The combination of bipolar disorder and obsessive-compulsive symptoms remains one of the most challenging clinical presentations in psychiatry.1–3 Standard treatments frequently fail or worsen mood instability: high-dose selective serotonin reuptake inhibitors (SSRIs) carry a substantial risk of manic switch, while mood stabilizers alone rarely touch the obsessions.4,5 Intravenous ketamine can produce rapid relief of both mood and intrusive thoughts,6,7 but cost, monitoring requirements, and transient dissociation limit its everyday use.
Case Report
Three consecutive adults (2 women aged 24 and 31 years and 1 man aged 46 years) seen in outpatient practice in Hong Kong between May and November 2025 presented with DSM-5 bipolar disorder (2 bipolar I, 1 bipolar II) and severe, mood-congruent obsessive-compulsive features—trichotillomania with onychophagia, persistent bladder-emptying ruminations with checking, and compulsive arranging accompanied by somatic delusions. All had failed multiple prior trials of high-dose SSRIs/serotonin-norepinephrine reuptake inhibitors, atypical antipsychotics, and standard mood stabilizers.
Each patient was started on an oral ketamine-mimetic protocol (the Cheung Glutamatergic Regimen)8 consisting of dextromethorphan (NMDA receptor antagonism, typically 30–120 mg/d), whose exposure was prolonged with low-dose fluoxetine (10–20 mg/d) as a cytochrome P450 (CYP)2D6 inhibitor and augmented with piracetam (AMPA receptor positive allosteric modulation, 600–1,200 mg/d) and, when needed, L-glutamine (500–1,000 mg/d) for presynaptic glutamate support.8 Conventional mood stabilizers and low-dose antipsychotics were continued or adjusted as clinically indicated.
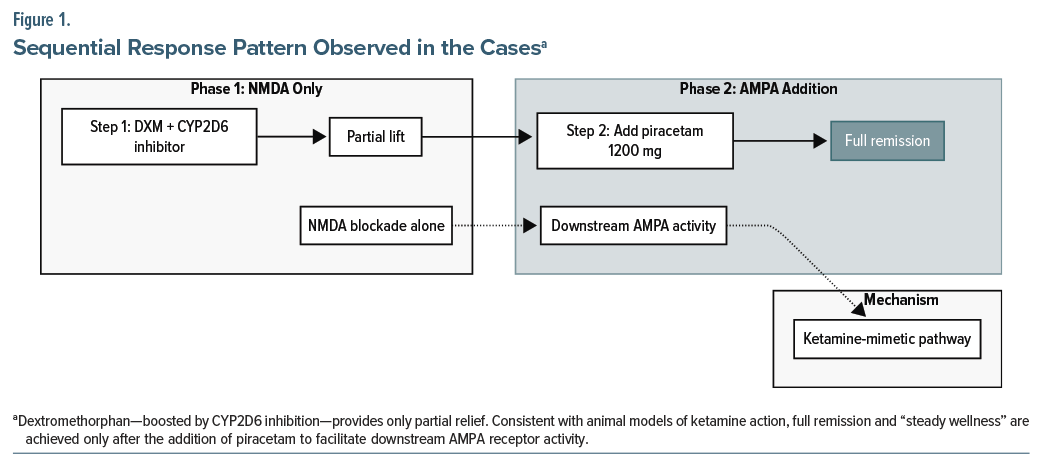
In all 3 cases, partial improvement occurred with dextromethorphan alone, but sustained remission of both depressive and anxious symptoms and obsessive-compulsive phenomena only followed the addition of piracetam (Figure 1). Transient hypomanic activation, when it occurred, was managed by reducing dextromethorphan dose while maintaining or increasing piracetam, alongside adequate mood stabilization.9 By late November 2025, scores on the Patient Health Questionnaire-9 (PHQ-9) scores had fallen markedly from baseline values of 14–27 to final values of 6–9, and Generalized Anxiety Disorder 7-item (GAD-7) scores had fallen from baseline values of 15–19 to final values of 6–9, and specific compulsive behaviors had largely resolved. Treatment was generally well tolerated; no serious adverse events were recorded.
Discussion
These naturalistic observations in routine care suggest that a fully oral, inexpensive NMDA–AMPA modulation strategy may offer a practical alternative for patients with the “bipolar obsessive-compulsive disorder” phenotype who respond poorly to conventional approaches.10,11 The consistent “second-step” effect of piracetam aligns with preclinical and clinical data indicating that downstream AMPA receptor activation is critical for the sustained antidepressant and antiobsessive actions of ketamine-like agents.12,13
Controlled trials are now needed to confirm efficacy, establish optimal dosing, and clarify long-term safety in this difficult-to-treat subgroup.
