Catatonia is a high-morbidity syndrome present in nearly 10% of psychiatric inpatients.1,2 In this article, we argue that increasing the rate of empiric treatment of suspected catatonia and preferentially erring on the side of administering catatonia-specific treatment when uncertain could lead to better outcomes.
From a risk-benefit perspective, prioritizing the identification and management of catatonia is prudent because of catatonia’s potential harm and in view of the effective, well-tolerated treatments available. However, swift catatonia management is hindered by clinical underrecognition, among other factors.
With catatonia’s undertreatment in mind, we discuss historical approaches to clinical decision-making and then introduce a decision-making matrix that incorporates expected risks and treatment benefits into management decisions. (Note: We use the term treatment in this article to refer to initiating catatonia-specific management, especially lorazepam or electroconvulsive therapy [ECT], though we recognize that catatonia’s sequelae and associated conditions [eg, major depression or schizophrenia] may be treated even in the absence of catatonia-specific management.)
Establishing Catatonia as a High Morbidity, Underrecognized, and Undertreated Entity
Catatonia can cause medical harm via several mechanisms, including poor oral intake leading to sequelae across organ systems, poor self-care, and malignant catatonia. This latter entity causes mortality in approximately 10% of cases, ranging as high as 30%–50% in untreated or improperly treated patients.3–7
Despite its grave potential harms, catatonia remains undertreated in many settings.8,9 Factors contributing to undertreatment include underdiagnosis, clinician discomfort with medication doses needed for clinical response, and unavailability of specific treatments, eg, ECT, in some settings.10
Regarding underdiagnosis, catatonia has a heterogeneous presentation with many different presenting signs, rendering it inherently challenging to recognize consistently.1 Additionally, catatonia can be missed due to its overlap with other syndromes, including delirium, psychosis, trauma-related disorders, volitional behavior, dissociation, and neuroleptic malignant syndrome.11 Catatonia can also present secondary to many other medical conditions, medications themselves, or medication withdrawal.12 The waxing and waning nature of catatonia’s clinical presentation—ranging from stupor to overexcitement—can also introduce diagnostic complications, leading to interrater unreliability and treatment interruptions.13 Catatonia rating scales have attempted to correct these interrater challenges with good effect.14
Aside from challenges inherent to diagnosis, catatonia treatment can also be hampered by clinician skepticism or unawareness, particularly in nonpsychiatric settings.1,10 Additionally, the unusually high doses of benzodiazepines sometimes required for optimal treatment of catatonia can unnerve clinicians, leading to undertreatment.15 Structurally, intravenous benzodiazepines and ECT, 2 of the mainstays of catatonia treatment, are unavailable in some settings. Finally, patient refusal of offered interventions can contribute to undertreatment.
Why Treatment of Catatonia Should Be Prioritized
Among the illnesses arising in psychiatric care settings, only a small number, such as GABAergic withdrawal, refeeding syndrome, and uncommon medication side effects (eg, serotonin syndrome, agranulocytosis, Stevens-Johnson syndrome), pose as high or higher acute medical risk than catatonia. These other high-risk conditions are typically swiftly managed, either in a psychiatric care setting or via medical transfer, even when diagnosis is not certain, to prevent potential lethality. We argue that similar risk-benefit logic should be applied to catatonia management: rather than undertreatment or hesitancy, urgency should be the default due to catatonia’s potential lethality. Additionally, because the gold standard for initial catatonia management, the “lorazepam challenge,” can both diagnose and treat, reflexive initial management is even more prudent.13
Medical Decision-Making Through Clinical Uncertainty: The Literature
Catatonia, as a high-risk yet apparently undertreated syndrome, is an interesting case study in medical decision-making. Much has been written about how clinicians make decisions, particularly regarding the difficult tasks of synthesizing large amounts of data, assessing risk versus benefit of treatment decisions, and determining an appropriate “therapeutic threshold” at which the probability of having a condition makes treatment appropriate.16
A method for quasimathematically balancing the individual “costs and benefits” of medical treatment was proposed in 1975 by Pauker and Kassirer.17 A later model explored the axes of “importance” and “certainty” inherent to medical decisions.18 Personal factors in decision-making, including recency and implicit biases, have also received attention.19 Recent literature has explored the complicated role of uncertainty in diagnosis and decision-making.20,21
Why Does Articulating How to Make Treatment Decisions Matter for Psychiatry?
