This work may not be copied, distributed, displayed, published, reproduced, transmitted, modified, posted, sold, licensed, or used for commercial purposes. By downloading this file, you are agreeing to the publisher’s Terms & Conditions.
Article Abstract
Objective: Because patients with mental illness can die prematurely, we sought to determine if undetected cardiovascular disease might be present in a psychiatric day treatment population.
Method: We studied 96 patients in a day treatment program seen between February 2011 and August 2012. Data were obtained through an electronic medical record database. Electrocardiographic diagnoses were assigned by 1 investigator (M.L.). Medications were categorized into classes, and problem lists revealed comorbid diagnoses. Fisher exact test (2-tailed) and analysis of variance were used to compare findings between patient groups. Electrocardiogram (ECG) findings were the primary outcome measure.
Results: Ninety-two ECGs were performed in 37 patients. Of these 37 patients, 70% were women, 65% were 50 years of age or younger, and 54% were people of color. ECGs were performed mainly for chest pain/dyspnea (46%) and overdose/altered mental status (27%). Of these 37 patients, 20 (54%) had abnormal ECGs, 7 (19%) had borderline findings, and 10 (27%) had normal studies. When compared with the larger group of 59 patients without ECG testing, those with abnormal ECGs were more likely to be older (mean age=47 vs 37 years, P<.001) and have more comorbid conditions (mean no.=10.0 vs 3.8, P<.0001). The most common abnormalities were conduction disorders (prolonged QRS≥105 ms, or prolonged QTc≥450 ms in men or≥460 ms in women), coronary artery disease, and arrhythmias.
Conclusions: In psychiatric outpatients who underwent ECG testing, mainly for chest pain or altered mental status, over 50% had concerning findings. Older patients with multiple comorbidities were at higher risk of having abnormal ECGs. Generalizability of these findings depends on validation in larger samples in multiple settings.
Prim Care Companion CNS Disord 2013;15(3):doi:10.4088/PCC.12m01484
© Copyright 2013 Physicians Postgraduate Press, Inc.
Submitted: October 22, 2012; accepted February 18, 2013.
Published online: May 9, 2013.
Corresponding author: Mark Linzer, MD, Division of General Internal Medicine, Hennepin County Medical Center (HCMC), 701 Park Ave (P7), Minneapolis, MN 55415 ([email protected]).
Electrocardiographic Abnormalities as Potential Contributors to Premature Mortality in Patients With Mental Illness in a Psychiatric Day Treatment Program
ABSTRACT
Objective: Because patients with mental illness can die prematurely, we sought to determine if undetected cardiovascular disease might be present in a psychiatric day treatment population.
Method: We studied 96 patients in a day treatment program seen between February 2011 and August 2012. Data were obtained through an electronic medical record database. Electrocardiographic diagnoses were assigned by 1 investigator (M.L.). Medications were categorized into classes, and problem lists revealed comorbid diagnoses. Fisher exact test (2-tailed) and analysis of variance were used to compare findings between patient groups. Electrocardiogram (ECG) findings were the primary outcome measure.
Results: Ninety-two ECGs were performed in 37 patients. Of these 37 patients, 70% were women, 65% were 50 years of age or younger, and 54% were people of color. ECGs were performed mainly for chest pain/dyspnea (46%) and overdose/altered mental status (27%). Of these 37 patients, 20 (54%) had abnormal ECGs, 7 (19%) had borderline findings, and 10 (27%) had normal studies. When compared with the larger group of 59 patients without ECG testing, those with abnormal ECGs were more likely to be older (mean age = 47 vs 37 years, P < .001) and have more comorbid conditions (mean no. = 10.0 vs 3.8, P < .0001). The most common abnormalities were conduction disorders (prolonged QRS ≥ 105 ms, or prolonged QTc ≥ 450 ms in men or ≥ 460 ms in women), coronary artery disease, and arrhythmias.
Conclusions: In psychiatric outpatients who underwent ECG testing, mainly for chest pain or altered mental status, over 50% had concerning findings. Older patients with multiple comorbidities were at higher risk of having abnormal ECGs. Generalizability of these findings depends on validation in larger samples in multiple settings.
Prim Care Companion CNS Disord 2013;15(3):doi:10.4088/PCC.12m01484
© Copyright 2013 Physicians Postgraduate Press, Inc.
Submitted: October 22, 2012; accepted February 18, 2013.
