Objective: While suicidal ideation is a recognized risk factor for future suicidal behavior, clinicians often subtype ideation in an effort to further clarify risk. This study referred to the SAFE (Suicide Assessment Form in Emergency Psychiatry) database to examine individuals who were assessed for suicidal ideation in the emergency department (ED) to determine whether ideation subtypes (active desire for death versus ambivalence about living) differentially predicted future suicide attempt.
Methods: Participants were individuals presenting to psychiatric services in the ED between January 1, 2009, and December 31, 2013, at 2 hospitals in Manitoba, Canada. People presenting with suicidal ideation were subtyped as having either ambivalence about living or active suicidal ideation. These presentations were examined as predictors of suicide attempt (defined by the Columbia Classification Algorithm for Suicide Assessment scale) within 6 months in regression models that adjusted for confounders.
Results: Of the 5,655 individuals presenting to the ED during the study, 158 (3.1%) presented again within 6 months with a suicide attempt. Individuals presenting with ambivalence about living showed more than a doubling in risk for future suicide attempts (odds ratio [OR] = 2.57, 95% CI = 1.64-4.02, P < .001). Active suicidal ideation also predicted attempts (defined by the within 6 months, with more than a tripling of risk compared to people who were not suicidal at baseline (OR = 3.75, 95% CI = 2.61-5.34, P < .001).
Conclusions: Psychiatric presentations to the ED often include suicidal ideation. Both active suicidal ideation and ambivalence about living are concerning presentations associated with risk of attempt within 6 months. Clinicians should be mindful that differentiating between active suicidal ideation and ambivalence about living may downplay the severity of the latter presentation.
Ambivalence About Living and the Risk for Future Suicide Attempts:
A Longitudinal Analysis
ABSTRACT
Objective: While suicidal ideation is a recognized risk factor for future suicidal behavior, clinicians often subtype ideation in an effort to further clarify risk. This study referred to the SAFE (Suicide Assessment Form in Emergency Psychiatry) database to examine individuals who were assessed for suicidal ideation in the emergency department (ED) to determine whether ideation subtypes (active desire for death versus ambivalence about living) differentially predicted future suicide attempt.
Methods: Participants were individuals presenting to psychiatric services in the ED between January 1, 2009, and December 31, 2013, at 2 hospitals in Manitoba, Canada. People presenting with suicidal ideation were subtyped as having either ambivalence about living or active suicidal ideation. These presentations were examined as predictors of suicide attempt (defined by the Columbia Classification Algorithm for Suicide Assessment scale) within 6 months in regression models that adjusted for confounders.
Results: Of the 5,655 individuals presenting to the ED during the study, 158 (3.1%) presented again within 6 months with a suicide attempt. Individuals presenting with ambivalence about living showed more than a doubling in risk for future suicide attempts (odds ratio [OR] = 2.57, 95% CI = 1.64–4.02, P < .001). Active suicidal ideation also predicted attempts (defined by the within 6 months, with more than a tripling of risk compared to people who were not suicidal at baseline (OR = 3.75, 95% CI = 2.61–5.34, P < .001).
Conclusions: Psychiatric presentations to the ED often include suicidal ideation. Both active suicidal ideation and ambivalence about living are concerning presentations associated with risk of attempt within 6 months. Clinicians should be mindful that differentiating between active suicidal ideation and ambivalence about living may downplay the severity of the latter presentation.
Prim Care Companion CNS Disord 2019;21(2):18m02361
To cite: Naherniak B, Bhaskaran J, Sareen J, et al. Ambivalence about living and the risk for future suicide attempts: a longitudinal analysis. Prim Care Companion CNS Disord. 2019;21(2):18m02361.
To share: https://doi.org/10.4088/PCC.18m02361
© Copyright 2019 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry, University of Manitoba, Winnipeg, Manitoba, Canada
bDepartment of Psychology, University of Manitoba, Winnipeg, Manitoba, Canada
cDepartment of Community Health Sciences, University of Manitoba, Winnipeg, Manitoba, Canada
*Corresponding author: James M. Bolton, MD, University of Manitoba, PZ430-771, Bannatyne Ave, Winnipeg, Manitoba, Canada, R3E 3N4 ([email protected]).