Decision-making models can aid medical practice broadly and may be particularly prudent in psychiatry due to the field’s reliance on intuition and pattern recognition in clinical decision-making. In psychiatry, where hard diagnostic tools are often lacking, experiential exposure to clinical phenotypes and intuition are often used to make diagnoses.22 This issue has received longstanding attention; in 1966, Gauron and Dickinson23 studied psychiatrists who struggled to articulate why they made the decisions they did, pointing to the role of clinical intuition. Using structured decisional approaches can reduce some of the risks of intuitive decision-making, such as heuristics and biases.24
A Tool for Managing Clinical Uncertainty
To illustrate why catatonia treatment is important and to help clinicians think through clinical decisions in general, we propose the following tool in Figure 1, which articulates how clinicians might make a clinical decision based on (1) the acute risk of harm from a condition (a function of the epidemiologic frequency of the condition and its inherent potential harm) and (2) the net benefit of treating the condition (a function of the potential effectiveness of treatment and the adverse event profile of treatment). Weighing the statistical concepts of type I error (ie, treating when illness is absent) and type II error (ie, not treating when illness is present), we can then consider how to preferentially “err” based on the clinical scenario. These concepts expand on ideas from Pauker and Kassirer,17 including the reality, central to psychiatry, that treatments have ambiguous and sometimes poor efficacy and that diagnosis can be capricious and uncertain. This particular matrix composition borrows from the risk management literature and offers insight into how to make clinical decisions when diagnosis is uncertain but some factors are known.25
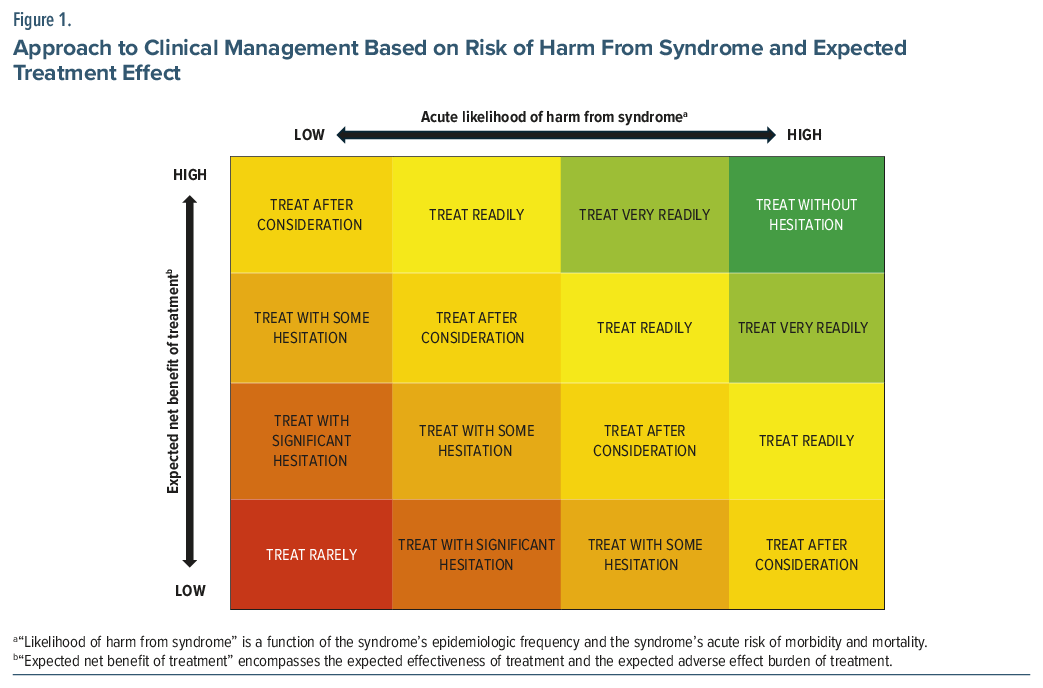
In Figure 1, catatonia and other high-morbidity conditions with highly effective treatments would be “green,” ie, should be prioritized in treatment even if diagnosis is uncertain. In “green” cases, type I error (treating unnecessarily) is preferred, as type II error (failing to treat real illness) carries severe consequences.
By the same logic, another common entity in psychiatry, alcohol withdrawal, is also “green”; due to the increased acknowledgment of the serious risks of withdrawal, prompt empiric treatment with benzodiazepines is the standard of care. Benzodiazepine treatment for alcohol withdrawal is highly effective in preventing the morbidity and mortality of withdrawal and is well-tolerated, and the risks of not treating true withdrawal are very high. We argue that catatonia should be approached similarly.
