Catatonia is a complex neuropsychiatric syndrome that may occur across a spectrum of psychiatric and medical conditions.1 Periodic catatonia (PC), a rare and underrecognized subtype, is characterized by recurring episodes of catatonia interspersed with periods of normal functioning.2 It is commonly reported in association with mood disorders, particularly bipolar disorder, which may account for its cyclical nature. We report a rare case of PC in an adult with autism spectrum disorder (ASD), in the absence of any other identifiable psychiatric or neurological comorbidities, that responded to lithium prophylaxis.
Case Report
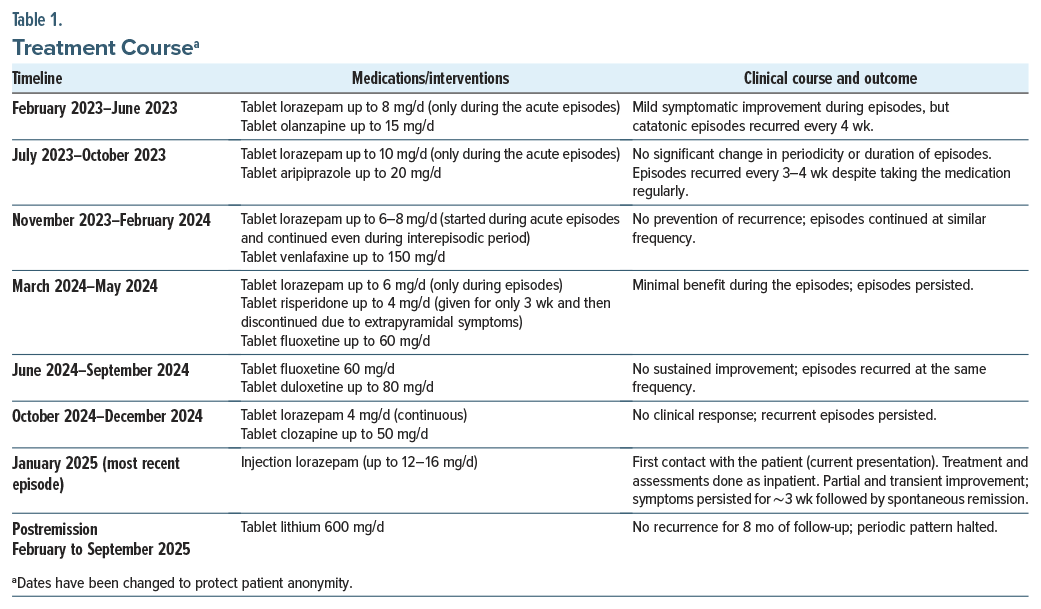
Mr S, a 30-year-old man, presented to the psychiatry outpatient department with a 2-year history of 15-to 28-day–long episodes marked by abrupt-onset mutism, posturing, staring, repetitive hand rubbing, reduced food intake, and rigidity. These symptoms fluctuated in intensity throughout the day, and during more severe phases, he even experienced bowel and bladder incontinence. Food intake and sleep were markedly reduced during these episodes, causing significant distress. Each episode was followed by a period of complete spontaneous symptomatic recovery lasting 3–4 weeks. Over 2 years, he experienced 10–12 episodes despite receiving multiple psychotropics for adequate durations (Table 1).
At the current presentation, his Bush-Francis Catatonia Rating Scale (BFCRS)3 score was 21, which decreased to 11 after an intravenous 2-mg lorazepam challenge. His previous medications were discontinued, and he was maintained on lorazepam (up to 12–16 mg/day). Despite treatment, symptoms persisted for 2 weeks with BFCRS scores fluctuating between 10 and 20 before spontaneous remission, similar to previous episodes. Electroconvulsive therapy was not considered given the periodic nature and the consistent pattern of spontaneous recovery observed in prior episodes. There was no history of psychotic or mood symptoms in any of the episodes including the current episode. Detailed developmental history revealed delayed language milestones, poor social reciprocity, restricted interests, emotional detachment, and an excessive need for routine—features suggestive of ASD. Diagnosis was confirmed using the Indian Scale for Assessment of Autism.4 Neurological workup, including neuroimaging and autoimmune profile, was unremarkable.
A diagnosis of catatonia associated with ASD (ICD-11 codes: 6A40 and 6A02) was considered most appropriate, although a definitive cause for the periodicity could not be determined. Given the cyclicity and lack of response to prior treatments, lithium was initiated prophylactically at 600 mg/day following spontaneous remission of the most recent episode. He was maintained on lithium monotherapy with serum levels of 0.47 mmol/L. At 8-month follow-up, the patient remained free of catatonic episodes and functionally stable.
Discussion
PC was first described by Kraepelin (1908) in schizophrenia and later investigated by Gjessing (1938), who proposed nitrogen balance changes as a possible contributor.5 Since then, literature on PC has remained limited to a few case reports, primarily in the context of mood and psychotic disorders.5–7 It has also been reported in a few cases of frontal lobe epilepsy8 and encephalitis.9 A review of the literature for the treatment of PC revealed only 5 case reports supporting lithium’s efficacy in managing PC prophylactically,10–14 including one with a 9-year symptom-free follow-up indicating its long-term efficacy.10 Evidence for other agents remains even more limited, with isolated reports involving antipsychotics like olanzapine15 and risperidone,16 both ineffective in our patient, as well as mirtazapine17 and lamotrigine.18 While catatonia is well recognized in ASD,19 to the best of our knowledge, PC in this population has not been previously reported. The British Association for Psychopharmacology guidelines to manage catatonia (2023) acknowledged PC as a distinct subtype and recommended lithium for prophylaxis based on a few case reports.2 Our case supports this recommendation, demonstrating that lithium, even at low serum levels, can be effective and well tolerated in preventing recurrence of PC at least in the short term, even in the presence of a neurodevelopmental condition like ASD. Early recognition of such catatonic patterns in primary care can prevent unnecessary medication trials and facilitate timely interventions.
