ABSTRACT
Objective: To evaluate the effects of lurasidone on social functioning in schizophrenia over the course of a 6-week, double-blind, placebo-controlled study and a subsequent 12-week open-label extension study.
Methods: A total of 478 patients with schizophrenia (per DSM-IV-TR criteria) randomized to either lurasidone 40 mg/d (n = 245) or placebo (n = 233) in the initial 6-week double-blind study (initiated May 2016, completed November 2018) were included in the analysis. Longer-term changes were examined in a sample of 146 patients who received lurasidone, and 141 who received placebo, during the 6-week study and received flexibly dosed (40–80 mg/d) lurasidone during the 12-week extension phase. The 4-item Positive and Negative Syndrome Scale (PANSS) prosocial subscale was used to examine changes in social functioning.
Results: At week 6 of the double-blind phase, lurasidone-treated patients had significantly greater improvement on the PANSS prosocial subscale compared to placebo-treated patients (P < .01, effect size at week 6 = 0.33). Significant differences from placebo were also evident at week 2 (P < .05), week 4 (P < .001), and week 5 (P < .01). Across the 12-week extension phase, patients who received lurasidone during both the 6-week double-blind phase and the 12-week open-label phase continued to show successive decreases in scores on the 4-item PANSS prosocial subscale (score change of –3.0 from double-blind baseline to week 6; mean score change of −4.2 from double-blind baseline to week 12 of the extension phase).
Conclusions: In patients with schizophrenia treated with lurasidone, social functioning improved relative to placebo during a 6-week double-blind study and continued to improve over the course of 12 weeks of extension treatment with lurasidone. Effects of lurasidone on social functioning appear to be comparable to what has been reported for other atypical antipsychotics.
Trial Registration: EudraCT Numbers: 2016-000060-42 and 2016-000061-23
J Clin Psychiatry 2024;85(1):23m14881
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Individuals with schizophrenia present with a range of symptoms that include positive symptoms such as delusions and hallucinations and negative symptoms such as apathy. In addition, depressive symptoms and cognitive deficits in working memory, executive function, and processing speed are often apparent.1,2 Across 65 studies, the median lifetime prevalence of schizophrenia has been estimated to be 0.48% (interquartile range, 0.26%–0.51%).3 This translates into over 20 million people worldwide with the disorder.4 Due to the early onset and chronicity of schizophrenia, together with impairment in functioning across a range of domains, the economic burden of schizophrenia is enormous, with an estimated impact in the range from 0.02% to 1.65% of the gross domestic product across various countries.5
Deficits in social functioning associated with schizophrenia are present from the early stage of the disorder and tend to persist over time.6,7 Impairment in social functioning has been found to be more pronounced for patients with longer illness durations.8,9 The range of deficits in social functioning for individuals with schizophrenia include difficulty coping with social situations, social withdrawal, and, often, social isolation. The impairments in social functioning found in schizophrenia are critical to understanding the disorder and therefore are part of common scales used to assess symptoms in schizophrenia. These impairments in social functioning include a focus on asociality with items measuring social behavior and also reduced interest and motivation for social interaction.10 The degree of impairment in social functioning in those with schizophrenia has been found to be associated with the extent to which personal recovery is achieved in such individuals.11,12 For these reasons, improving social functioning is an important clinical outcome for patients with schizophrenia.
Lurasidone is a second-generation antipsychotic agent that received regulatory approval for the treatment of schizophrenia in the US for adults (in 2010) and adolescents (in 2017). It also is approved for the treatment of schizophrenia in multiple countries, including countries in the European Union, Switzerland, Canada, Australia, and Japan. Lurasidone acts as an antagonist for dopamine D2, serotonin-7 (5-HT7), and 5-HT2A receptors and as a partial agonist for 5-HT1A receptors, with minimal binding affinity for histamine H1 and muscarinic M1 receptors.13 The short- and long-term efficacy and safety of lurasidone (40–160 mg/d) in adults and adolescents (aged 13–17; 40–80 mg/d) has been demonstrated in multiple clinical trials.14–20 In placebo-controlled trials enrolling patients with schizophrenia, minimal effects of lurasidone on body weight and metabolic parameters have been demonstrated.14,19
Despite the body of evidence on the efficacy of lurasidone, little attention has been given to the effects of this agent on social functioning among patients with schizophrenia. One randomized 6-week study that enrolled non-medicated patients with schizophrenia21 reported no significant difference between lurasidone and olanzapine on improvement in social functioning. Enrolling patients with treatment-resistant schizophrenia, a small study22 randomized patients to 24 weeks of 80 or 240 mg/d of lurasidone following a 6-week open trial of lurasidone 80 mg/d and found that social functioning was significantly improved in both treatment groups beginning at week 12 of the 24-week randomized phase 2. No placebo-controlled studies of lurasidone in the treatment of schizophrenia have specifically examined change in social functioning. In the treatment of bipolar depression, a pooled study analysis23 revealed that lurasidone significantly improved social relationships compared to placebo, with a moderately large Cohen d effect size of 0.55.
Lurasidone may improve social functioning through its impact on cognitive variables. Research suggests that cognitive ability and social cognition predict social functioning both cross-sectionally and longitudinally among individuals with schizophrenia.24–26 These findings, taken together with data indicating that lurasidone has been found to improve cognitive functioning and social cognition in patients with schizophrenia,27,28 suggest a possible mechanism for lurasidone’s improving social functioning through improvement of cognitive functioning and social cognition.