Article Information
Published Online: February 23, 2026. https://doi.org/10.4088/JCP.25cr16262
© 2026 Physicians Postgraduate Press, Inc.
J Clin Psychiatry 2026;87(2):25cr16262
Submitted: December 10, 2025; accepted January 20, 2026.
To Cite: Cheung N. Oral glutamatergic modulation with dextromethorphan and piracetam for refractory bipolar disorder with obsessive-compulsive disorder: three consecutive cases from routine practice. J Clin Psychiatry 2026;87(2):25cr16262.
Author Affiliation: Cheung Ngo Medical Limited, Hong Kong SAR, China.
Corresponding Author: Ngo Cheung, MBBS, FHKAM(Psychiatry), Cheung Ngo Medical Limited, Hong Kong SAR, China ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: This work received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Patient Consent: Consent was received from the 3 patients to publish the anonymized case report.
References (13)

- Amerio A, Stubbs B, Odone A, et al. The prevalence and predictors of comorbid bipolar disorder and obsessive-compulsive disorder: a systematic review and meta-analysis. J Affect Disord. 2015;186:99–109. PubMed CrossRef
- Amerio A, Stubbs B, Odone A, et al. Bipolar I and II disorders: a systematic review and meta-analysis on differences in comorbid obsessive-compulsive disorder. Iran J Psychiatry Behav Sci. 2016;10(3):e3604. PubMed CrossRef
- Ferentinos P, Preti A, Veroniki AA, et al. Comorbidity of obsessive-compulsive disorder in bipolar spectrum disorders: systematic review and meta-analysis of its prevalence. J Affect Disord. 2020;263:193–208. PubMed CrossRef
- De Prisco M, Tapoi C, Oliva V, et al. Clinical features in co-occurring obsessive-compulsive disorder and bipolar disorder: a systematic review and meta-analysis. Eur Neuropsychopharmacol. 2024;80:14–24. PubMed CrossRef
- de Filippis R, Aguglia A, Costanza A, et al. Obsessive-compulsive disorder as an epiphenomenon of comorbid bipolar disorder? An updated systematic review. J Clin Med. 2024;13(5):1230. PubMed CrossRef
- Berman RM, Cappiello A, Anand A, et al. Antidepressant effects of ketamine in depressed patients. Biol Psychiatry. 2000;47(4):351–354. PubMed CrossRef
- Zarate CA Jr, Brutsche NE, Ibrahim L, et al. Replication of ketamine’s antidepressant efficacy in bipolar depression: a randomized controlled add-on trial. Biol Psychiatry. 2012;71(11):939–946. PubMed CrossRef
- Cheung N. DXM, CYP2D6-inhibiting antidepressants, piracetam, and glutamine: proposing a ketamine-class antidepressant regimen with existing drugs.Preprints.org. Preprint posted online November 25, 2025. https://www.preprints.org/manuscript/202511.1815
- Cheung N. Clinical experience and optimisation of the Cheung glutamatergic regimen for refractory psychiatric diseases. Preprints.org. Preprint posted online November 28, 2025. https://www.preprints.org/manuscript/202511.2246
- Cheung N. Case series: marked improvement in treatment-resistant obsessive–compulsive symptoms with over-the-counter glutamatergic augmentation in routine clinical practice. Preprints.org. Preprint posted online November 28, 2025. https://www.preprints.org/manuscript/202511.2223
- Cheung N. Oral glutamatergic augmentation for trauma-related disorders with fluoxetine-/ bupropion-potentiated dextromethorphan ± piracetam: a four-patient case series. Preprints.org. Preprint posted online November 24, 2025. https://www.preprints.org/manuscript/202511.1788
- Maeng S, Zarate CA Jr, Du J, et al. Cellular mechanisms underlying the antidepressant effects of ketamine: role of AMPA receptors. Biol Psychiatry. 2008;63(4):349–352. PubMed CrossRef
- Zanos P, Moaddel R, Morris PJ, et al. NMDAR inhibition-independent antidepressant actions of ketamine metabolites. Nature. 2016;533(7604):481–486. PubMed CrossRef
This PDF is free for all visitors!