Article Information
Published Online: February 3, 2026. https://doi.org/10.4088/PCC.25cr04066
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(1):25cr04066
Submitted: August 21, 2025; accepted October 30, 2025.
To Cite: Bakam A, Raina S, Reddy YCJ. Periodic catatonia in an adult with autism spectrum disorder responding to lithium: A case report. Prim Care Companion CNS Disord. 2026;28(1):25cr04066.
Author Affiliations: Department of Psychiatry, National Institute of Mental Health and Neurosciences, Bangalore, India (Raina, Reddy); Department of Psychiatry, All India Institute of Medical Sciences, Bibinagar, Hyderabad, India (Bakam).
Corresponding Author: Anirudh Bakam, MD, All India Institute of Medical Sciences (AIIMS) Bibinagar, Hyderabad, India ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient and family to publish this case report, and information, including dates, has been de-identified to protect patient anonymity.
ORCID: Anirudh Bakam: https://orcid.org/0009-0009-7738-3082
References (19)

- Pathak H, Susan Varghese S, Suhas S, et al. Risk factors for catatonia relapse in psychotic and affective disorders. JAMA Psychiatry. 2025:e251818.
- Rogers JP, Oldham MA, Fricchione G, et al. Evidence-based consensus guidelines for the management of catatonia: recommendations from the British Association for Psychopharmacology. J Psychopharmacol Oxf Engl. 2023;37(4):327–369. PubMed CrossRef
- Bush G, Fink M, Petrides G, et al. Rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129–136. PubMed CrossRef
- Deshpande S. Indian Scale for Assessment of Autism-Test Manual; 2008. doi:10.13140/RG.2.1.3240.4004 CrossRef
- Prasad A, Avinash P, Victor R, et al. Periodic catatonia: a tangled spectra within neuropsychiatry. Ann Indian Psychiatry. 2024;8(4):341. CrossRef
- Hervey WM, Stewart JT, Catalano G. Diagnosis and management of periodic catatonia. J Psychiatry Neurosci. 2013;38(3):E7–E8. PubMed CrossRef
- Ghaffarinejad AR, Sadeghi MM, Estilaee F, et al. Periodic catatonia. Challenging diagnosis for psychiatrists. Neurosci Riyadh Saudi Arab. 2012;17(2):156–158. PubMed
- Leentjens A, Pepplinkhuizen L. A case of periodic catatonia, due to frontal lobe epilepsy. Int J Psychiatry Clin Pract. 1998;2(1):57–59. PubMed CrossRef
- Sutar R, Rai NK. Revisiting periodic catatonia in a case of SSPE and response to intrathecal interferon: a case report. Asian J Psychiatry. 2020;51:101996. PubMed CrossRef
- Petursson H. Lithium treatment of a patient with periodic catatonia. Acta Psychiatr Scand. 1976;54(4):248–253. PubMed CrossRef
- Padhy SK, Subodh B, Bharadwaj R, et al. Recurrent catatonia treated with lithium and carbamazepine: a series of 2 cases. Prim Care Companion CNS Disord. 2011;13(1):PCC.10l00992. PubMed
- Sato Y, Shinozaki M, Okayasu H, et al. Successful treatment with lithium in a refractory patient with periodic catatonic features: a case report. Clin Neuropharmacol. 2020;43(3):84–85. PubMed CrossRef
- Sovner RD, McHugh PR. Lithium in the treatment of periodic catatonia: a case report. J Nerv Ment Dis. 1974;158(3):214–221. PubMed CrossRef
- Wald D, Lerner J. Lithium in the treatment of periodic catatonia: a case report. Am J Psychiatry. 1978;135(6):751–752. PubMed CrossRef
- Guzman CS, Myung VHM, Wang YP. Treatment of periodic catatonia with atypical antipsychotic, olanzapine. Psychiatry Clin Neurosci. 2008;62(4):482. PubMed CrossRef
- Duggal HS, Gandotra G. Risperidone treatment of periodic catatonia. Can J Psychiatry Rev Can Psychiatr. 2005;50(4):241–242. PubMed CrossRef
- Yeh YW, Chen CY, Kuo SC, et al. Mirtazapine treatment of periodic catatonia in organic mental disorder: a case report. Prog Neuropsychopharmacol Biol Psychiatry. 2010;34(3):553–554. PubMed CrossRef
- Konstantinou G, Papageorgiou CC, Angelopoulos E. Periodic catatonia: long-term treatment with Lamotrigine: a case report. J Psychiatr Pract. 2021;27(4):322–325. PubMed CrossRef
- Vaquerizo-Serrano J, Salazar DPG, Singh J, et al. Catatonia in autism spectrum disorders: a systematic review and meta-analysis. Eur Psychiatry. 2022;65(1):e4.
Enjoy this premium PDF as part of your membership benefits!