Suicide claims more than 800,000 lives each year worldwide1 and is the 10th leading cause of death in people aged 15 to 34 years in Canada.2 For every suicide death, there are approximately 20 attempts.3 While prediction of suicide attempts and future suicide risk is difficult, 4–7 suicide prevention strategies nevertheless aim to identify those at risk of future suicidal behavior6,7 and attempt to stratify the level of risk.8–10 One area of focus has been the assessment of individuals with suicidal ideation and the implementation of appropriate interventions.10,11
Suicidal ideation is considered a first step in the path leading to suicidal behavior,7,12,13 and the rate of suicide in those with suicidal ideation is greater than in the general public.14 Suicidal thoughts are prevalent: the lifetime prevalence rate of suicidal ideation for the general population is estimated to be 14%.15 According to the National Comorbidity Survey,16 34% of individuals transition from suicidal ideation to a plan, 72% proceed from a plan to an attempt, and 26% progress from ideation to an unplanned attempt.Ninety percent of unplanned and 60% of planned first attempts occurred within 1 year of the onset of ideation.17 These findings are replicated in other populations, with studies17–19 showing that 60% of individuals transition from ideation to plan and attempt suicide within 1 year of ideation onset. Fortunately, evaluation of suicidal ideation coupled with treatment of existing mental disorders can reduce the number of suicide attempts,18 reiterating the importance of suicidal ideation as a stage of intervention.20–24
Early recognition of suicide risk is important, as most males and a substantial proportion of females die in their first suicide attempt.25 With 1 in 20 suicide attempts resulting in death,1 and previous suicidal ideation perhaps being one of the strongest predictors of incident suicide attempts,24 suicidal ideation gives cause for concern. The risk of attempts increases as a function of frequency of suicidal ideation, with even mild and relatively infrequent thoughts leading to increased risk of suicide attempt.20 Thus, suicidal ideation is important in the assessment of suicide risk and selection of the level of intervention,24,25 and its assessment is a priority in the evaluation of those with no current or previous suicide plan.12,19
While efforts have been made to revise the nomenclature for the study of suicidal ideation, ambiguity remains,26–29 and the point at which ideation becomes clinically significant is not yet obvious.19 However, general consensus is that suicidal behaviors fall on a continuum. Suicidal ideation is defined as a desire for death or thoughts to kill oneself.19 Suicidal ideation is occasionally specified as passive (an ambivalence toward living) or active (clear intention of wanting to kill oneself). These ideation subtypes are poorly understood in terms of their severity and outcomes, and the limited literature in this area is conflicting. Active wishes to kill oneself are thought to be more serious than a passive thought about death,26 but passive suicidal ideation can be more persistent and difficult to treat.30 A wish to die has been shown to be associated with higher levels of suicide attempts, whereas ambivalence about living and a wish to live were associated with lower levels of suicidal behavior.29 Another study15 showed that passive suicidal ideation did not increase the risk of suicide plans or attempts and may even decrease these risks. However, other studies31–33 did not find major differences between those exhibiting passive or active suicidal ideation when comparing course or outcome. Furthermore, passive and active suicidal ideation can both occur within the same individual; 1 study29 found that people who experienced both a passive desire for death and suicidal ideation had a higher risk for suicide attempts than either subtype alone. The literature to date has primarily been cross-sectional in nature, and, as such, the clinical utility of subtyping suicidal ideation is largely unknown.
The main objective of the current study was to determine whether the ideation subtypes of active suicidal ideation and ambivalence about living (or what is commonly referred to as passive suicidal ideation) are associated with risk of future suicide attempt within 6 months. A secondary objective was to examine the clinical and demographic factors that are correlated with the different ideation subtypes. The use of a large clinical sample and longitudinal design, along with standardized measures and physician assessment of all presentations, allowed this study to overcome many of the described limitations of prior research. On the basis of past literature,7,34 we hypothesized that active suicidal ideation would be predictive of future suicide attempts within 6 months.
METHODS
Setting
The data used in this study came from the SAFE (Suicide Assessment Form in Emergency Psychiatry) database project, a large study involving 2 tertiary care hospitals in Winnipeg, Manitoba, Canada, that examined risk factors for suicide after emergency department (ED) presentation. These 2 hospitals in Winnipeg handle approximately 40% of all ED visits.35 In addition, individuals who require psychiatric assessment from other Winnipeg EDs are often transferred to these 2 hospitals for further assessment. The study period was 5 years from January 1, 2009, to December 31, 2013. Psychiatric services in the ED are provided 24 hours per day by residents and staff psychiatrists associated with the Department of Psychiatry at the University of Manitoba.
Study Population
The study population included all consecutive presentations to psychiatric services covering the 2 described sites during the study period (11,315 presentations). For the purposes of this study, we differentiated between multiple presentations made by the same individual and the number of individuals presenting to the hospital. Presentations with missing or incorrect health identification numbers were excluded from the study (n = 658), as they could not be linked to prior or subsequent presentations, leaving us with 10,657 presentations and 6,862 individuals. We excluded individuals if their index and only presentations occurred after June 30, 2013 (n = 553) and if there were missing details about their presentation to the ED that would prevent classification into the different groups (n = 654), leaving us with 9,530 presentations made by 5,655 individuals.