A variable that interacts with this framework is diagnostic uncertainty; in cases of total or near-total diagnostic certainty, the suspected entity should, of course, be treated first. However, when significant diagnostic uncertainty exists and various entities remain on a differential, clinicians should still prioritize an early empiric treatment trial for “green” conditions on the differential, given their risk profile and potential to resolve with safe, effective treatments. For example, if a patient presents with waxing and waning mutism, staring, and posturing, we believe that it should be standard practice to give empiric catatonia treatment even when diagnosis is not certain because of catatonia’s high acute risk of harm. In practice, this would mean that catatonia diagnosis should supersede other items on the differential, such as trauma-related disorders with dissociative features, that lack highly and rapidly effective treatment.
Detailed discussion of “yellow,” “orange,” or “red” conditions in this figure is largely beyond the scope of this article. In general, “yellow” entities might include major depressive disorder and schizophrenia, syndromes that are generally less imminently morbid and for which reasonably efficacious treatments exist. Importantly, however, the acute risk of these diagnoses is not fixed and may vary substantially across clinical presentations. When patients exhibit features such as suicidal ideation, violent ideation, and command auditory hallucinations, the urgency of intervention increases markedly. In these situations, the acute symptoms themselves should be conceptualized as “green” conditions, warranting prompt treatment regardless of the underlying diagnosis.
By contrast, when such high-risk features are absent, the overall acute medical risk of “yellow” or “orange” conditions is lower than that of “green” conditions such as catatonia, GABAergic withdrawal, or refeeding syndrome. Accordingly, “yellow” conditions should be treated less reflexively than “green” conditions, as clinicians have more time to consider the differential and gather more data. Conditions with high imminent risk but ineffective treatments (“yellow-orange,” bottom right of this figure) are fortunately uncommon in psychiatry; examples might include Huntington disease or prion disease, fatal illnesses for which all available treatments should certainly be tried but for which no effective primary treatments currently exist. Finally, “red” conditions include those with low acute risk of harm and low net benefit treatments, such as malingering and factitious disorder, for which treatment is often ineffective and sometimes harmful.
Conclusion
Catatonia is a high-risk, often undertreated syndrome that can serve as a case study for psychiatric decision-making in the presence of diagnostic uncertainty. Catatonia is undertreated for many reasons including underrecognition, diagnostic difficulty, overlap with other diagnoses, and concerns about treatment risks. Building on ideas from prior decision-making models, we propose a tool for making treatment decisions in uncertain scenarios, emphasizing deliberate consideration of inherent risks and treatment effectiveness and encouraging clinicians to prioritize action when effective, low-risk treatment exists for high-morbidity conditions like catatonia. With this tool, we hope clinicians may feel more confident approaching uncertain clinical circumstances, ultimately benefiting the patients we serve.
Article Information
Published Online: April 20, 2026. https://doi.org/10.4088/JCP.26ac16389
© 2026 Physicians Postgraduate Press, Inc.
J Clin Psychiatry 2026;87(3):26ac16389
To Cite: MacLean RL, Stoklosa JB. Catatonia as a case study in psychiatric decision-making. J Clin Psychiatry. 2026;87(3):26ac16389.
Author Affiliations: McLean Hospital, Belmont, Massachusetts (MacLean, Stoklosa); Department of Psychiatry, Mass General Brigham, Boston, Massachusetts (MacLean, Stoklosa); Harvard Medical School, Boston, Massachusetts (MacLean, Stoklosa).
Corresponding Author: Rachel L. MacLean, MD, McLean Hospital, 115 Mill Street, Mailstop #105, Belmont, MA 02478 ([email protected])
Author Contributions: Contributed to the conception of the paper: (MacLean, Stoklosa); conducted a literature search: (MacLean); wrote the first manuscript draft: (MacLean); created the figure: (MacLean, Stoklosa); edited the manuscript: (MacLean, Stoklosa).
Financial Disclosure: None.
Funding/Support: None.
