform dosing modification strategies over time or the appreciable impact that stopping one component of a therapeutic regimen may have on the remaining elements.
Prescribing, represcribing, and deprescribing might collectively be construed as phases of iterative decision-making that consider the implications of treatment initiation, continuation, and cessation. It signals a fluid process that is more sophisticated and multifaceted than the sheer act of discontinuing a medication. We therefore encourage the field to destigmatize the term “deprescribing” from its misappropriated usage, explicate its accurate definition, and reclaim its purposeful meaning in ways that are akin to its use in all other medical specialties.
Article Information
Published Online: June 2, 2025. https://doi.org/10.4088/JCP.25ac15936
© 2025 Physicians Postgraduate Press, Inc. J Clin Psychiatry 2025;86(4):25ac15936
To Cite: Goldberg JF, Swartz HA, Mago R, et al. What is meant by the term “deprescribing,” and does it belong in our lexicon? J Clin Psychiatry 2025;86(4):25ac15936.
Author Affiliations: Department of Psychiatry, Icahn School of Medicine at Mount Sinai, New York, New York (Goldberg); Department of Psychiatry, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania (Swartz); Department of Psychiatry, SUNY Upstate Medical University, Syracuse, New York (Mago); Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania (Mago); Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada (McIntyre); Academic Department of Psychiatry, Kolling Institute, Northern Clinical School, Faculty of Medicine and Health, The University of Sydney, Sydney, New South Wales, Australia (Malhi); CADE Clinic and Mood-T, Royal North Shore Hospital, St. Leonards, New South Wales, Australia (Malhi); Department of Psychiatry, University of Oxford, Oxford, UK and Oxford Uehiro Centre for Practical Ethics, Faculty of Philosophy, University of Oxford, Oxford, UK (Malhi); Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada (Rosenblat); Mood Disorders Psychopharmacology Unit, University Health Network, Toronto, Ontario, Canada (Rosenblat); Department of Psychiatry, Ammon-Pinizzotto Center for Women’s Mental Health at Massachusetts General Hospital, Boston, Massachusetts (Freeman); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (Freeman); Bipolar and Depressive Disorders Unit, Hospital Clínic de Barcelona, Barcelona, Spain (Vieta); Institute of Neurosciences (UBNeuro); Institut d’Investigacions Biomèdiques August Pi i Sunyer (IDIBAPS), Barcelona, Spain (Vieta); Biomedical Research Networking Centre on Mental Health (CIBERSAM), Instituto de Salud Carlos III (ISCIII) (Vieta); Department of Medicine, School of Medicine and Health Sciences, University of Barcelona, Barcelona, Spain (Vieta); Department of Psychiatry, Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania (Thase); Philadelphia Veterans Affairs Medical Center, Philadelphia, Pennsylvania (Thase); Department of Psychiatry & Behavioral Sciences, University of New Mexico, Albuquerque, New Mexico (Tohen); Department of Psychiatry and Behavioral Sciences, New York Medical College, Valhalla, New York (Citrome).
Corresponding Author: Joseph F. Goldberg, MD, Department of Psychiatry, Icahn School of Medicine at Mount Sinai, 128 East Ave, Norwalk, CT 06851 ([email protected]).
Relevant Financial Relationships: Dr Goldberg has been a consultant for Abbvie, Alkermes, AIvogen, Genomind, Luye Pharma, Neumora, and Otsuka; has been on the speakers/advisory boards of Alkermes, Axsome, Bristol-Myers Squibb, and Intracellular Therapies; and has received royalties from American Psychiatric Publishing and Cambridge University Press. Dr Swartz has received honoraria from Medscape/WebMD, Clinical Education Alliance, Mediflix, Intracellular Therapies and other financial or material support from Wolters Kluwer, American Psychiatric Association Press, and New Harbinger Publications. Dr McIntyre has been a consultant for and received honoraria from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Neurawell, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, Abbvie, Bristol-Myers Squibb, and Atai Life Sciences and has received grant/ research support from CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute. Dr Malhi is an employee of The University of Sydney and NSW Health; has been a consultant for AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka, and Servier; has received grant or research support from National Health and Medical Research Council, Australian Rotary Health, NSW Health, American Foundation for Suicide Prevention, Ramsay