Abstract
Background: The attitudes of clinical staff toward aggression have been shown to influence the way they manage this behavior. The purpose of this study was to examine the attitudes of nursing staff toward the causes and management of aggression in an emergency department (ED) setting of a tertiary care multispecialty hospital.
Methods: A convenience sample of 35 staff nurses was recruited from the emergency department of a tertiary care hospital in South India. Participants completed the Management of Aggression and Violence Scale (MAVAS), which assessed attitudes toward the causes and management of aggression in psychiatric settings. The study was conducted between August 2017 and December 2017.
Results: A total of 35 clinical staff were invited to take part in the study, and of these, 33 completed the questionnaire. 51.5% of the respondents were male. 87.9% were BSc educated, and 57.6% had 1–3 years of experience in psychiatry. The MAVAS total score showed that 18 (54.5%) respondents had a positive attitude, and the rest of the respondents had a neutral attitude. The respondents had a tendency to disagree that factors directly related to the patient or external and situational factors, such as the environment and other people, contributed to aggressive behaviors. They also disagreed with the statement that patients from certain cultural groups were prone to these behaviors. Respondents had mixed views regarding the prevention and management of aggressive behavior. There was agreement that negotiation and de-escalation could be used more effectively and that seclusion and physical restraint sometimes may be required and should not be discontinued.
Conclusions: Aggression in ED units of multispecialty hospitals occurs occasionally and is problematic. Attitudes of staff nurses toward the causes and management of aggression can affect the way staff manage this behavior. Hence, educational and training initiatives are needed to change the complex and contradictory attitudes of the nursing staff toward aggression for better management of this challenging clinical situation.
Prim Care Companion CNS Disord 2026;28(2):25m04081
Author affiliations are listed at the end of this article.
An emergency department (ED) is a major gateway to health care for a large proportion of the general population. Visits to the ED for mental health reasons account for 10%–15% of all visits.1,2 Individuals with mental illness and mental health issues will continue to present to general hospital EDs for a variety of reasons. The ED serves as the first contact for medical care due to ease of accessibility and round-the-clock availability compared to specialized psychiatric services.3
Aggressive behavior is one of the most common behavioral symptoms requiring ED consultation, and the ED is identified as one of the most high-risk areas for patient violence.4 Violent behavior may get precipitated in the ED, which is often a result of the interaction of illness, patient, environmental/setting, and staff variables. Mental health assessments are often viewed as complex, vague, or ambiguous, requiring time and patience; they are seen as challenging situations to manage by ED staff.5,6 Indeed, the prevalence of patient violence in EDs has risen at an alarming pace worldwide. Around 25% of nurse respondents experienced physical assaults more than 20 times in the 3 years preceding the 2009 study by Gacki-Smith and colleagues, and almost one-fifth of respondents experienced frequent verbal abuse.7 Furthermore, some emergency nurses may have strong thoughts and feelings toward individuals with mental illness that have been ingrained in them by society, such as these patients may exhibit strange and unpredictable behavior and are to be either feared or ridiculed.8–10
The attitudes of ED nursing staff toward aggression can influence the way they respond to this behavior when shown by patients with mental illness.11 Positive attitudes may influence the adoption of person-centered approaches, whereas negative attitudes may contribute to the use of containment measures. The existing literature provides inconsistent findings regarding the attitudes of staff toward aggressive patients with mental illness.12 Studies have reported a significant relationship between staff with negative attitudes toward aggressive patients and the use of physical and chemical restraint, which can culminate in adverse health outcomes.13
Research is scarce regarding the attitudes of ED nursing staff toward the causes and management of patient aggression in psychiatry. In light of the relationship between attitudes toward aggression and the adoption of measures to deal with this behavior, as well as the implications for the patient’s safety and well-being, the aim of the current study was to examine the attitudes of ED nursing staff toward the causes and management of aggression in emergency settings.
METHODS
A survey design was used, incorporating a structured questionnaire. A convenience sample of 35 staff nurses was recruited from the emergency medicine department of a tertiary care hospital in South India. Staff nurses received verbal invitations to participate. Written informed consent was obtained from the staff who willingly agreed to participate. The study was conducted between August 2017 and December 2017.
Respondents were asked to react to written statements regarding the causes of aggression and its management. Their evaluation of the statements about aggression was considered an expression of their attitudes toward the causes and management of aggression. The assumption was made that sociodemographic and environmental characteristics may have an impact on nurses’ attitudes toward aggression.