The aim of the current study was to evaluate the effect of lurasidone on social functioning in schizophrenia using the data from a 6-week, randomized, double-blind study15 and the 12-week open-label phase of the study.20
METHODS
Study Design and Participants
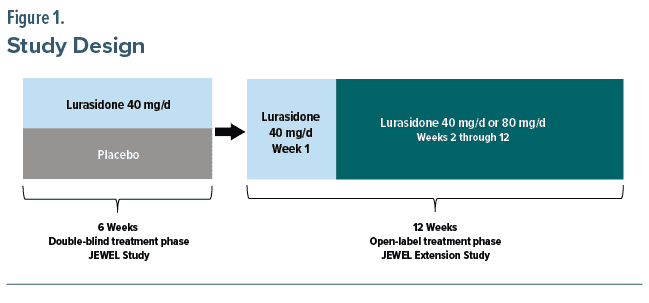
The present analysis uses data from a multicenter, randomized, double-blind, placebo-controlled, parallel-group 6-week study (JEWEL study; EudraCT number: 2016-000060-42; study initiated May 2016 and completed November 2018)15 and the subsequent pre-planned 12-week open-label extension study (clinical trial registration: EudraCT number: 2016-000061-23).20 The initial 6-week study evaluated the efficacy and safety of lurasidone 40 mg/d for patients with acute schizophrenia. Patients for the 6-week study were recruited at 73 clinical sites in 5 countries (Japan, Ukraine, Russia, Romania, Poland). In the extension study, patients who completed the short-term double-blind study were treated with flexibly dosed 40 or 80 mg/d of open-label lurasidone for an additional 12 weeks. The overall design of the double-blind phase followed by the extension phase is presented in Figure 1.
The 6-week study and the subsequent 12-week extension phase were conducted in accordance with the International Conference on Harmonization Guideline for Good Clinical Practice and the Declaration of Helsinki. The protocols were approved by the Ethics Committee at each participating center. Written informed consent was obtained from each patient following an explanation of study procedures.
Patients (aged 18–74 years) eligible for the 6-week study received a diagnosis of schizophrenia based on the Mini-International Neuropsychiatric Interview (MINI)29 6.0.0 using the Diagnostic and Statistical Manual of Mental Disorders, Fourth Edition, Text Revision (DSM-IV-TR)30 criteria; a Positive and Negative Syndrome Scale (PANSS)31 total score ≥ 80; a PANSS item score ≥ 4 (moderate) on 2 or more certain PANSS items (delusions, conceptual disorganization, hallucinations, suspiciousness, or unusual thought content) at both screening and baseline; and a score of 4 (moderately ill) or higher on the Clinical Global Impressions–Severity of Illness scale (CGI-S)32 at screening and baseline. Key exclusion criteria for the 6-week trial included continuous hospitalization for > 3 months (90 days) immediately prior to screening, continuous hospitalization for > 14 days for acute exacerbation of psychotic symptoms immediately prior to screening in patients who had been treated continuously with adequate doses of at least 1 antipsychotic agent for ≥ 4 weeks immediately prior to screening, and a decrease of ≥ 20% in the PANSS total score between screening and baseline visits. Additional selection details are given in the article describing the 6-week study.15
Eligibility for the 12-week extension phase study included completion of the 6-week double-blind study and completion of all assessments on the final acute study visit. Excluded from the extension phase were patients deemed to be at an imminent risk of suicide or injury to self or others or who answered “yes” to item 4 (active suicidal ideation with some intent to act, without specific plan) or item 5 (active suicidal ideation with specific plan and intent) on the Columbia-Suicide Severity Rating Scale (C-SSRS)33 at the baseline visit of the extension phase. Additional extension phase exclusions included evidence of severe tardive dyskinesia, severe dystonia, or other severe movement disorder or need for treatment with any potent cytochrome P450 (CYP) 3A4 inhibitors or inducers.
Randomization and Masking During Double-Blind Study
For the 6-week trial, randomization was implemented (1:1 ratio of drug to placebo) at baseline using an Interactive Voice/Web Response System (IXRS). Patients, investigators, and all research staff were unaware of the identity of the treatment group assignment from the time of randomization until database lock and unblinding. Lurasidone and placebo were identical in packaging, labeling, schedule of administration, and appearance during the double-blind trial.
Drug Administration
For the 6-week double-blind study, tablets containing either lurasidone 40 mg/d or placebo were administered once daily (orally) in the evening, with food or within 30 minutes after eating. During the 12-week extension phase, open-label lurasidone 40 mg/d was administered during the first week, followed by flexible dosing of lurasidone up to 80 mg/d. Dosing adjustments at each subsequent visit were then allowed.
Concomitant Medications
During the initial 6-week double-blind trial, use of antipsychotics, antidepressants, mood stabilizers, and other psychotropics was discontinued. During the extension phase, antidepressant medications (except fluvoxamine) and/or mood stabilizers (except carbamazepine and oxcarbazepine) could be initiated. Benztropine (≤ 6 mg/d) was prescribed as needed during both the 6-week double-blind phase and 12-week extension phase for the management of treatment-emergent movement disorders. If inadequate response or intolerability to benztropine treatment occurred, use of biperiden, trihexyphenidyl, diphenhydramine, or promethazine was permitted. Treatment with propranolol (≤ 120 mg/d) was allowed for akathisia. During both the 6-week trial and extension phase, concomitant use of lorazepam, zolpidem, temazepam, brotizolam, triazolam, lormetazepam, zopiclone, or eszopiclone was permitted. Prohibited during the extension phase were fluoxetine, monoamine oxidase inhibitors, additional antipsychotic medications, electroconvulsive therapy, herbal supplements (for psychotropic reasons), and antiarrhythmic drugs of Class 1A or of Class 3.