Published online: May 9, 2013.
Corresponding author: Mark Linzer, MD, Division of General Internal Medicine, Hennepin County Medical Center (HCMC), 701 Park Ave (P7), Minneapolis, MN 55415
([email protected]).
Although the increased mortality among patients with psychiatric disorders has been reported by numerous investigators,1–6 the mortality gap between patients with mental illness and those without has remained wide.7 Reasons for this disparity include accidents, lack of selfcare, violence, and suicide. There is also advanced risk due to poverty, smoking, and lack of exercise.8 However, less attention has been directed toward medical disorders that accompany psychiatric illness, many of which may be attributed to side effects from psychotropic medications,8,9 including weight gain, prediabetes, and dyslipidemias. Thus, while
the psychiatric patient may have many risk factors, it is not clear that our care systems identify this risk or work assertively with our patients to modify it.
Hennepin County Medical Center (HCMC), Minneapolis, Minnesota, recently started a program in Medical Psychiatry to integrate medical and psychiatric care for patients with mental illness. In this program, we have placed an internist in a psychiatric outpatient setting, the day treatment program. Patients usually enroll in the day treatment program after prolonged psychiatric hospital stays. The program consists of daily care on weekdays, with group therapy sessions and other programs aimed at improving the patient’s ability to function. In 2011, after noting premature coronary artery disease and abnormal electrocardiograms (ECGs) among a small number of psychiatric outpatients, the authors decided to systematically review medical records of day treatment patients to determine the prevalence and nature of ECG findings. Our hypothesis was that ECGs performed on our psychiatric outpatients would display abnormal findings that might explain, in part, the premature mortality of patients with mental illness. We secondarily sought to determine if some medication classes would be overrepresented among patients with abnormal ECGs and if cardiovascular outcomes were more prevalent in this subgroup.
METHOD
This was a cohort study of all patients (N = 96) seen in the psychiatric day treatment program at HCMC for the first time between February 3, 2011, and June 20, 2011, with ECGs performed between March 25, 2010, and September 6, 2011. ECG findings were the primary outcome measure. Data were collected through an electronic medical record database, Clarity (Epic, Verona, Wisconsin). A preliminary chart audit of 10 charts showed that Clarity was accurate in terms of age, sex, and ethnicity but had discrepancies in assessing diagnoses (through problem lists) and medications. We thus performed a chart audit of 50% of the records of those who underwent ECG testing to assess disagreement rates in determining diagnoses and medications and to use these data to improve the methods with which data were drawn from Clarity.
All ECGs were assessed by one investigator (M.L.), a general internist at HCMC. The investigator first reviewed the interpretation from the cardiologist who had reviewed the ECG for the medical record.
The final reading was determined by the investigator; but in cases in which the investigator felt there was uncertainty (eg, nonspecific Q waves versus an old myocardial infarction [MI]), the ECG was reviewed by a cardiologist (G.S.). Abnormal ECG findings were categorized as (1) conduction disorders (heart block, bundle branch blocks, intraventricular conduction defects [QRS ≥ 105 ms], prolonged QTc intervals [≥ 450 ms in males and ≥ 460 ms in females], and paced rhythm); (2) arrhythmias (sinus bradycardia ≤ 50bpm, sinus tachycardia ≥ 120 bpm, atrial fibrillation, multiple premature ventricular contractions); (3) coronary artery disease (evidence of Q wave infarcts); (4) nonspecific T wave abnormalities; and (5) structural abnormalities (left or right ventricular hypertrophy). A separate category, borderline findings, included low voltage, sinus bradycardia (> 50, < 60 bpm), sinus tachycardia (> 100, <120 bpm), early repolarization, and nonspecific Q waves. Remaining ECGs were considered normal.
Because several patients had multiple ECGs, we constructed a hierarchy to determine the most abnormal ECG (to provide a date for assessing diagnoses and medication use at the time the ECG was performed). The hierarchy was (1) acute ischemia (most abnormal), then (2) serious arrhythmia, (3) conduction disorder, (4) coronary artery disease (prior MI), (5) structural abnormalities, (6) nonspecific T wave findings, and (7) borderline findings. Patients with multiple abnormalities moved up the scale for most abnormal ECG, and in the case of ties (eg, each ECG had 2 abnormalities), we used the ECG with the widest QRS, the longest QTc, or the most abnormal-appearing T waves.
