To the Editor: Depression is highly prevalent in patients with cancer (10.8%–24%) and among cancer survivors (13.7%) as well.1 Rates of depression in cancer patients are thought to be up to 3 times higher than in the general population. Variations in reported rates might be a factor of site of primary cancer (eg, highest in pancreatic and lung cancers), age (eg, children are no more depressed than healthy controls), sex (eg, females are 2–3 times more likely to experience depression), and metastases with cancer pain.2
Depression in cancer patients is typically multifactorial: adjustment to diagnosis, neurotoxicity and immune reactions, mass effects, or iatrogenic (chemo/radiotherapy). Depression in these patients is underrecognized and undertreated. Depression in patients with cancer has been strongly tied to a poorer quality of life, compromised clinical outcomes, and higher mortality rates (39%),3 hence the need for outright treatment.
Multiple case series and case reports suggest the effectiveness of tricyclic antidepressants and selective serotonin reuptake inhibitors in a range of cancers; however, only a small number of randomized controlled trials have been conducted. In the same vein, mirtazapine, an atypical antidepressant designated a noradrenergic-specific serotonergic antidepressant with a unique mode of action (Table 1), was shown to be effective in treating depression in patients with cancer in a systematic review.4 It has a half-life of 20–40 hours, and food does not affect absorption. The usual dose range is 15–45 mg/d. Mirtazapine is also available commercially in an orally disintegrating tablet form, which could be user friendly for terminal patients or those with neurogenic dysphagia or swallowing difficulties.
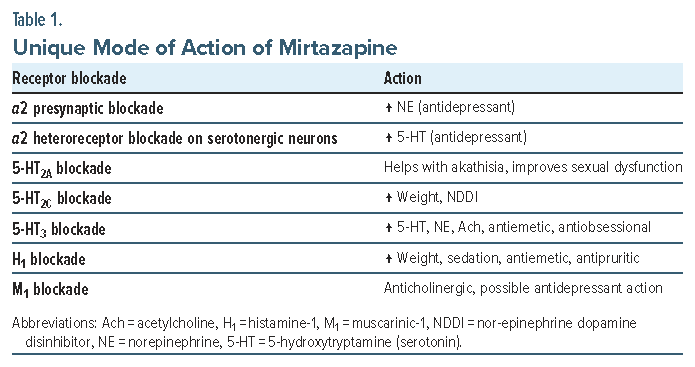
Mirtazapine (7.5–45 mg/d) helped not only with depression and anxiety, as measured by the Hospital Anxiety and Depression Scale, but also with somatic symptoms and overall quality of life. It treated insomnia (via H1 blockade) and helped with anorexia/ cachexia (via 5-hydroxytryptamine [5-HT2c] and H1 antagonism). Of note, lower doses tend to be more soporific.5
Due to antiemetic actions, via 5-HT3 and H1 antagonism, mirtazapine has been demonstrated to help with chemotherapy-induced emesis.6 Moreover, it has shown to improve gastric emptying.
Importantly, mirtazapine has minimal pharmacokinetic drug-drug interactions—a priority for patients on chemotherapy. Mirtazapine does not significantly affect cytochrome P450 (CYP) isoenzymes. It is a substrate for CYP2D6, CYP3A4, and possibly CYP1A2. Of note, mirtazapine-induced neutropenia has been reported. Other less common side effects include transaminitis, hyperlipidemia, myoclonus, and orthostasis.
A modicum of evidence speaks to the idea of antinociceptive/analgesic actions of mirtazapine, which could be advantageous in patients with cancer.7 As the habenula is reported to be involved in the emotion/reward-related pain and hypoalgesia, mirtazapine could attenuate pain and/or augment hypoalgesia by blocking the habenular α2 receptor after intermittent cold stress in mice.8 Other mechanisms at play involve facilitating analgesia by enhancing central monoaminergic neurotransmission (5-HT and norepinephrine), facilitating descending pain modulation system by decreasing afferent input in spinothalamic tracts, and central skeletal muscle relaxant actions by depressing polysynaptic reflexes causing muscle spasm/tension.9,10
Interestingly, preclinical evidence in animals exists suggesting mirtazapine can suppress tumor growth11 via immune response and the serotonergic system. The suppressive effects include increasing secretion of tumor necrosis factor (TNF)-ƴ and infiltration of CD4+ and CD8+. Furthermore, antimetastatic activity through enhanced Lin-7C/β-catenin pathway activation has been demonstrated for mirtazapine.12 It also increases levels of TNF-α, which play an important role in carcinostasis.