Assessment of Social Functioning
Assessment of social functioning was derived from the PANSS. The PANSS consists of subscales measuring negative symptoms (N), positive symptoms (P), and general psychopathology (G). However, a 4-item PANSS prosocial subscale has also been developed.34,35 The 4-item PANSS prosocial subscale was a modification of a previous 6-item scale36 that retained the active social avoidance (G16), passive social withdrawal (N4), and emotional withdrawal (N2) items from the 6-item subscale and added difficulty in abstract thinking (N5). The 4 items were chosen based on analyses that suggested these items captured social functioning changes for an antipsychotic (aripiprazole) that was perceived by psychiatrists to have unique beneficial effects on interpersonal functioning compared to other antipsychotics (haloperidol, risperidone, ziprasidone, olanzapine, clozapine, and quetiapine).34 The 4-item PANSS prosocial subscale has been found to be sensitive to change in double-blind trials that found significantly greater improvements for aripiprazole compared to placebo and for aripiprazole compared to haloperidol, and change over time in an open-label non-controlled 16-week study of brexpiprazole, in the treatment of schizophrenia.35,37,38 No available studies have examined the association between the 4-item PANSS subscale score and other measures of social functioning. However, one study calculated a PANSS “experience” scale consisting of the active social avoidance, passive social withdrawal, and emotional withdrawal items and found this scale significantly predicted interpersonal functioning (r = 0.46), but other negative symptoms failed to contribute significantly to the prediction of interpersonal functioning.39
The PANSS prosocial subscale score is a sum of the 4 items. In addition to the prosocial subscale, we examined all individual N, P, and G PANSS items to see how change in prosocial subscale items compared with change in other items. Trained raters implemented the PANSS using the standard item anchoring from absent (1) to extreme (7). The PANSS was administered at double-blind study baseline and weekly during the 6-week trial, and at open-label baseline and weeks 1, 2, 4, 8, and 12 during the 12-week extension study. Internal consistency (Cronbach α) on the 4-item prosocial scale total score was 0.59 using data from baseline of the double-blind phase and was 0.70 using data from the open-label baseline in the current study.
Statistics
The population for the analysis of changes in social functioning during the 6-week double-blind phase was defined as patients who received at least one dose of study drug and had at least one post-baseline PANSS assessment that yielded a total score. The population for examination of social functioning changes during the extension phase was defined as all patients treated with lurasidone who completed the double-blind phase, entered the extension phase, and had at least one post–open-label PANSS assessment that yielded a total score during the extension phase.
Scores on the PANSS prosocial subscale measure were analyzed using a mixed effects model for repeated measures (MMRM), with fixed factors of pooled study center, visit (week 1, 2, 3, 4, 5, and 6; as a categorical variable), treatment (lurasidone and placebo), and treatment-by-visit interaction and baseline PANSS prosocial subscale score as a covariate. A specific contrast was included in the model to evaluate changes at week 6. An unstructured covariance matrix was used for the within-subject correlation. The Kenward-Roger approximation was used to calculate the denominator degrees of freedom. Cohen d effect sizes were calculated as the absolute least squares mean difference at week 6 divided by the model estimate of standard deviation. Additional mixed models examined change from double-blind baseline to each weekly assessment and change from double-blind baseline to week 6 for all PANSS items. No imputation of missing data was conducted for significance testing on changes in prosocial functioning during the double-blind phase.
For examination of changes during the extension phase, only descriptive statistics were used to summarize social functioning changes given that there was no random assignment to placebo during that phase. We calculated mean change from double-blind baseline to each assessment conducted during the open-label phase, and to endpoint (last observation carried forward [LOCF]) during that phase. Analyses were conducted using SAS Version 9.4 or later.
RESULTS
Participant Disposition and Characteristics
A total of 483 patients were randomized to lurasidone 40 mg/d (n = 247) or placebo (n = 236) in the initial 6-week double-blind study. Of these, there were 375 patients (lurasidone, n = 199; placebo, n = 176) who completed the 6-week study, with 289 of these enrolling in the subsequent 12-week open-label extension phase (148 from lurasidone 40 mg/d and 141 from placebo during the 6-week trial). Two patients assigned to lurasidone and 2 assigned to placebo during the 6-week double-blind phase did not have post-baseline assessments, plus 1 patient (assigned to placebo) did not take any study medication, leaving 478 patients included in analyses of social functioning changes during the initial 6 weeks. Two patients enrolled in the extension phase did not have post–open-label baseline assessments (both treated with lurasidone 40 mg/d in the 6-week study) and were excluded from the analysis of changes in scores on the PANSS prosocial subscale during the 12-week open-label phase. The remaining 146 patients who received lurasidone during both the double-blind and open-label phases, and 141 who received placebo during the double-blind phase and open-label flexibly dosed lurasidone during the extension phase, were examined for social functioning changes over the course of the extension phase.
Of the 146 patients who received 40 mg/d of lurasidone during the fixed-dose 6-week phase, 72 received modal 40 mg/d and 74 received modal 80 mg/d during the extension phase. Of the 141 patients who received placebo during the 6-week double-blind phase, 79 received modal 40 mg/d and 62 received modal 80 mg/d of lurasidone during the extension phase. Overall, the median duration of study drug exposure was 84 days during the extension phase.