![]() The ASCP Corner, edited by Leslie L. Citrome, MD, MPH, is a collection of brief peer-reviewed, evidence-based articles, authored by American Society of Clinical Psychopharmacology members, that examine the practice of psychopharmacology through the lens of clinical experience. The information contained herein only represents the opinion of the author(s). See more ASCP Corner Articles at Psychiatrist.com/ASCP-Corner
The ASCP Corner, edited by Leslie L. Citrome, MD, MPH, is a collection of brief peer-reviewed, evidence-based articles, authored by American Society of Clinical Psychopharmacology members, that examine the practice of psychopharmacology through the lens of clinical experience. The information contained herein only represents the opinion of the author(s). See more ASCP Corner Articles at Psychiatrist.com/ASCP-Corner
References (25)

- Solmi M, Pigato GG, Roiter B, et al. Prevalence of Catatonia and its moderators in clinical samples: results from a meta-analysis and meta-regression analysis. Schizophr Bull. 2018;44(5):1133–1150. PubMed CrossRef
- Grover S, Chakrabarti S, Ghormode D, et al. Catatonia in inpatients with psychiatric disorders: a comparison of schizophrenia and mood disorders. Psychiatry Res. 2015;229(3):919–925. PubMed CrossRef
- Cornic F, Consoli A, Tanguy ML, et al. Association of adolescent catatonia with increased mortality and morbidity: evidence from a prospective follow-up study. Schizophr Res. 2009;113(2–3):233–240. PubMed CrossRef
- Mann SC, Caroff SN, Bleier HR, et al. Lethal catatonia. Am J Psychiatry. 1986;143(11):1374–1381. PubMed CrossRef
- Pelzer AC, van der Heijden FM, den Boer E. Systematic review of catatonia treatment. Neuropsychiatr Dis Treat. 2018;14:317–326. PubMed CrossRef
- Rogers JP, Oldham MA, Fricchione G, et al. Evidence-based consensus guidelines for the management of catatonia: recommendations from the British Association for Psychopharmacology. J Psychopharmacol Oxf Engl. 2023;37(4):327–369. PubMed CrossRef
- Singerman B, Raheja R. Malignant catatonia-a continuing reality. Ann Clin Psychiatry Off J Am Acad Clin Psychiatr. 1994;6(4):259–266. PubMed CrossRef
- Hirjak D, Rogers JP, Wolf RC, et al. Catatonia. Nat Rev Dis Primer. 2024;10(1):49. PubMed CrossRef
- Fink M. Catatonia: a syndrome appears, disappears, and is rediscovered. Can J Psychiatry Rev Can Psychiatr. 2009;54(7):437–445. PubMed CrossRef
- van der Heijden FMMA, Tuinier S, Arts NJM, et al. Catatonia: disappeared or under-diagnosed?. Psychopathology. 2005;38(1):3–8. PubMed CrossRef
- Lang FU, Lang S, Becker T, et al. Neuroleptic malignant syndrome or catatonia? Trying to solve the catatonic dilemma. Psychopharmacol Berl. January 2015;232(1):1–5. PubMed CrossRef
- Connell J, Oldham M, Pandharipande P, et al. Malignant catatonia: a review for the intensivist. J Intensive Care Med. 2023;38(2):137–150. PubMed CrossRef
- Edinoff AN, Kaufman SE, Hollier JW, et al. Catatonia: clinical overview of the diagnosis, treatment, and clinical challenges. Neurol Int. 2021;13(4):570–586. PubMed CrossRef
- Bush G, Fink M, Petrides G, et al. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129–136. PubMed CrossRef
- Sienaert P, Dhossche DM, Vancampfort D, et al. A clinical review of the treatment of catatonia. Front Psychiatry. 2014;5:181. PubMed CrossRef
- Therapeutic decision making: a cost-benefit analysis | New Engl J Med [Internet]. [cited 2025 Oct 29]. Available from: https://www.nejm.org/doi/full/10.1056/NEJM197507312930505
- Pauker SG, Kassirer JP. Therapeutic decision making: a cost-benefit analysis. N Engl J Med. 1975;293(5):229–234. PubMed CrossRef
- Whitney SN. A new model of medical decisions: exploring the limits of shared decision making. Med Decis Mak. 2003 Jul 1;23(4):275–280. PubMed CrossRef
- McKinlay JB, Potter DA, Feldman HA. Non-medical influences on medical decision-making. Soc Sci Med. 1996 Mar 1;42(5):769–776. PubMed CrossRef
- Masic I. Medical decision making - an overview. Acta Inf Medica. 2022;30(3):230–235. PubMed CrossRef
- Helou MA, DiazGranados D, Ryan MS, et al. Uncertainty in decision making in medicine: a scoping review and thematic analysis of conceptual models. Acad Med J Assoc Am Med Coll. 2020;95(1):157–165. PubMed CrossRef
- Bhugra D, Easter A, Mallaris Y, et al. Clinical decision making in psychiatry by psychiatrists. Acta Psychiatr Scand. 2011;124(5):403–411. PubMed CrossRef
- Gauron EF, Dickinson JK. Diagnostic decision making in psychiatry: I. Information usage. Arch Gen Psychiatry. 1966;14(3):225–232. PubMed CrossRef
- Hall KH. Reviewing intuitive decision-making and uncertainty: the implications for medical education. Med Educ. 2002;36(3):216–224. PubMed CrossRef
- Pascarella G, Rossi M, Montella E, et al. Risk analysis in healthcare organizations: methodological framework and critical variables. Risk Manag Healthc Pol. 2021;14:2897–2911. PubMed CrossRef
This PDF is free for all visitors!