“Chemo brain” or chemotherapy-induced cognitive dysfunction is quite ubiquitous in patients with cancer, and inflammatory cytokines are thought to be causative. Mirtazapine, possibly through 5-HT3 antagonism, sounds procognitive.13 It has been shown to possess antioxidative and neuroprotective actions in cisplatin-induced neurotoxic rodent model. It has been demonstrated to exert astrocyte-mediated dopaminergic neuroprotection.14 Long-term use of mirtazapine has a stimulatory effect on antioxidant enzyme mRNA level expression in peripheral monocytes.15
Article Information
Published Online: June 24, 2025. https://doi.org/10.4088/PCC.25lr03918
© 2025 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2025;27(3):25lr03918
To Cite: Naguy A. Onco-psychopharmacology: is mirtazapine a catholicon? Prim Care Companion CNS Disord 2025;27(3):25lr03918.
Author Affiliation: Kuwait Centre for Mental Health, Shuwaikh, Kuwait; Priory East Midlands, Nottinghamshire, United Kingdom (Naguy).
Corresponding Author: Ahmed Naguy, MBBch, MSc, MRCPsych (UK), Kuwait Centre for Mental Health, Jamal Abdul-Nassir St, Shuwaikh, Sulibikhat 21315, Kuwait ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
References (15)

- Naser AY, Hameed AN, Mustafa N, et al. Depression and anxiety in patients with cancer: a cross-sectional study. Front Psychol. 2021; 12:585534. PubMed CrossRef
- Radhakrishnan R, Selvaraj H, Chidambaram K, et al. Prevalence of depression and anxiety disorders among cancer patients: an insight from a single institute. Cureus. 2023;15(8):e42831. PubMed CrossRef
- Pinquart M, Duberstein PR. Depression and cancer mortality: a meta-analysis. Psychol Med. 2010;40(11):1797-1810. PubMed CrossRef
- Economos G, Lovell N, Johnston A, et al. What is the evidence for mirtazapine in treating cancer-related symptomatology? A systematic review. Support Care Cancer. 2020;28(4):1597-1606. PubMed CrossRef
- Kim SW, Shin IS, Kim JM, et al. Effectiveness of mirtazapine for nausea and insomnia in cancer patients with depression. Psychiatry Clin Neurosci. 2008;62(1):75–83. PubMed CrossRef
- Kinomura M, Iihara H, Fujii H, et al. Effect of mirtazapine for the prevention of nausea and vomiting in patients with thoracic cancer receiving platinum-based chemotherapy. Anticancer Res. 2023;43(3):1301-1307. PubMed CrossRef
- Schreiber S, Rigai T, Katz Y, et al. The antinociceptive effect of mirtazapine in mice is mediated through serotonergic, noradrenergic and opioid mechanisms. Brain Res Bull. 2002;58(6):601–605. PubMed CrossRef
- Neyama H, Dozono N, Uchida H, et al. Mirtazapine, an α 2 antagonist-type antidepressant, reverses pain and lack of morphine analgesia in fibromyalgia-like mouse models. J Pharmacol Exp Ther. 2020;375(1):1-9. PubMed CrossRef
- Naguy A, Alamiri B. Antidepressants- a misnomer? Clinical impressionism or scientific empiricism? Prim Care Companion CNS Disord. 2022;24(3):21br03084. PubMed CrossRef
- Naguy A. Milnacipran for postcoital cephalgia and premature ejaculation. Am J Ther. 2019;26(5):e662-e664. PubMed CrossRef
- Fang C-K, Chen H-W, Chiang I-T, et al. Mirtazapine inhibits tumor growth via immune response and serotonergic system. PLoS One. 2012;7(7):e38886. PubMed CrossRef
- Uzawa K, Kasamatsu A, Shimizu T, et al. Suppression of metastasis by mirtazapine via restoration of the Lin-7C/β-catenin pathway in human cancer cells. Sci Rep. 2014;4:5433. PubMed CrossRef
- Moodliar S, Naguy A, Elsori DH. Add-on mirtazapine to clozapine-responsive early-onset schizophrenia. Psychiatry Res. 2020;284:112701. PubMed CrossRef
- Gulec M, Oral E, Dursun OB, et al. Mirtazapine protects against cisplatin-induced oxidative stress and DNA damage in the rat brain. Psychiatry Clin Neurosci. 2013;67(1):50–58. PubMed CrossRef
- Das A, Ranadive N, Kinra M, et al. An overview on chemotherapy-induced cognitive impairment and potential role of antidepressants. Curr Neuropharmacol. 2020;18(9):838-851. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!