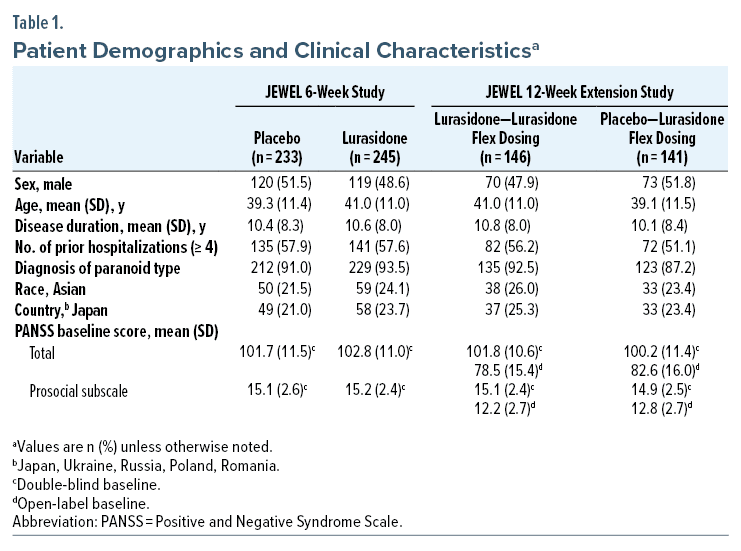
The demographic and clinical characteristics of the analysis sample for the 6-week study were generally similar for those who received lurasidone compared to placebo. The sample analyzed for the extension phase was also similar to those enrolled during the 6-week phase (Table 1). For the sample as a whole, there were similar proportions of men and women, with a mean age of about 40 years.
Social Functioning Outcomes
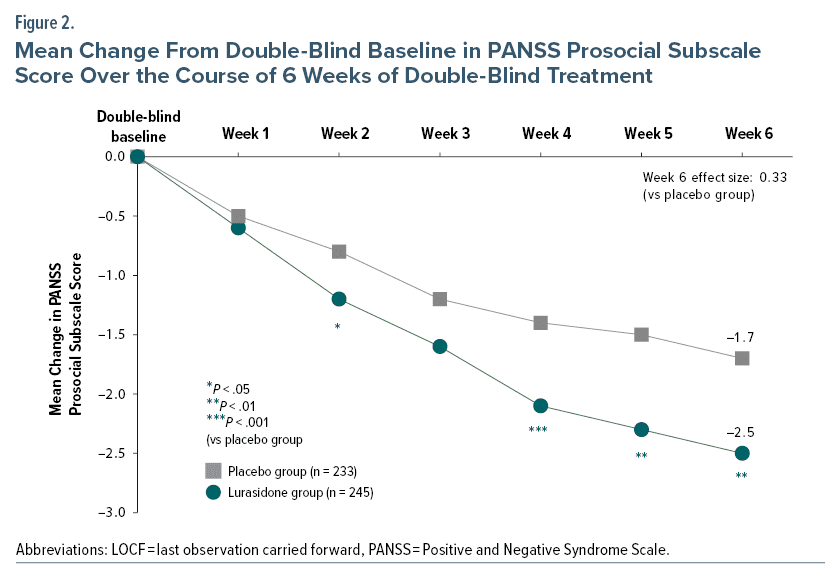
At week 6 of the double-blind phase, MMRM analyses revealed lurasidone-treated patients had statistically significantly greater improvement on the 4-item PANSS prosocial subscale compared to placebo-treated patients (P < .01, Cohen d effect size at week 6 = 0.33) (Figure 2). Significant differences from placebo were evident at week 2 (P < .05, d = 0.21), week 4 (P < .001, d = 0.33), and week 5 (P < .01, d = 0.29), in addition to week 6 (Figure 2).
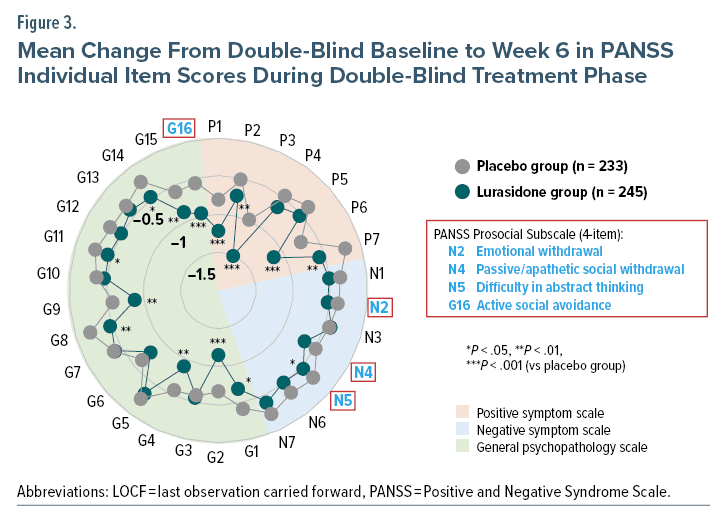
Examination of change from double-blind baseline to week 6 on the individual items in the 4-item PANSS prosocial subscale revealed statistically significant superiority of lurasidone, compared to placebo, on active social avoidance (P < .001) and difficulty in abstract thinking (P < .05). No significant differences were evident in emotional withdrawal or passive/apathetic social withdrawal (Figure 3). Of note is that the amount of mean difference between lurasidone and placebo on change from double-blind baseline to week 6 on the active social avoidance item was numerically surpassed by only 4 other PANSS items: delusions (P1), hallucinatory behavior (P3), suspiciousness/persecution (P6), and anxiety (G2).