Instrument
The Management of Aggression and Violence Scale (MAVAS) was used to assess attitudes toward the causes of and ways to manage aggression.14 The respondents were instructed to answer all items based on their perceptions and experiences within their own specific ED and hospital setting. The MAVAS originally contained 27 items on a 4-point Likert scale, ranging from 1 (strongly agree) to 4 (strongly disagree), with the cutoff for agreeing set at 2.5 (a 5-point version of the scale is also available). A low score indicates agreement with a statement. The scale has undergone psychometric evaluation and has been shown to contain a strong 4-factor structure: (1) internal (5 points): aggression is mainly due to factors within the aggressive person; (2) external (3 points): aggression is mainly caused by influences in the person’s physical or social environment; (3) situational/interactional (5 points): aggression is attributable to factors in the immediate environment; and (4) approaches to the management of aggression (14 points). Ethical approval to carry out the study was obtained from the Institutional Ethics Committee of the hospital.
Statistical Analysis
Data analyses were conducted using SPSS, version 15. Frequencies, percentages, means, and standard deviations were used to analyze the sociodemographic characteristics of the respondents. Associations between attitude and selected sociodemographic variables were analyzed by χ2 test.
RESULTS
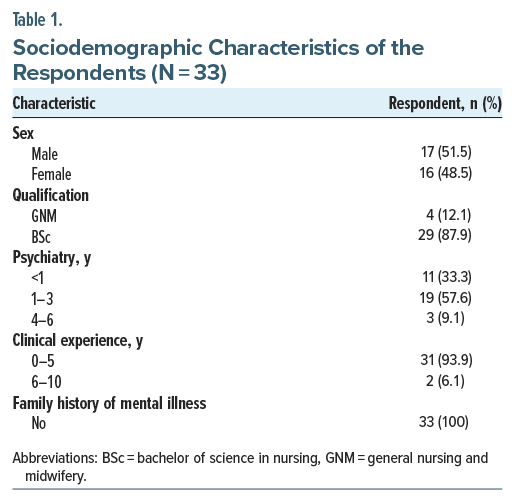
Sociodemographic Characteristics of Participants
A total of 35 clinical staff were invited to take part in the study, of whom 33 completed the questionnaire. Of the respondents, 51.5% were male. All the respondents were aged 20–30 years; 87.9% were BSc educated, and 57.6% had 1–3 years of experience in psychiatry. The MAVAS total score revealed that 18 (54.5%) respondents had a positive attitude, while the rest had a neutral attitude. The MAVAS total score was not correlated with age, sex, education level, clinical experience, or psychiatric experience. The sociodemographic characteristics are summarized in Table 1.
Causes of Aggression
Internal factors. The mean scores of all 5 statements in this domain were >2.5, suggesting that respondents did not believe that factors directly attributable to the patient are contributing to the violent behavior among patients with mental illness. The respondents disagreed with the perception that aggression was common and not preventable in patients with mental illness. They disagreed with the belief that patients become aggressive because they are ill and that particular types of patients are prone to aggression. They also disagreed with the belief that aggressive patients should control their feelings toward the staff and that such behavior would resolve on its own if the patient was left alone (Table 2).