To determine the reason the ECG was performed, 2 investigators (M.L. and K.B.) reviewed the charts of the 37 patients who had ECGs performed. Consensus was reached on a reason for the ECGs being performed in all cases. They were then summarized into 4 categories: (1) chest pain/dyspnea, (2) overdose/altered mental status, (3) routine/preoperative, and (4) other. For determining medication use, we used Clarity to assess medications at the time of the most abnormal ECG, and then 2 of us (M.L. and P.Y.) performed chart reviews of 50% of the 37 patients (about 10 patients each) who had ECGs performed. Discrepancies in medications were used to improve the specificity of the data pull from Clarity; medication lists were then revised for all subjects. The overall discrepancy rate was 7.3%, in part due to lack of consistency between medication lists and medications listed in notes from clinics, the emergency department, or the hospital. Medications were then subclassified into medication classes (eg, antipsychotics, opiates, anticonvulsants, and antidepressants) under the supervision of P.Y., a clinical pharmacist and informaticist. Problem lists were retrieved through Clarity to determine diagnoses at the time of the most abnormal ECG as well as subsequent cardiovascular diagnoses (syncope, presyncope, palpitations, tachycardias, MI, cerebrovascular accidents [CVAs], coronary artery disease, or death) and serious cardiovascular diagnoses (MI, CVA, or death) during follow-up (mean length of follow-up = 18.6 months).
We then performed a chart audit of 50% of the charts to assess the accuracy of the problem lists by comparing them with clinical notes (disagreement rate = 23.5%). Disagreements were due to problem lists having similar diagnoses listed in multiple manners, many nondiagnoses listed (eg, health maintenance examination), and missing new diagnoses (eg, diagnoses established during an emergency department visit). The final list of diagnoses used the problem lists, but we note the disagreement rate as a limitation on the accuracy of these lists. To portray the diagnoses, we collapsed them into categories (eg, cardiovascular, gastrointestinal, and endocrine). Fisher exact test (2-tailed) was used to compare medication use and rates of new and serious cardiovascular diagnoses in patients with abnormal versus normal ECGs. We also used Fisher exact test and analysis of variance to compare characteristics of those patients with abnormal ECGs to those with normal ECGs and to the larger group of patients who did not have ECGs performed.
RESULTS
Of 96 patients in the day treatment program, 37 patients had 92 ECGs performed. Of these 37 patients, 26 (70%) were female, 24 (65%) were 50 years of age or younger, and 20 (54%) were persons of color—African American (n = 15), multiracial (n = 3), Native American (n = 1), or other (n = 1). Thirty-one of the 37 patients had diagnoses listed on their problem lists at the time of the most abnormal ECG. The most frequent diagnosis was psychiatric (26 of 31 or 84%), followed by rheumatologic/musculoskeletal (58%), GI (52%), and endocrine (48%). Seventy-seven percent of patients had at least 1 diagnosis that did not fit into 1 of 16 subcategories. ECGs were usually performed for clinical concerns: 46% of the most abnormal ECGs for each patient were performed for chest pain or shortness of breath, 27% were performed in the setting of an overdose or altered mental status, 11% were “routine” or “preoperative,” and the remainder (16%) were for other reasons.