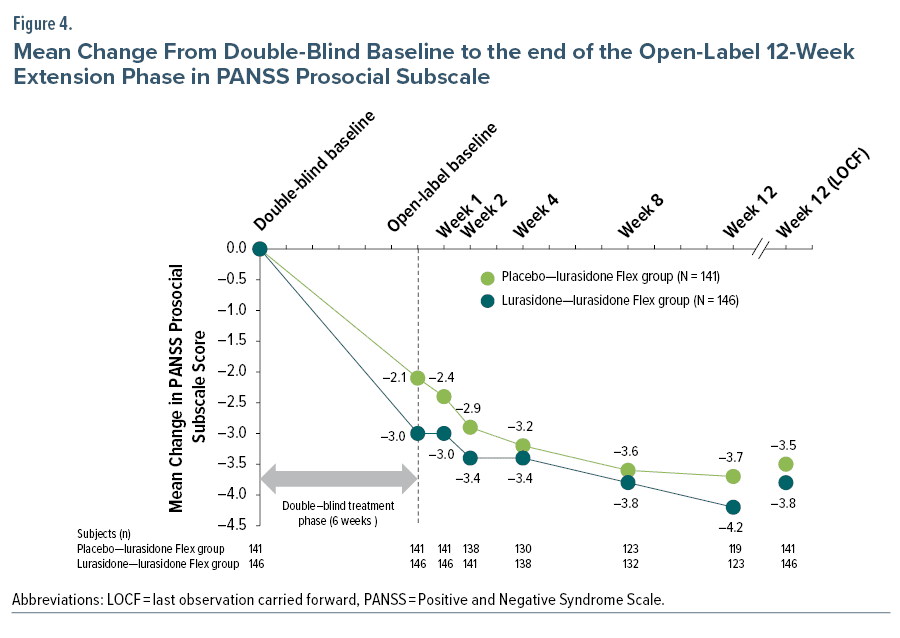
Across the 12-week extension phase, patients who received lurasidone during both the 6-week double-blind phase and the 12-week open-label phase continued to show successive decreases in scores on the 4-item PANSS prosocial subscale (Figure 4). Change from double-blind baseline to week 6 was −3.0 scale points for lurasidone-treated patients, improving to a −3.8 mean change from double-blind baseline to week 12 (LOCF) of the extension phase (26.7% further mean improvement from the end of double-blind phase, n = 146). For patients who received placebo during the double-blind phase, the mean change during the double-blind phase was −2.1 scale points, improving to a −3.5 mean change from double-blind baseline to week 12 (LOCF) of the extension phase (66.7% further mean improvement from the end of the double-blind phase, n = 141) (Figure 4).
DISCUSSION
The current study is the first to document the effects of lurasidone compared to placebo on social functioning in the treatment of schizophrenia using the PANSS prosocial subscale. During a 6-week double-blind trial, lurasidone 40 mg/d had greater improvements compared to placebo on social function beginning at week 2. The overall drug versus placebo effect size at week 6 (0.33) was very similar to that found (0.34) in a meta-analysis of 10 placebo-controlled short-term studies evaluating the effects of other antipsychotic drugs on social functioning.40 Given this similarity in effect sizes, it is unlikely that the effects of lurasidone on social functioning are greater than such effects for other antipsychotics in the treatment of schizophrenia. However, more head-to-head comparisons of lurasidone to other antipsychotics on improvements in social functioning, beyond the existing study comparing lurasidone and olanzapine,21 are needed to directly evaluate any potential differences among antipsychotics on this outcome. Though modest in size, the effect size found here for changes in social functioning for lurasidone compared to placebo is clinically meaningful when considered in the context of the chronic and disabling nature of schizophrenia and the importance of social functioning to long-term recovery from the illness.
The effects of lurasidone on social functioning during the 6-week trial were driven primarily by an impact on the active social avoidance item that showed considerably larger changes than were evident on the other 3 items on the 4-item PANSS prosocial subscale. In fact, no statistically significant drug-placebo differences were found on the emotional withdrawal and passive/apathetic social withdrawal items. The relative size of the effect on the active social avoidance item was evident in the fact that only 4 items on the PANSS (P1, P3, P6, and G2) displayed numerically larger drug-placebo differences than that found for the active social avoidance item. These results suggest that active social avoidance is responsive to treatment with lurasidone and is a critical aspect of the overall therapeutic effects of lurasidone in the treatment of schizophrenia. Considering the early deficits in social functioning associated with schizophrenia, and the relation of such deficits to the degree of achievement in personal recovery, improvement in social functioning should be a high priority in the clinical management of individuals with this disorder.6,11,12
Noteworthy was the fact that improvements in social functioning continued through the open-label extension phase. The 26.7% additional mean change evident over the course of the 12-week open-label phase is particularly important because deficits in social functioning have been found to be highly persistent among those with schizophrenia over time periods as long as 20 years.41 In the CATIE study,42 improvement from baseline to 12 months in interpersonal relationships following antipsychotic treatment was very modest, with no differences seen among first and second generation antipsychotic agents. A study directly comparing lurasidone to other antipsychotics would be needed to evaluate whether the longer-term changes in social functioning seen here exceed those evident with other treatment approaches.
Although the mechanism through which lurasidone improves social functioning is not known, one possibility for the mechanism, as mentioned in the Introduction, is the intervening role of changes in cognitive ability. In animal models of learning, memory, and cognitive ability, lurasidone has been found to significantly improve response rates.43–45 Consistent with these animal studies, both cognitive functioning and social cognition have been found to improve across treatment in patients with schizophrenia treated with lurasidone.27,28 This procognitive effect of lurasidone is thought to be a function of the blockade of serotonin receptors 5-HT7 and 5-HT1A.46 The 5-HT7 receptors are expressed mainly in brain regions (ie, thalamus, hypothalamus, hippocampus, cortex) involved in the regulation of memory, learning, and cognition.47 These procognitive and prosocial effects are not unique to lurasidone, as other antipsychotics have also been found to exert such effects to different degrees.48,49 However, the effect of some antipsychotics on cognition is complicated and confounded by their association with metabolic syndrome that can in turn negatively impact cognitive functioning over time.48 Lurasidone has not been associated with metabolic syndrome.50 Given that better cognition and social functioning have been linked with long-term recovery in those with schizophrenia, use of a pharmacologic agent that leads to improvements in these domains is an important clinical consideration.