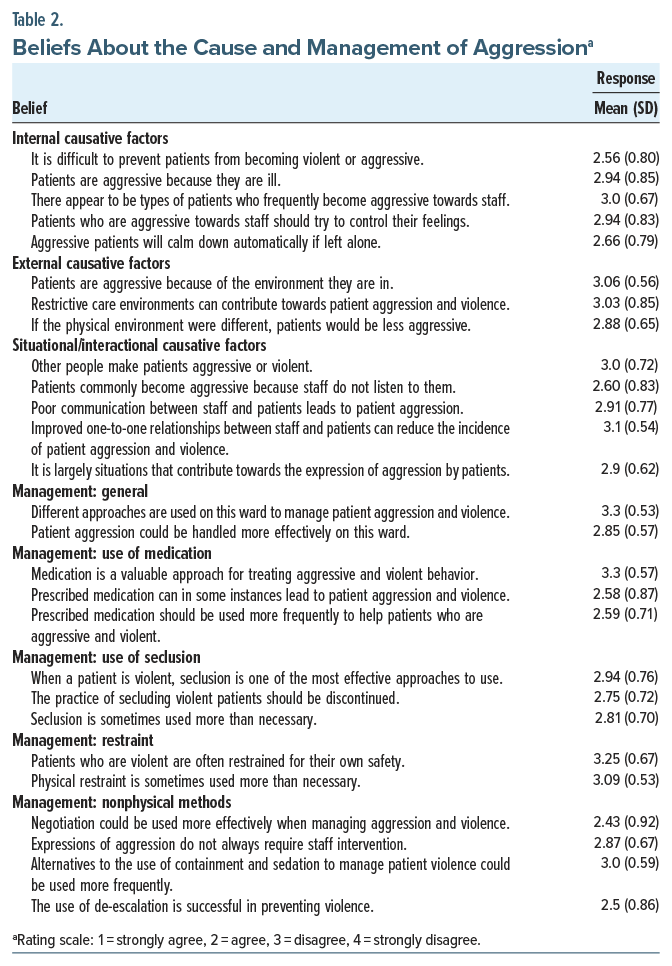
External factors. The mean scores of all 3 statements in this domain were >2.5, indicating that respondents tended to disagree that environmental factors were influential in causing aggression. The respondents disagreed with the belief that a restrictive care environment contributes to aggressive behavior and that a better physical environment could prevent aggressive behavior (Table 2).
Situational/interactional factors. The mean scores of all 5 statements in this domain were >2.5, suggesting that respondents did not believe that factors in the immediate situation, such as other people, poor listening, and communication by the staff, contributed to aggressive behavior. They also did not believe that improved one-to-one communication between staff and patients could reduce the incidence of patient aggression and violence (Table 2).
Management of Aggression
The mean scores of 2 statements regarding the general management of aggressive behaviors were >2.5, indicating that respondents disagreed with the statements on the existence of different approaches in the management of violent patients in the ward and that patient aggression could be dealt with more effectively in the units. Interestingly, respondents disagreed with the statement regarding medications as a valuable approach for treating violent patients (mean=3.3). They also disagreed with the statements regarding the role of prescribed medications in precipitating violence and their more frequent use in aggressive patients. The respondents indicated disagreement that seclusion was one of the most effective ways to deal with this form of behavior, that restraint and seclusion were sometimes used more often than necessary, and that patients were usually restrained for their own safety. Moreover, there was disagreement with the statement that the practice of seclusion should be discontinued. The respondents also indicated disagreement with the statement that patients who are violent are often restrained for their own safety, but they did not believe that restraint is sometimes used more than necessary. They agreed with the statement regarding the effectiveness of negotiations in the management of aggressive patients. The respondents also indicated disagreement with the statement about whether or not staff should always intervene in situations when patients were aggressive and that alternatives to the use of containment and sedation to manage patient violence could be used more frequently. However, there was agreement-to-disagreement regarding the use of de-escalation in preventing violence.
DISCUSSION
The findings of our investigation offer profound insights into the perspectives of nurses regarding the underlying causes and management of aggression and violence within the ED of a tertiary care hospital. Concerning the causative factors, the participants expressed disagreement with the notion that intrinsic or direct patient-related elements were instrumental in precipitating violent behavior. They did not perceive aggression as being intrinsically linked to the patients’ illnesses nor did they identify any specific categories of patients who might be more predisposed to aggression than others. This observation suggests that the respondents were less inclined to attribute culpability to patients for their aggressive behavior. However, this conclusion is incongruent with the existing literature. In prior analogous studies involving nursing personnel, respondents indicated that patients exhibiting specific conditions were more vulnerable to aggressive and violent behaviors, notably those with persecutory delusions, impulsivity, thought disorders, neuropsychological impairments, disorganized behavior, and substance abuse. The literature further suggests that the likelihood of such behaviors is heightened during the acute phase of psychotic illness.15–19
The respondents in the current study exhibited a tendency to dissent regarding the notion that external, situational, or interactional influences played a role in the manifestation of aggressive behavior. These findings stand in stark contrast to previous studies. A restrictive environment, characterized by locked wards, incessant and irritating noises, and a dearth of privacy, significantly heightens the likelihood of frustration, which, in turn, fosters aggressive behaviors.20–22 Furthermore, prior research has demonstrated that inadequate communication between staff and patients, along with aversive and excessively critical behaviors exhibited by staff toward patients, significantly contributes to aggressive behaviors among inpatients.23
In the context of managing patient aggression, the ED nurses exhibited a notable reluctance to acknowledge that the management of such behavior necessitates diverse methodologies. Furthermore, they demonstrated a lack of commitment to enhancing their efficacy in addressing patient aggression. Their perception of pharmacologic interventions as a valuable strategy for mitigating aggressive conduct was markedly deficient, and they expressed dissent toward the more frequent utilization of medications in the control of aggressive behavior. These observations stand in stark contrast to the prevailing literature, which indicates that person-centered and judicious medication-use techniques can significantly moderate the propensity for aggressive behavior.24 However, they did not regard prescribed medications as a contributing factor to aggression among patients.