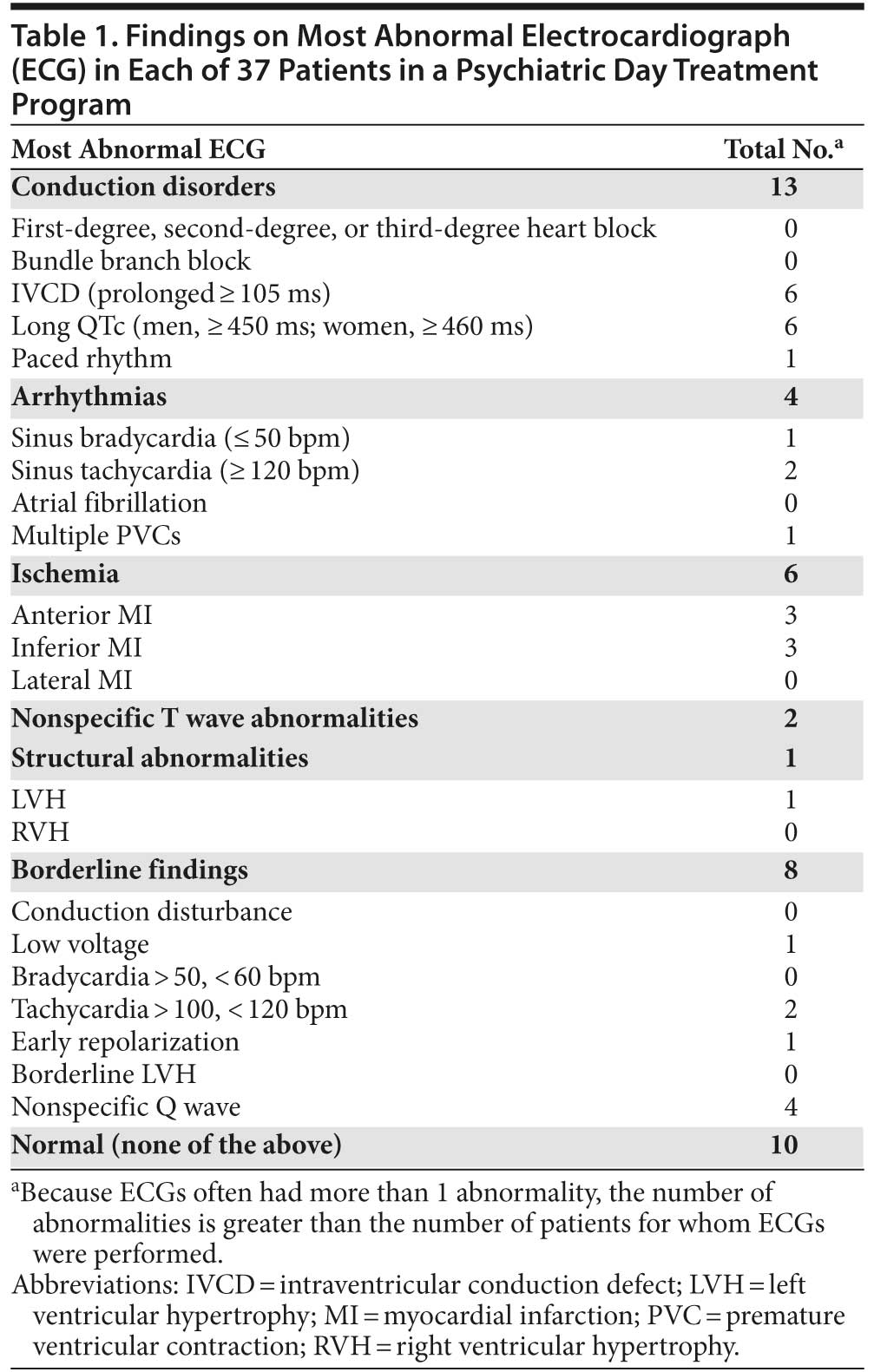
Of the 37 patients with ECGs ordered, 20 (54%) had abnormal findings, 7 (19%) had borderline findings, and 10 (27%) had normal findings. Thus, at least 21% (20 of 96) of the total population had abnormal ECG findings. Table 1 shows findings from the most abnormal ECG in the 3 categories abnormal, borderline, and normal. Because ECGs often had more than 1 abnormality, the number of abnormalities is greater than the number of patients for whom ECGs were performed. Conduction defects were the most prevalent abnormalities, occurring in 13 of 20 patients (65%) with abnormal ECGs. These were predominantly prolonged QRS complexes (nonspecific intraventricular conduction defects with QRS ≥ 105 ms) or prolonged QTc intervals (≥ 450 ms in males and 460 ms in females). QRS intervals ranged from 105 to 145 ms, with 4 of 6 patients having intervals of 115 ms or longer. QTc intervals ranged from 457 to 520 ms, with 4 of the 6 patients having intervals longer than 470 ms. Of the 20 patients, 6 (30%) had evidence of prior MI, and 4 (20%) had an arrhythmia. Seven patients had 8 borderline ECG findings, including low voltage, sinus tachycardia < 120 bpm, early repolarization, and nonspecific Q waves. Of the 37 patients, only 10 (27%) in whom an ECG was performed had a normal ECG.
The 20 patients with abnormal ECGs were about the same mean age as those patients with normal ECGs (47 vs 45 years) but considerably older than the larger group who did not undergo ECG testing (47 vs 37 years, P < .001). The mean number of comorbidities was also greater in the abnormal ECG group than in the larger group without ECG testing (10.0 vs 3.8, P < .0001).