Limitations
Several limitations of this study should be noted. First, the analyses were post hoc and therefore await confirmation in prospective trials. A second limitation is that extension phase treatment was open-label, with no placebo or active comparator control group. A third limitation is that social functioning was assessed using a PANSS subscale rather than a scale developed more specifically to measure social impairment. The validity of the PANSS prosocial scale in relation to other measures of social functioning is not well-established, and the PANSS prosocial scale is not among those listed in a compilation of standard rating scales for measuring social functioning.51 The importance of using well-validated scales that are sensitive to change in treatment studies of schizophrenia has been emphasized previously.52 The advantage, however, of the PANSS prosocial subscale is that the PANSS is used in most treatment studies of schizophrenia, and therefore the extent to which the current findings are evident with other pharmacologic agents can readily be investigated in post hoc analyses. A fourth limitation is that the generalizability of the results to other dosages of lurasidone is not known. A final limitation of the current study is that the generalizability of the results to other types of patients, and other durations of treatment, is not known because the study population consisted of patients who met specific inclusion and exclusion criteria and the duration of evaluation of the extension phase was only 12 weeks.
CONCLUSION
In conclusion, among patients with an acute exacerbation of schizophrenia, lurasidone (40 mg/d) improves social functioning more than placebo over the course of 6 weeks of double-blind treatment, and such improvements continue during an additional 12 weeks of ongoing open-label flexible dose (40–80 mg/d) lurasidone treatment.
Article Information
Published Online: January 31, 2024. https://doi.org/10.4088/JCP.23m14881
© 2024 Physicians Postgraduate Press, Inc.
Submitted: March 25, 2023; accepted October 20, 2023.
To Cite: Miura I, Sano F, Sakaguchi R, et al. Effect of lurasidone on social functioning in schizophrenia: post hoc analysis of the JEWEL study. J Clin Psychiatry. 2024;85(1):23m14881.
Author Affiliations: Department of Neuropsychiatry, Fukushima Medical University, Fukushima, Japan (Miura); Department of Data Science, Drug Development Division, Sumitomo Pharma Co., Ltd., Tokyo, Japan (Sano); Department of Clinical Research, Drug Development Division, Sumitomo Pharma Co., Ltd., Tokyo, Japan (Sakaguchi); Department of Clinical Operation, Drug Development Division, Sumitomo Pharma Co., Ltd., Tokyo, Japan (Okamoto); Medical Science, Sumitomo Pharma Co., Ltd., Tokyo, Japan (Maruyama).
Corresponding Author: Itaru Miura, MD, PhD, 1 Hikarigaoka, Fukushima 960-1295, Japan ([email protected]).
Relevant Financial Relationships: Dr Miura reports personal fees from Sumitomo Pharma Co., Ltd. Drs Sakaguchi, Okamoto, Sano, and Maruyama are employees of Sumitomo Pharma.
Funding/Support: This work was funded by Sumitomo Pharma Co., Ltd. Medical writing assistance was provided by Edward Schweizer, MD, of Paladin Consulting Group, Inc. (Concord, MA) and funded by Sumitomo Pharma Co., Ltd.
Role of the Funders/Sponsors: Sumitomo Pharma Co., Ltd participated in the design and analysis of the original studies. All authors participated in the interpretation of the data presented in the current post hoc analysis, provided critical review and edits during manuscript development, and approved the final draft for submission.
Acknowledgments: We thank the patients and providers who participated in the study. We also thank Kentaro Takai, PhD, and Katsuhiko Hagi, PhD, who are employees of Sumitomo Pharma Co., Ltd., for providing support in performing the post hoc analyses.
Clinical Points
- Improvement in social functioning is an important outcome in the treatment of schizophrenia.
- In individuals with schizophrenia, lurasidone is effective (compared to placebo) in improving social functioning during 6 weeks of treatment, with continued improvement observed during 12 weeks of open-label continuation treatment.
- Effects of lurasidone on social functioning appear to be comparable to what has been reported for other atypical antipsychotics.