The respondents in the current study exhibited a tendency to oppose seclusion as one of the most effective strategies for managing aggressive patients. They also expressed disagreement with the practice of restraint as a means of ensuring patient safety. However, opinions were divided regarding the proposition that the practice of seclusion should be discontinued. Furthermore, they contested the assertion that seclusion and restraint were employed more frequently than necessary in the management of aggression. Previous studies among nursing staff have similarly indicated a preference for retaining the option to utilize seclusion.25,26 As our findings suggest, the respondents may perceive pharmacologic interventions as inadequate for addressing all manifestations of aggression. Furthermore, staff practices may be adversely influenced by situational and contextual factors within the workplace, as well as broader cultural dynamics, rendering them resistant to change.12
The respondents also concurred on the efficacy of nonphysical approaches for managing aggressive patients, such as negotiation and de-escalation techniques. However, they expressed reservations regarding the more frequent implementation of these alternatives in place of containment and sedation when addressing violent patients. Furthermore, they acknowledged the critical role of staff interventions in all instances of violence.
CONCLUSION
Our study offers numerous invaluable insights into the critical issue of nurses’ attitudes toward the causes and management of aggression, thereby enriching the sparse body of research pertaining to this phenomenon within the ED context. The attitudes of emergency nurses regarding the origins and management of patient violence exert a profound influence and are directly correlated with the strategies employed to address this complex behavior. The results of this study indicate that emergency nurses harbor divergent perspectives concerning the most efficacious and acceptable methods for preventing and managing such challenging conduct, underscoring the necessity for a comprehensive approach to aggression management that encompasses pharmacologic, restrictive, and nonphysical strategies. The implications of the findings from this study are significant across clinical, educational, and policy domains.
Article Information
Published Online: March 26, 2026. https://doi.org/10.4088/PCC.25m04081
© 2026 Physicians Postgraduate Press, Inc.
Submitted: September 12, 2025; accepted December 19, 2025.
To Cite: Uvais NA, Rahman AMAU, Shihabudheen DP. Attitudes of emergency department nurses toward violent patients with mental illness. Prim Care Companion CNS Disord. 2026;28(2):25m04081.
Author Affiliations: Department of Psychiatry, Iqraa International Hospital and Research Centre, Calicut, Kerala, India (Uvais, Shihabudheen); Department of Psychiatry, Government Medical College, Kozhikode, India (Rahman).
Corresponding Author: N. A. Uvais, MBBS, DPM, Iqraa International Hospital and Research Centre, Calicut, Kerala, India ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Clinical Points
- Staff attitudes significantly influence aggression management, with over half of surveyed nurses holding neutral—not positive—views on causes and management.
- Nurses tended to disagree that patient factors, environment, or culture are primary causes of aggression, potentially overlooking key triggers and preventative strategies.
- Staff endorsed de-escalation techniques but also agreed on the necessity of seclusion and restraint, revealing mixed attitudes requiring targeted education.
References (26)

- Clarke D, Hughes L, Brown AM, et al. Psychiatric emergency nurses in the emergency department: the success of the Winnipeg, Canada experience. J Emerg Nurs. 2005;31(4):351–356. PubMed CrossRef
- Owens PL, Mutter R, Stocks C. Mental health and substance abuse related emergency department visits among adults in 2007. In: HCUP Statistical Brief #92. Rockville, MD: Agency for Healthcare Research and Quality; 2010.
- Clarke DE, Brown AM, Hughes L. Mental health and illness in the emergency department. In Health Education: Challenges, Issues, and Impact (pp.97-117). Fortier A, Turcotte S (eds). Novascience Publications, New York. 2010.