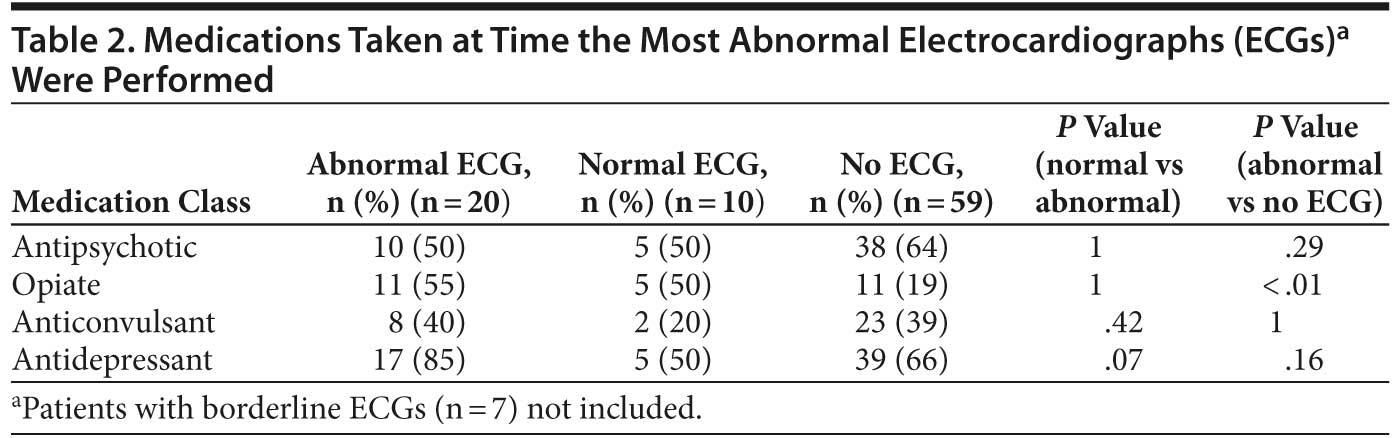
Patients were typically taking numerous medications (mean number of medications per patient in the 37 patients with ECGs performed = 15.3). We utilized standard subcategories to classify medications (eg, antipsychotics, opiates, anticonvulsants, antidepressants, quinolones) and dropped from consideration all medication groups that were unlikely to affect the ECG. We then dropped from consideration medications that were used in a very small number of patients. We then compared the use of medications in 4 remaining subclasses between patients with normal and abnormal ECGs. The categories were antipsychotics, opiates, anticonvulsants, and antidepressants (Table 2). Interestingly, there was no difference in antipsychotics between the 2 groups. Anticonvulsants were used in 40% of the patients in the abnormal ECG group and 20% of the patients with normal ECGs, but this difference was not statistically significant (P = .42). Antidepressants were used more often in patients with abnormal ECGs (85% of the abnormal ECG group, versus 50% of patients with normal ECGs), but this difference was also not statistically significant (P = .07), perhaps due to the small sample size. Opiates were more often seen in the abnormal ECG group than in the larger untested group (55% vs 19%, P < .01).
Cardiovascular diagnoses were found at the time of the most abnormal ECG in 5 of the 37 patients (14%). New cardiovascular diagnoses occurred in 6 patients, and only 2 of these cardiac outcomes were severe (stroke and death). There was no difference in the rate of new cardiovascular diagnoses or in severe cardiac outcomes in those with normal versus abnormal ECGs (P value = 1).
DISCUSSION
In this study of 96 patients in a psychiatric day treatment program, we found that 37 patients who underwent ECG testing had a high prevalence of abnormal ECGs, with the most common abnormality being conduction disorders. “Older” patients (mean age = 47 years) with more medical diagnoses appeared to be a higher-risk group. Many of the findings were seen in the setting of a medical emergency such as altered mental state or drug overdose; thus, these findings may represent the risk of psychotropic medications under situations of excess use. Our findings will require replication in other settings and larger samples in order to ascertain the true prevalence of ECG abnormalities in a day treatment population. Whether the defects that were identified by these ECG findings contribute to the premature mortality seen in patients with mental illness likewise remains to be determined.