References (52)

- McCutcheon RA, Reis Marques T, Howes OD. Schizophrenia-an overview. JAMA Psychiatry. 2020;77(2):201–210. PubMed CrossRef
- Kahn RS, Sommer IE, Murray RM, et al. Schizophrenia. Nat Rev Dis Primers. 2015;1(1):15067. PubMed CrossRef
- Simeone JC, Ward AJ, Rotella P, et al. An evaluation of variation in published estimates of schizophrenia prevalence from 1990─2013: a systematic literature review. BMC Psychiatry. 2015;15(1):193. PubMed CrossRef
- World Health Organization. Schizophrenia fact sheet. 2019. https://www.who.int/news-room/fact-sheets/detail/schizophrenia
- Chong HY, Teoh SL, Wu DB, et al. Global economic burden of schizophrenia: a systematic review. Neuropsychiatr Dis Treat. 2016;12:357–373. PubMed
- Grant C, Addington J, Addington D, et al. Social functioning in first- and multiepisode schizophrenia. Can J Psychiatry. 2001;46(8):746–749. PubMed CrossRef
- Wiersma D, Wanderling J, Dragomirecka E, et al. Social disability in schizophrenia: its development and prediction over 15 years in incidence cohorts in six European centres. Psychol Med. 2000;30(5):1155–1167. PubMed CrossRef
- Frascarelli M, Tognin S, Mirigliani A, et al. Medial frontal gyrus alterations in schizophrenia: relationship with duration of illness and executive dysfunction. Psychiatry Res. 2015;231(2):103–110. PubMed CrossRef
- Preston NJ. Predicting community survival in early psychosis and schizophrenia populations after receiving intensive case management. Aust N Z J Psychiatry. 2000;34(1):122–128. PubMed CrossRef
- Kirkpatrick B, Strauss GP, Nguyen L, et al. The Brief Negative Symptom Scale: psychometric properties. Schizophr Bull. 2011;37(2):300–305. PubMed CrossRef
- Drapalski AL, Medoff D, Dixon L, et al. The reliability and validity of the Maryland Assessment of Recovery in Serious Mental Illness Scale. Psychiatry Res. 2016;239:259–264. PubMed CrossRef
- Watanabe S, Taniguchi T, Sugihara M. Relationship between social function and personal recovery in patients with schizophrenia. Asian J Psychiatr. 2022;71:103078. PubMed CrossRef
- Ishibashi T, Horisawa T, Tokuda K, et al. Pharmacological profile of lurasidone, a novel antipsychotic agent with potent 5-hydroxytryptamine 7 (5-HT7) and 5-HT1A receptor activity. J Pharmacol Exp Ther. 2010;334(1):171–181. PubMed CrossRef
- Hagi K, Nosaka T, Kane J, et al. Efficacy and tolerability of lurasidone in schizophrenia: a systematic review and meta-analysis of short-term, randomized, placebo controlled trials. Eur Psychiatry. 2021;64(suppl 1):S157. CrossRef
- Iyo M, Ishigooka J, Nakamura M, et al. Efficacy and safety of lurasidone in acutely psychotic patients with schizophrenia: A 6-week, randomized, double-blind, placebo-controlled study. Psychiatry Clin Neurosci. 2021;75(7):227–235. PubMed CrossRef
- Stahl SM, Cucchiaro J, Simonelli D, et al. Effectiveness of lurasidone for patients with schizophrenia following 6 weeks of acute treatment with lurasidone, olanzapine, or placebo: a 6-month, open-label, extension study. J Clin Psychiatry. 2013;74(5):507–515. PubMed CrossRef
- Loebel A, Cucchiaro J, Xu J, et al. Effectiveness of lurasidone vs quetiapine XR for relapse prevention in schizophrenia: a 12-month, double-blind, noninferiority study. Schizophr Res. 2013;147(1):95–102. PubMed CrossRef
- Correll CU, Cucchiaro J, Silva R, et al. Long-term safety and effectiveness of lurasidone in schizophrenia: a 22-month, open-label extension study. CNS Spectr. 2016;21(5):393–402. PubMed CrossRef
- Arango C, Ng-Mak D, Finn E, et al. Lurasidone compared to other atypical antipsychotic monotherapies for adolescent schizophrenia: a systematic literature review and network meta-analysis. Eur Child Adolesc Psychiatry. 2020;29(9):1195–1205. PubMed CrossRef
- Iyo M, Ishigooka J, Nakamura M, et al. Safety and effectiveness of lurasidone in patients with schizophrenia: a 12-week, open-label extension study. Neuropsychiatr Dis Treat. 2021;17:2683–2695. PubMed CrossRef
- Jena M, Ranjan R, Mishra BR, et al. Effect of lurasidone vs olanzapine on neurotrophic biomarkers in unmedicated schizophrenia: a randomized controlled trial. J Psychiatr Res. 2019;112:1–6. PubMed CrossRef
- Meltzer HY, Share DB, Jayathilake K, et al. Lurasidone improves psychopathology and cognition in treatment-resistant schizophrenia. J Clin Psychopharmacol. 2020;40(3):240–249. PubMed CrossRef
- Dembek C, Fan Q, Niu X, et al. Impact of lurasidone on health-related quality of life in adults with bipolar depression: a post-hoc analysis. Curr Med Res Opin. 2022;38(9):1613–1619. PubMed CrossRef
- Lipkovich IA, Deberdt W, Csernansky JG, et al. Relationships among neurocognition, symptoms and functioning in patients with schizophrenia: a path-analytic approach for associations at baseline and following 24 weeks of antipsychotic drug therapy. BMC Psychiatry. 2009;9(1):44. PubMed CrossRef
- Martínez-Domínguez S, Penadés R, Segura B, et al. Influence of social cognition on daily functioning in schizophrenia: study of incremental validity and mediational effects. Psychiatry Res. 2015;225(3):374–380. PubMed CrossRef
- Cowman M, Holleran L, Lonergan E, et al. Cognitive predictors of social and occupational functioning in early psychosis: a systematic review and meta-analysis of cross-sectional and longitudinal data. Schizophr Bull. 2021;47(5):1243–1253. PubMed CrossRef
- Harvey PD, Ogasa M, Cucchiaro J, et al. Performance and interview-based assessments of cognitive change in a randomized, double-blind comparison of lurasidone vs ziprasidone. Schizophr Res. 2011;127(1–3):188–194. PubMed CrossRef
- Harvey PD, Siu CO, Hsu J, et al. Effect of lurasidone on neurocognitive performance in patients with schizophrenia: a short-term placebo- and active-controlled study followed by a 6-month double-blind extension. Eur Neuropsychopharmacol. 2013;23(11):1373–1382. PubMed CrossRef
- Sheehan DV, Lecrubier Y, Sheehan KH, et al. The Mini-International Neuropsychiatric Interview (M.I.N.I.): the development and validation of a structured diagnostic psychiatric interview for DSM-IV and ICD-10. J Clin Psychiatry. 1998;59(suppl 20):22–33, quiz 34–57. PubMed
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. Fourth Edition, Text Revision. Washington, DC: American Psychiatric Press; 2000.