Research and Teaching Fund, Elsevier, AstraZeneca, Janssen-Cilag, Lundbeck, Otsuka, and Servier; and is the recipient of an investigator-initiated grant from Janssen-Cilag (PoET Study), joint grant funding from the University of Sydney and National Taiwan University (Ignition Grant), and grant funding from The North Foundation. Dr Rosenblat has been on the speakers/advisory boards of Boehringer Ingelheim and AbbVie. As an employee of Massachusetts General Hospital, Dr Freeman works with the MGH CTNI and MGH Center for Women’s Mental Health, which has had research funding from multiple pharmaceutical companies and NIMH. MGH National Pregnancy Registry: Current Sponsors: Alkermes, Inc. (2016–present); Dr. Reddy’s Laboratories, Inc. (2023–present); Eisai Inc. (2022– present); Otsuka America Pharmaceutical, Inc. (2008–present); Supernus Pharmaceuticals (2021–present); Teva Pharmaceutical Industries Ltd. (2018–present). Past Sponsors: Forest/Actavis/Allergan (2016–2018, declined to sponsor: 2018–present); Aurobindo Pharma (2020–2022, declined to sponsor: 2022–present); AstraZeneca Pharmaceuticals (2009–2014, declined to sponsor: 2014–present); AuroMedics Pharma LLC (2021–2022, declined to sponsor: 2022–present); Johnson & Johnson/Janssen Pharmaceuticals, Inc (2019–2023, declined to sponsor: 2024–present); Ortho-McNeil-Janssen Pharmaceuticals, Inc (2009–2014, declined to sponsor: 2015–present); Pfizer, Inc. (2009–2011, declined to sponsor: 2012–present); Sage Therapeutics (2019–2023, declined to sponsor 2024–present); Sunovion Pharmaceuticals, Inc. (2011–2023, declined to sponsor: 2024–present). Updated sponsors can be found at: https://womensmentalhealth.org/research/pregnancyregistry/. Research through MGH: Sage, NIA, NIMH. Consulting through CTNI. Advisory boards or consulting, data safety committees/independent data safety and monitoring committees: Janssen (Johnson & Johnson), Novartis, Neurocrine, Eliem, Sage, Brainify, Everly Health, Tibi Health, Relmada, Beckley Psytech, Brii Biotech, Reunion. Educational activities (speaking, planning): MGH Psych Academy, WebMD, Medscape, PriMed, Postpartum Support International, PRIME, HMP Global, CME Institute. Dr Vieta has been a consultant for Abbvie, Angelini, AstraZeneca, Biogen, Biohaven, Bristol-Myers Squibb, Celon, Compass, Ferrer, GH Research, Gedeon Richter, HMNC, Idorsia, Janssen, Jazz, Lilly, Lundbeck, Merck Sharp & Dohme, Newraxpharm, Newron, Novartis, Organon, Otsuka, Pfizer, Roche, Sage, Sanofi-aventis, Servier, Shire, Sunovion, Takeda, and Teva; has received grant/research support from AB-Biotics, Abbvie, Almirall, AstraZeneca, BeckleyPsych, Boehringer-Ingelheim, Bristol-Myers Squibb, Celon, Cephalon, Compass, Dainippon Sumitomo Pharma, Elan, Ferrer, GH Research, GlaxoSmithKline, Intra-Cellular, Janssen, Lilly, Lundbeck, Orion, Otsuka, Pfizer, Sanofi-Aventis, Servier, Sunovion, and Takeda; has been on the speakers/advisory boards of Abbvie, Angelini, AstraZeneca, Biogen, Biohaven, Bristol Myers Squibb, Celon, Compass, Ferrer, GH Research, Gedeon Richter, HMNC, Idorsia, Janssen, Jazz, Lilly, Lundbeck, Merck Sharp & Dohme, Newraxpharm, Newron, Novartis, Organon, Otsuka, Pfizer, Roche, Sage, Sanofi-Aventis, Servier, Shire, Sunovion, Takeda, and Teva; and has received other financial or material support from Abbott, Abbvie, Adamed, Angelini, AstraZeneca, Bristol Myers Squibb, Cambridge University Press, Elsevier, Farmindustria, Ferrer, Galenica, GlaxoSmithKline, Janssen, Johnson & Johnson, Lilly, Lundbeck, Oxford University Press, Otsuka, Pfizer, Sanofi-Aventis, and Viatris. Dr Thase has been a consultant for Autobahn Therapeutics, Axsome Therapeutics, Inc, Clexio Biosciences, Gerson Lehman, GH Therapeutics, H. Lundbeck, A/S, Janssen Pharmaceuticals, Inc, Johnson & Johnson, Luye Pharma Group, Ltd, Merck & Company, Inc, Object Pharma, Otsuka Pharmaceutical Company, Ltd, Pfizer, Inc, Sage Pharmaceuticals, Seelos Pharmaceuticals, and Takeda Pharmaceutical Company, Ltd; has received grant/research support from Acadia Inc, Alkermes, Axsome Therapeutics Inc, Intracellular, Inc, Janssen Pharmaceuticals, Inc, Myriad, National Institute of Mental Health, Otsuka Pharmaceutical Company, Ltd, Patient-Centered Outcomes Research Institute (PCORI), and Takeda Pharmaceutical Company, Ltd; and has received royalties from American Psychiatric Foundation, Guilford Publications, Herald House, and Kluwer-Wolters, and W.W. Norton & Company, Inc. His spouse is employed by Open Health. Dr Tohen has received honoraria from and been on speakers/advisory boards of Abbvie, Alkermes, Merck, Otsuka, Lundbeck, Biohaven, Intracellular