In a study of 103 psychiatric outpatients in Great Britain in 2005,10 only 2 of 65 patients who underwent ECG testing (3%) had a prolonged QTc. Our rate was considerably higher (6 of 37 patients, or 16% of those tested). As to why our rate is so much higher, cutoffs for QT prolongation in the British study were somewhat higher (470 ms in females) than in ours, and geographical variation in types of drugs may have played a role. Hollister11 looked at 1,006 consecutive psychiatric inpatients screened with ECG testing and found 6 (< 1%) with prolonged QT intervals. An older British study12 found ECG abnormalities in 42% of 140 schizophrenic patients taking phenothiazines, with the most common findings being ST and T wave changes, P-R and QT interval prolongation, sinus tachycardia, and bundle branch block. Thus, multiple studies agree that the ECG may be a sensitive indicator of cardiac risk in psychiatric patients, but the degree of this risk appears to be variable.
When comparing our patients’ rates of ECG findings to those in the general population, the conduction disorder prevalence was considerably higher in our day treatment patients. We had 6 patients with prolonged QRS complexes (6 of 96, or a 6% rate) and 6 with prolonged QTc intervals (also 6%). In the Framingham study,13 about 1%–3% of people under 60 years of age had a mildly prolonged QRS (100–110 ms), and in 2 studies assessing prevalence of long QT syndrome, the community rate was about 1 in 2,000, or 0.05%.14,15 Larger studies will be required of psychiatric day treatment patients, however, to assess true prevalence rates of these ECG findings.
Patients who underwent ECG testing in this study often did so for a reason, usually chest pain or shortness of breath or in the setting of a drug overdose or altered mental status. Thus, these ECG findings may well have been related to the patients’ presenting clinical scenario. Our data should thus not be used to infer that symptom-free patients would have these findings. However, the abnormal ECG findings do show that the day treatment population may be a group at risk, either for disorders associated with chest pain and shortness of breath or for taking excess doses of medication and compromising the ECG in that manner. The ECG cost (for performance and interpretation) at HCMC is $172; this would be a cost effective test if it were to prevent any significant adverse cardiovascular outcomes.
The proportion of patients with ECGs performed (37 of 96) is relatively low, and the absolute number of patients with ECGs performed (37) is small. Thus, our data must be viewed with caution in terms of extrapolating to larger populations. In a sense, they define a case series of patients in a day treatment program with unanticipated ECG abnormalities. We hope our study will prompt larger-scale investigations of psychiatric inpatients and outpatients to assess electrocardiographic findings and cardiac risk. Only then will we know if assessing ECGs in psychiatric patients will provide important diagnostic information.
The Medical Letter on Drugs and Therapeutics has recently written about drugs that prolong the QT interval, how women are at greater risk, and which classes of non-psychiatric medications (eg, antiarrhythmics, antibiotics, and opiates) prolong the QT interval.16 Psychiatric patients may thus be put at risk by a psychotropic medication that prolongs the QT interval and then may receive other medications (quinolones or opiates) or develop electrolyte abnormalities (hypokalemia and hypomagnesemia) that prolong it further. Gupta and colleagues17 discuss mechanisms of drug-related QT prolongation, and note key risk factors to take into account when prescribing such medications: female sex, structural heart disease, hypokalemia, multiple QT-prolonging drugs or drugs that interfere with their metabolism, higher drug doses, prolonged baseline QTc, a family history of long QT syndrome or sudden death, and prior history of drug-related torsades de pointes. Gupta et al also note that liver disease, bradycardia, and atrioventricular block can further increase the risk. Finally, Gupta et al state that patients should be counseled about these risks. Abdelmawla and Mitchell18 discuss sudden cardiac death and antipsychotics and make the case for monitoring and prevention. They suggest that clinicians need to be able to read the ECG and assess the risk for prescribing psychotropic medications. Our findings in Table 1 show that conduction disorders, including a widened QRS and prolonged QTc, are relatively common findings and should be taken into account when prescribing medications.
Table 1 also shows the presence of prior MI in several patients. This prevalence is striking given the young age of the majority of patients. Future studies from our group aim to focus on disturbances in the metabolic environment that might, along with smoking, substance use, and lack of attention to diet and exercise, predispose our patients to premature cardiovascular disease.