- Kay SR, Fiszbein A, Opler LA. The Positive and Negative Syndrome Scale (PANSS) for schizophrenia. Schizophr Bull. 1987;13(2):261–276. PubMed CrossRef
- Guy W. ECDEU Assessment Manual for Psychopharmacology (revised). Rockville, MD: National Institute of Mental Health; 1976.
- Posner K, Brown GK, Stanley B, et al. The Columbia-Suicide Severity Rating Scale: initial validity and internal consistency findings from three multisite studies with adolescents and adults. Am J Psychiatry. 2011;168(12):1266–1277. PubMed CrossRef
- Baran X, Docherty J. 2008. The A-effect of aripiprazole. Presented at: the American Psychiatric Association meeting; May 3–8, 2008; Washington, DC.
- Docherty JP, Baker RA, Eudicone J, et al. Effect of aripiprazole versus haloperidol on PANSS Prosocial items in early-episode patients with schizophrenia. Schizophr Res. 2010;120(1-3):199–203. PubMed CrossRef
- Purnine DM, Carey KB, Maisto SA, et al. Assessing positive and negative symptoms in outpatients with schizophrenia and mood disorders. J Nerv Ment Dis. 2000;188(10):653–661. PubMed CrossRef
- Correll CU, Stanford AD, Claxton A, et al. Social and functional outcomes with two doses of aripiprazole lauroxil vs placebo in patients with schizophrenia: a post-hoc analysis of a 12-week phase 3 efficacy study. Psychiatry Res. 2019;274:176–181. PubMed CrossRef
- Malla A, Ota A, Nagamizu K, et al. The effect of brexpiprazole in adult outpatients with early-episode schizophrenia: an exploratory study. Int Clin Psychopharmacol. 2016;31(6):307–314. PubMed CrossRef
- Harvey PD, Khan A, Keefe RSE. Using the Positive and Negative Syndrome Scale (PANSS) to define different domains of negative symptoms: prediction of everyday functioning by impairments in emotional expression and emotional experience. Innov Clin Neurosci. 2017;14(11–12):18–22. PubMed
- Leucht S, Leucht C, Huhn M, et al. Sixty years of placebo-controlled antipsychotic drug trials in acute schizophrenia: systematic review, bayesian meta-analysis, and meta-regression of efficacy predictors. Am J Psychiatry. 2017;174(10):927–942. PubMed CrossRef
- Velthorst E, Fett AJ, Reichenberg A, et al. The 20-year longitudinal trajectories of social functioning in individuals with psychotic disorders. Am J Psychiatry. 2017;174(11):1075–1085. PubMed CrossRef
- Swartz MS, Perkins DO, Stroup TS, et al; CATIE Investigators. Effects of antipsychotic medications on psychosocial functioning in patients with chronic schizophrenia: findings from the NIMH CATIE study. Am J Psychiatry. 2007;164(3):428–436. PubMed CrossRef
- Ishiyama T, Tokuda K, Ishibashi T, et al. Lurasidone (SM-13496), a novel atypical antipsychotic drug, reverses MK-801-induced impairment of learning and memory in the rat passive-avoidance test. Eur J Pharmacol. 2007;572(2–3):160–170. PubMed CrossRef
- Horisawa T, Nishikawa H, Toma S, et al. The role of 5-HT7 receptor antagonism in the amelioration of MK-801-induced learning and memory deficits by the novel atypical antipsychotic drug lurasidone. Behav Brain Res. 2013;244:66–69. PubMed CrossRef
- Enomoto T, Ishibashi T, Tokuda K, et al. Lurasidone reverses MK-801-induced impairment of learning and memory in the Morris water maze and radial-arm maze tests in rats. Behav Brain Res. 2008;186(2):197–207. PubMed CrossRef
- Yasui-Furukori N. Update on the development of lurasidone as a treatment for patients with acute schizophrenia. Drug Des Devel Ther. 2012;6:107–115. PubMed CrossRef
- Martín-Cora FJ, Pazos A. Autoradiographic distribution of 5-HT7 receptors in the human brain using [3H]mesulergine: comparison to other mammalian species. Br J Pharmacol. 2004;141(1):92–104. PubMed CrossRef
- MacKenzie NE, Kowalchuk C, Agarwal SM, et al. Antipsychotics, metabolic adverse effects, and cognitive function in schizophrenia. Front Psychiatry. 2018;9:622. PubMed CrossRef
- Désaméricq G, Schurhoff F, Meary A, et al. Long-term neurocognitive effects of antipsychotics in schizophrenia: a network meta-analysis. Eur J Clin Pharmacol. 2014;70(2):127–134. PubMed CrossRef
- Pillinger T, McCutcheon RA, Vano L, et al. Comparative effects of 18 antipsychotics on metabolic function in patients with schizophrenia, predictors of metabolic dysregulation, and association with psychopathology: a systematic review and network meta-analysis. Lancet Psychiatry. 2020;7(1):64–77. PubMed CrossRef
- Leifker FR, Patterson TL, Heaton RK, et al. Validating measures of real-world outcome: the results of the VALERO expert survey and RAND panel. Schizophr Bull. 2011;37(2):334–343. PubMed CrossRef
- Brissos S, Molodynski A, Dias VV, et al. The importance of measuring psychosocial functioning in schizophrenia. Ann Gen Psychiatry. 2011;10(1):18. PubMed CrossRef
This PDF is free for all visitors!