Therapies, and Autobahn. Dr Citrome has been a consultant for AbbVie/Allergan, Acadia, Adamas, Adheretech, Alkermes, Alumis, Angelini, Astellas, Autobahn, Avanir, Axsome, Biogen, BioXcel, Bristol-Myers Squibb, Boehringer Ingelheim, Cadent Therapeutics, Cerevel, Clinilabs, COMPASS, Delpor, Draig Therapeutics, Eisai, Enteris BioPharma, HLS Therapeutics, Idorsia, INmune Bio, Impel, Intra-Cellular Therapies, Janssen, Karuna, Lundbeck, Luye, Lyndra, MapLight, Marvin, Medavante-ProPhase, Merck, Mitsubishi-Tanabe Pharma, Neumora, Neurocrine, Neurelis, Noema, Novartis, Noven, Otsuka, Ovid, Praxis, Recordati, Relmada, Reviva, Sage, Sumitomo/Sunovion, Supernus, Teva, University of Arizona, Vanda, and Wells Fargo and done one-off ad hoc consulting for individuals/entities conducting marketing, commercial, or scientific scoping research; has been on speakers/advisory boards for AbbVie/Allergan, Acadia, Alkermes, Angelini, Axsome, BioXcel, Bristol-Myers Squibb, Eisai, Idorsia, Intra-Cellular Therapies, Janssen, Lundbeck, Neurocrine, Neopharm, Noven, Otsuka, Recordati, Sage, Sunovion, Takeda, Teva, and Vanda and for CME activities organized by medical education companies such as Medscape, NACCME, NEI, Vindico, and universities and professional organizations/societies; is a stock shareholder (small number of shares of common stock) in Bristol-Myers Squibb, Eli Lilly, J & J, Merck, and Pfizer (purchased >10 years ago) and has stock options in Reviva; and has received royalties/publishing income from Taylor & Francis (Editor-in-Chief, Current Medical Research and Opinion, 2022-date), Wiley (Editor-in-Chief, International Journal of Clinical Practice, through end 2019), UpToDate (reviewer), Springer Healthcare (book), Elsevier (Topic Editor, Psychiatry, Clinical Therapeutics, through Spring). Dr Mago reports no relevant financial relationships.
Funding/Support: None.
![]() The ASCP Corner, edited by Leslie L. Citrome, MD, MPH, is a collection of brief peer-reviewed, evidence-based articles, authored by American Society of Clinical Psychopharmacology members, that examine the practice of psychopharmacology through the lens of clinical experience. The information contained herein only represents the opinion of the author(s). See more ASCP Corner Articles at Psychiatrist.com/ASCP-Corner
The ASCP Corner, edited by Leslie L. Citrome, MD, MPH, is a collection of brief peer-reviewed, evidence-based articles, authored by American Society of Clinical Psychopharmacology members, that examine the practice of psychopharmacology through the lens of clinical experience. The information contained herein only represents the opinion of the author(s). See more ASCP Corner Articles at Psychiatrist.com/ASCP-Corner
The editor of the ASCP Corner, Leslie Citrome, MD, MPH, recused himself from the peer review process. J. Craig Nelson, MD, founding editor of the ASCP Corner, oversaw the peer review process for this manuscript.
References (10)

- Woodward M. Deprescribing: achieving better health outcomes for older people through reducing medications. J Pharm Pract Res. 2003;33:323–328. CrossRef
- Gupta S, Cahill JD. A prescription for “deprescribing” in psychiatry. Psychiatr Serv. 2016;67(8):904–907. CrossRef
- Oliveira MG, Moreira PM, Amorim WW, et al. Deprescribing hypertension medication in older adults: can it lower drug burden without causing harm?. Clin Geriatr Med. 2024;40(4):659–668.
- Krychtiuk KA, Gersh BJ, Washam JB, et al. When cardiovascular medicines should be discontinued. Eur Heart J. 2024;45(23):2039–2051. CrossRef
- Schulthess-Lisibach AE, Lüthold RV, Tombez C, et al. DepRescribing inappropriate Proton Pump InhibiTors (DROPIT): study protocol of a cluster-randomised controlled trial in Swiss primary care. BMJ Open. 2025;15(1):e094495.
- Abdelhafiz AH, Sinclair AJ. Deintensification of hypoglycaemic medications-use of a systematic review approach to highlight safety concerns in older people with type 2 diabetes. J Diabetes Complications. 2018;32(4):444–450. PubMed CrossRef
- Baik H, Baye F, McDonald CJ. Use of menopausal hormone therapy beyond age 65 years and its effects on women’s health outcomes by types, routes, and doses. Menopause. 2024;31(5):363–371. CrossRef
- Martelletti P, Luciani M, Spuntarelli V, et al. Deprescribing in migraine. Exp Opin Drug Saf. 2021;20(6):623–625. CrossRef
- Thompson J. Deprescribing in palliative care. Clin Med (Long). 2019;19(4):311–314. PubMed CrossRef
- Read J, Moncrieff J. Depression: why drugs and electricity are not the answer. Psychol Med. 2022;52(8):1401–1410. CrossRef
This PDF is free for all visitors!