Table 2 shows that antidepressant use was very common (85% of patients) in the abnormal ECG group and found in only 50% of the normal ECG group. This finding was of borderline statistical significance (P = .07). Older studies looking at antidepressant use, the ECG, and cardiac risk in psychiatric patients19,20 have demonstrated cardiac effects during overdoses, with lesser effects seen during usual outpatient treatment. Recently, some selective serotonin reuptake inhibitor medications have received warnings about QT prolongation in high doses.21 Larger studies that assess the risk of newer antidepressants will be welcome to determine if they have more cardiac risk than previously demonstrated. Opiate use was somewhat more common in our abnormal ECG group versus the larger untested group (55% vs 19%). Whether this defines a higher risk category also remains to be determined. Additional consideration should be given to the possibility that medication use and association with ECG findings may be an epiphenomenon wherein the diagnosis for which the medication is prescribed (eg, depression) is linked with underlying heart disease, rather than the medication causing or unmasking it.
While the absolute prolongation of the QTc intervals in our patients was not excessively long (ie, only 1 patient had a QTc longer than 500 ms), Beach and colleagues21 make 2 points about QTc intervals and psychotropic medications that are relevant in this regard. First, there is a diurnal variation in QTc that can be as wide as 75–100 ms; thus, modest prolongations at baseline may be quite a bit higher 12 hours later. Second, the risk of serious arrhythmias such as torsades de pointes, for some medications, may not be correlated with the duration of the QTc. This may be due to the fact that some drugs prolong the QTc in a heterogeneous manner (some myocardial areas being affected more than others) and, in these circumstances, the results are more proarrhythmic.
Pincus and colleagues22 discuss quality measures for the long-term care of psychiatric patients. Their first quality measure (safety) concerns use of medications that affect the metabolic environment. Other proposed measures include effectiveness of systems of care (eg, patient registries and depression screening), patient-centered care (patient experience), timeliness (eg, for chemical dependence treatment), and equity (with respect to disparities in care). The metrics of Pincus et al dovetail well with our findings: the psychiatric patient is at risk, and standardized systems of care, including cardiovascular assessment and monitoring, will very likely be needed to promote long-term safety. Likewise, Zareba and Lin23 propose ongoing monitoring for psychiatric patients with prolonged QTc intervals (> 0.45 sec), with repeated ECGs after first dose of an antipsychotic drug and close monitoring of potassium and magnesium levels. Glassman and Bigger24 propose baseline ECGs in older patients, especially those with underlying cardiac disease or those taking drugs known to prolong the QT interval.
We urge others who care for psychiatric outpatients to be cognizant of cardiac risk in this population, and we encourage larger-scale studies to better define the degree of risk and the best systems of care to attenuate it.
Author affiliations: Department of Medicine (Drs Linzer, Coffey, and Shroff and Ms Poplau), Center for Healthcare Innovation (Ms Clifford), Analytic Center of Excellence (Ms Baker), Department of Performance Measurement and Improvement (Ms Baum), and Office of the Medical Director (Dr Yoder), Hennepin County Medical Center, and the Department of Medicine (Drs Linzer, Coffey, and Shroff), University of Minnesota, Minneapolis.
Potential conflicts of interest: None reported.
Funding/support: This project was supported by a grant from UCare, Minneapolis, Minnesota.
Additional information: The Clarity database is owned by Epic (Verona, Wisconsin) and housed at the Hennepin County Medical Center. Questions about the database should be directed to Dr Linzer.