- Kit WW. Nurses’ attitude towards patient violence in emergency department. Nurs Care Open Access J. 2016;1(3):00012.
- Crowley JJ. A clash of cultures: A&E and mental health. Accid Emerg Nurs. 2000;8(1):2–8. PubMed CrossRef
- Karshmer JF, Hales A. The role of the psychiatric clinical nurse specialist in the emergency department. Clin Nurse Spec. 1997;11(6):264–268. PubMed CrossRef
- Gacki SJ, Juarez AM, Boyett L, et al. Violence against nurses working in US emergency departments. J Nurs Adm. 2009;39(7/8):340–349. PubMed CrossRef
- Sartorius N. Stigma and mental health. Lancet. 2007;370(9590):810–811. PubMed CrossRef
- Schulze B. Stigma and mental health professionals: a review of the evidence on an intricate relationship. Int Rev Psychiatry. 2007;19(2):137–155. PubMed CrossRef
- Thornicroft G. Shunned: Discrimination against people with mental illness. Oxford: Oxford University Press; 2007. CrossRef
- Jansen GJ, Middel B, Dassen TW, et al. Cross-cultural differences in psychiatric nurses’ attitudes to inpatient aggression. Arch Psychiatr Nurs. 2006;20(2):82–93. PubMed CrossRef
- McCann, Baird J, Muir-Cochrane E. Attitudes of clinical staff toward the causes and management of aggression in acute old age psychiatry inpatient units. BMC Psychiatry. 2014;14:80. PubMed CrossRef
- Nakahira M, Moyle W, Creedy D, et al. Attitudes toward dementia-related aggression among staff in Japanese aged care settings. J Clin Nurs. 2009;18(6):807–816. PubMed CrossRef
- Duxbury J. Testing a new tool: the Management of Aggression and Violence Scale (MAVAS). Nurse Res. 2003;10(4):39–52. PubMed CrossRef
- Lewis CF, Fields C, Rainey E. A study of geriatric forensic evaluees: who are the violent elderly?. J Am Acad Psychiatry L. 2006;34(3):324–332. PubMed
- Ferguson CJ, Averill PM, Rhoades H, et al. Social isolation, impulsivity and depression as predictors of aggression in a psychiatric inpatient population. Psychiatr Quart. 2005;76(2):123–137. PubMed CrossRef
- Chaplin R, McGeorge M, Hinchcliffe G, et al. Aggression on psychiatric inpatient units for older adults and adults of working age. Int J Geriatr Psychiatry. 2008;23(8):874–876. PubMed CrossRef
- Pulsford D, Duxbury J. Aggressive behaviour by people with dementia in residential care settings: a review. J Psychiatr Ment Health Nurs. 2006;13(5):611–618. PubMed CrossRef
- Steinert T, Wolfle M, Gebhardt RP. Measurement of violence during in-patient treatment and association with psychopathology. Acta Psychiatr Scand. 2000;102(2):107–112. PubMed CrossRef
- Papadopoulos C, Ross J, Stewart D, et al. The antecedents of violence and aggression within psychiatric in-patient settings. Acta Psychiatr Scand. 2012;125(6):425–439. PubMed CrossRef
- Daffern M, Howells K. Psychiatric inpatient aggression: a review of structural and functional asessment approaches. Aggress Violent Behav. 2002;7:477–497. CrossRef
- Nijman HL. A model of aggression in psychiatric hospitals. Acta Psychiatr Scand Suppl. 2002;106(s412):142–143. PubMed CrossRef
- Whittington R, Wykes T. Aversive stimulation by staff and violence by psychiatric patients. Br J Clin Psychol. 1996;35(1):11–20. PubMed CrossRef
- Pulsford D, Duxbury JA, Hadi M. A survey of staff attitudes and responses to people with dementia who are aggressive in residential care settings. J Psychiatr Ment Health Nurs. 2011;18(2):97–104. PubMed CrossRef
- Duxbury J, Whittington R. Causes and management of patient aggression and violence: staff and patient perspectives. J Adv Nurs. 2005;50(5):469–478. PubMed CrossRef
- Foster C, Bowers L, Nijman H. Aggressive behaviour on acute psychiatric wards: prevalence, severity and management. J Adv Nurs. 2007;58(2):140–149. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





