To the Editor: Catatonia is a psychomotor condition increasingly recognized for its prevalence and growing visibility in clinical practice and national guidelines.1 Although most commonly considered a psychiatric diagnosis, 25% of cases of catatonia are estimated to occur secondary to medical conditions.2 Catatonia frequently overlaps with delirium, underscoring its complex and incompletely elucidated pathophysiology. Both occur in the setting of medical illness and are strongly influenced by underlying neurological vulnerability.2 Because such vulnerability appears to increase the risk of these conditions, major neurocognitive disorder (MNCD) may likewise predispose patients to catatonia. As catatonia is not only life-threatening but also physically debilitating, its occurrence in a medically and cognitively frail patient could signal poor prognosis. Yet the prognostic significance of catatonia remains understudied, particularly in end-of-life contexts. In this letter, we present a combined cohort of 4 patients with baseline neurocognitive disorders who developed catatonia shortly before death.
Methods
We conducted a chart review of 4 patients evaluated by the consultation-liaison psychiatry service.
Results
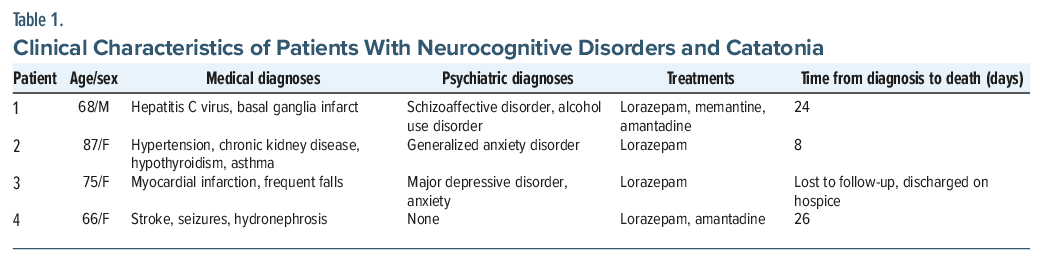
All patients had MNCD, diagnosed either before or at the time of consultation. Ages ranged from 68–87 years (mean: 74 years). Three (75%) had additional psychiatric comorbidities: 1 with major depressive disorder and anxiety, 1 with generalized anxiety disorder, and 1 with alcohol use disorder and schizoaffective disorder. Two had a history of stroke. Clinical demographics of the patients are listed in further detail in Table 1.
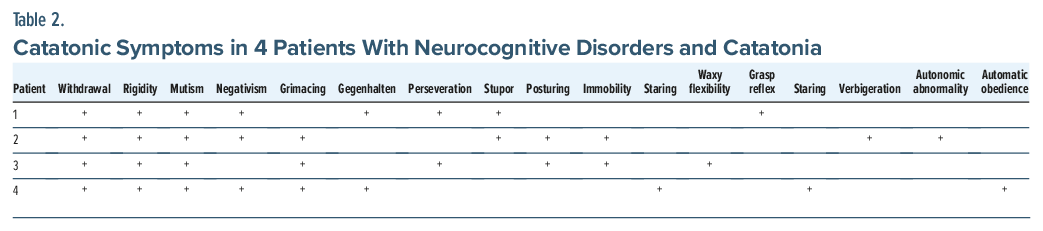
All patients exhibited withdrawal, rigidity, and mutism; 3 also demonstrated negativism and grimacing (Table 2). The average number of catatonic signs over the course of admission was 8.75. Each received lorazepam; 2 required augmentation with memantine alone or with amantadine due to partial response. Although the Bush-Francis Catatonia Rating Scale (BFCRS)3 was not uniformly performed, all patients demonstrated partial clinical improvement. Electroconvulsive therapy (ECT) was unavailable. Most died within 1 month of diagnosis (mean: 19.3 days).
Discussion
We describe 4 patients with MNCD who developed catatonia shortly before death. Despite some improvement with lorazepam and adjunctive agents, all experienced rapid decline, with death within a mean of 19.3 days. This raises key questions: Does catatonia in MNCD mark transition to the final stages of life? and How should this inform goals-of-care discussions?
The consistent pattern—withdrawal, mutism, rigidity—followed by decline suggests that catatonia may serve as a prognostic clue in advanced MNCD. Recognizing this may prompt palliative care involvement, especially as catatonic symptoms complicate decisions about artificial nutrition, hydration, and other life-prolonging measures.4 The limited response to lorazepam suggests that catatonia in MNCD may follow a distinct therapeutic course, underscoring the need for research on treatment strategies tailored to MNCD-associated catatonia. This pattern also aligns with findings that catatonia in medical settings often presents with more catatonic signs than the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition or BFCRS thresholds, suggesting that “medical” catatonia may differ from “psychiatric” catatonia and may require adjusted diagnostic thresholds in populations with high rates of delirium.5
ECT, the first-line “silver bullet” for severe catatonia, was unavailable, highlighting a broader systems issue. While ECT is known to offer symptom relief, little has been written about its role in values-based decision-making in end-stage illness. Growing interest in “palliative ECT” calls for investigation into when ECT may be lifesaving versus burdensome near life’s end.6 This case series highlights the need for research at the intersection of catatonia, MNCD, and dying to guide care that is both medically appropriate and aligned with patient goals and values.
Article Information
Published Online: April 28, 2026. https://doi.org/10.4088/PCC.25lr04150
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25lr04150
To Cite: Prognostic implications of catatonia in end-of-life care for patients with advanced neurocognitive disorder. Prim Care Companion CNS Disord. 2026;28(2):25lr04150.
Author Affiliations: Department of Psychiatry, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania (Coulter); Departments of Family and Preventive Medicine, Medicine, and Psychiatry and Behavioral Sciences, Emory University School of Medicine and Grady Memorial Hospital, Atlanta, Georgia (Robbins-Welty).
Corresponding Author: Andrew M. Coulter, MD, MA, Department of Psychiatry, University of Pittsburgh School of Medicine, Pittsburgh, Pennsylvania ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Additional Information: All patient information has been de-identified.
Acknowledgement: https://www.thecatatoniafoundation.org/resources-catatonia-ingeneral.
References (6)

- Oldham MA. Catatonia: the Phoenix rises again and is here to stay. J Acad Consult Liaison Psychiatry. 2025;66(2):115–117. PubMed CrossRef
- Coid F, Rogers JP, Saini A, et al. Taking an evidence-based approach to ten common myths about catatonia: an educational review. J Acad Consult Liaison Psychiatry. 2025;66(4):358–368. PubMed CrossRef
- Bush G, Fink M, Petrides G, et al. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129–136. PubMed CrossRef
- Zingela Z, Stroud L, Cronje J, et al. The psychological and subjective experience of catatonia: a qualitative study. BMC Psychol. 2022;10(1):173. PubMed CrossRef
- Mormando C, Reinfeld S, Gnova N, et al. Catatonia and delirium in a general medical setting: prevalence and naturalistic treatment outcome. J Acad Consult Liaison Psychiatry. 2025. doi:10. 1016/j.jaclp.2025.10.334. CrossRef
- Robbins-Welty GA, Slauer RD, Brown MM, et al. Palliative electroconvulsive therapy: a descriptive cohort study. J Acad Consult Liaison Psychiatry. 2024; 66(3):215–223. PubMed CrossRef
Please sign in or purchase this PDF for $40.