REFERENCES
1. Felker B, Yazel JJ, Short D. Mortality and medical comorbidity among psychiatric patients: a review. Psychiatr Serv. 1996;47(12):1356–1363. PubMed
2. Colton CW, Manderscheid RW. Congruencies in increased mortality rates, years of potential life lost, and causes of death among public mental health clients in eight states. Prev Chronic Dis. 2006;3(2):A42. PubMed
3. Laursen TM, Munk-Olsen T, Nordentoft M, et al. Increased mortality among patients admitted with major psychiatric disorders: a register-based study comparing mortality in unipolar depressive disorder, bipolar affective disorder, schizoaffective disorder, and schizophrenia. J Clin Psychiatry. 2007;68(6):899–907. doi:10.4088/JCP.v68n0612 PubMed
4. Black DW. Iowa Record-Linkage Study: death rates in psychiatric patients. J Affect Disord. 1998;50(2–3):277–282. doi:10.1016/S0165-0327(98)00019-6 PubMed
5. Alexander CS, Niño A. Cardiovascular complications in young patients taking psychotropic drugs: a preliminary report. Am Heart J. 1969;78(6):757–769. doi:10.1016/0002-8703(69)90442-6 PubMed
6. Wahlbeck K, Westman J, Nordentoft M, et al. Outcomes of Nordic mental health systems: life expectancy of patients with mental disorders. Br J Psychiatry. 2011;199(6):453–458. doi:10.1192/bjp.bp.110.085100 PubMed
7. Thornicroft G. Physical health disparities and mental illness: the scandal of premature mortality. Br J Psychiatry. 2011;199(6):441–442. doi:10.1192/bjp.bp.111.092718 PubMed
8. Alakeson V, Frank RG, Katz RE. Specialty care medical homes for people with severe, persistent mental disorders. Health Aff (Millwood). 2010;29(5):867–873. doi:10.1377/hlthaff.2010.0080 PubMed
9. Manu P, Correll CU, van Winkel R, et al. Prediabetes in patients treated with antipsychotic drugs. J Clin Psychiatry. 2012;73(4):460–466. doi:10.4088/JCP.10m06822 PubMed
10. Mackin P, Young AH. QTc measurement and metabolic parameters in psychiatric patients taking typical or atypical antipsychotic drugs: a preliminary study. J Clin Psychiatry. 2005;66(11):1386–1391. doi:10.4088/JCP.v66n1107 PubMed
11. Hollister LE. Electrocardiographic screening in psychiatric patients. J Clin Psychiatry. 1995;56(1):26–29. PubMed
12. Jeeva Raj MV, Benson R. Phenothiazines and the electrocardiogram. Postgrad Med J. 1975;51(592):65–68. doi:10.1136/pgmj.51.592.65 PubMed
13. Kreger BE, Anderson KM, Kannel WB. Prevalence of intraventricular block in the general population: the Framingham Study. Am Heart J. 1989;117:903–910. doi:10.1016/0002-8703(89)90630-3 PubMed
14. Schwartz PJ, Stramba-Badiale M, Crotti L, et al. Prevalence of the congenital long-QT syndrome. Circulation. 2009;120(18):1761–1767. doi:10.1161/CIRCULATIONAHA.109.863209 PubMed
15. Levine E, Rosero SZ, Budzikowski AS, et al. Congenital long QT syndrome: considerations for primary care physicians. Cleve Clin J Med. 2008;75(8):591–600. doi:10.3949/ccjm.75.8.591 PubMed
16. Quetiapine (Seroquel) and QT-interval prolongation. Med Lett Drugs Ther. 2011;53(1374):79–80. PubMed
17. Gupta A, Lawrence AT, Krishnan K, et al. Current concepts in the mechanisms and management of drug-induced QT prolongation and torsade de pointes. Am Heart J. 2007;153(6):891–899. doi:10.1016/j.ahj.2007.01.040 PubMed
18. Abdelmawla N, Mitchell AJ. Sudden cardiac death and antipsychotics. part 2: monitoring and prevention. Adv Psychiatr Treat. 2006;12(2):100–109. doi:10.1192/apt.12.2.100
19. Burrows GD, Vohra J, Hunt D, et al. Cardiac effects of different tricyclic antidepressant drugs. Br J Psychiatry. 1976;129(4):335–341. doi:10.1192/bjp.129.4.335 PubMed
20. Roose SP, Laghrissi-Thode F, Kennedy JS, et al. Comparison of paroxetine and nortriptyline in depressed patients with ischemic heart disease. JAMA. 1998;279(4):287–291. doi:10.1001/jama.279.4.287 PubMed
21. Beach SR, Celano CM, Noseworthy PA, et al. QTc prolongation, torsades de pointes, and psychotropic medications. Psychosomatics. 2013;54(1):1–13. doi:10.1016/j.psym.2012.11.001 PubMed
22. Pincus HA, Spaeth-Rublee B, Watkins KE. Analysis & commentary: the case for measuring quality in mental health and substance abuse care. Health Aff (Millwood). 2011;30(4):730–736. doi:10.1377/hlthaff.2011.0268 PubMed
23. Zareba W, Lin DA. Antipsychotic drugs and QT interval prolongation. Psychiatr Q. 2003;74(3):291–306. doi:10.1023/A:1024122706337 PubMed
24. Glassman AH, Bigger JT Jr. Antipsychotic drugs: prolonged QTc interval, torsade de pointes, and sudden death. Am J Psychiatry. 2001;158(11):1774–1782. doi:10.1176/appi.ajp.158.11.1774 PubMed
Download Premium PDF
Enjoy this premium PDF as part of your membership benefits!