Baseline Patient Assessment
Psychiatric residents conducted the assessment of the patients and were supervised by staff psychiatrists. General psychiatric assessment included a review of the presenting problem, a thorough assessment of mental disorder symptoms, and treatment history. All patients were assessed for suicidal thoughts and behaviors. In addition, basic demographic information (sex, marital status, and age category) was obtained. The physician then completed the SAFE database study form, which included items for suicidal ideation subtypes and other potential risk factors for suicide. Residents and staff psychiatrists received specific training that included education about the SAFE form components and how to correctly complete the form. Baseline presentations were captured from January 1, 2009, to June 30, 2013, to ensure that each person had a full 6 months of follow-up after index presentation. Baseline presentations after June 30, 2013, were included if there was a repeat presentation with suicide attempt prior to December 31, 2013.
Baseline Measures
Suicidal ideation subtype. Unstructured clinical interviews were used to determine if the patient displayed active suicidal ideation or ambivalence about living.
Active suicidal ideation. This item was coded as present if the person presented with a clear and current intention of wanting to kill himself/herself (eg, voicing a firm desire for death, having a plan in place and intent to carry it out).
Ambivalence about living. This item was coded as present if the person described current thoughts about death with no clear intent to act on them (eg, showing no preference for living or dying, thoughts of not wanting to be alive but no plan for self-harm).
Sociodemographic correlates. The following sociodemographic correlates were captured on the SAFE data form as dichotomous measures: sex, age (19–45, > 45 years), marital status (single, married), presence of stressors (yes, no), and presence of social support (yes, no).
Mental and physical disorder correlates. The following health variables were encoded dichotomously (present or absent at time of presentation): depression, substance abuse, psychosis, anxiety, impulsivity, and physical illness.
Primary outcome measure. Suicide attempt within 6 months. People who presented again to 1 of 2 study hospitals with a suicide attempt within 6 months of their baseline presentation were included. A suicide attempt was defined using the Columbia Classification Algorithm for Suicide Assessment scale (C-CASA),36 a standardized scale developed to classify suicidal behavior. The C-CASA specifically assesses self-harm behaviors with intent to die and separates those from self-harm behavior without suicidal intent.
Secondary outcome measure. Repeat presentation type. Individuals who made a repeat presentation to the ED during the study period were categorized according to the type of suicidal behavior using the C-CASA. Seven mutually exclusive categories were considered: (1) suicide attempt; (2) preparatory acts toward imminent suicidal behavior; (3) suicidal ideation; (4) self-injurious behavior, no suicidal intent; (5) self-injurious behavior, intent unknown; (6) not enough information; and (7) presentation did not feature suicidality or self-injurious behavior.
Statistical Analysis
Study participants were categorized into 3 groups at baseline: active suicidal ideation, ambivalence about living, and no suicidal ideation (reference group). If assessors checked both suicidal ideation categories as present, they were considered as active suicidal ideation. The “no ideation” group included individuals with index presentations that featured no suicidal ideation or self-injurious behavior, as determined by C-CASA. Descriptive prevalence rates for each of the variables at baseline were generated using SPSS 21.0.37 Binary logistic regressions were conducted to investigate the associations between baseline measures and suicidal ideation subgroups. Logistic regression was also used to generate odds ratios for the risk of subsequent suicide attempt among each ideation subtype, both unadjusted and adjusted by sex (male, female) and age (19–45, > 45 years). These demographic factors were selected as potential confounders given their consistent association with suicide and suicidal behaviors.38 A survival analysis was conducted using the Cox proportional hazards model to determine time to suicide attempt after initial presentation based on subtype of ideation. Finally, for each of the 3 subtype groupings, rates of subsequent presentations to the ED (categorized by type of subsequent presentation coded by the C-CASA scale) were determined among those individuals with multiple presentations. The purpose of this analysis was to examine the stability versus change of presentation types over time.
Ethical Approval
The study was approved by the Research Ethics Board at the University of Manitoba.
RESULTS
Over the course of the study period, 5,655 individuals were enrolled in the SAFE database project who could be classified into 1 of 3 subgroups (active suicidal ideation: n = 1,241, 22%; ambivalence about living: n = 809, 14%; and no ideation: n = 3,605, 64%) (Figure 1). Prevalence of sociodemographic factors and mental and physical illnesses is presented in Table 1 stratified by suicidal ideation subtype at baseline presentation. Suicide attempts within 6 months of initial presentation varied across subgroups (active suicidal ideation: n = 68, 5.6%; ambivalence about living: n = 31, 3.9%; and no ideation: n = 55, 1.6%).
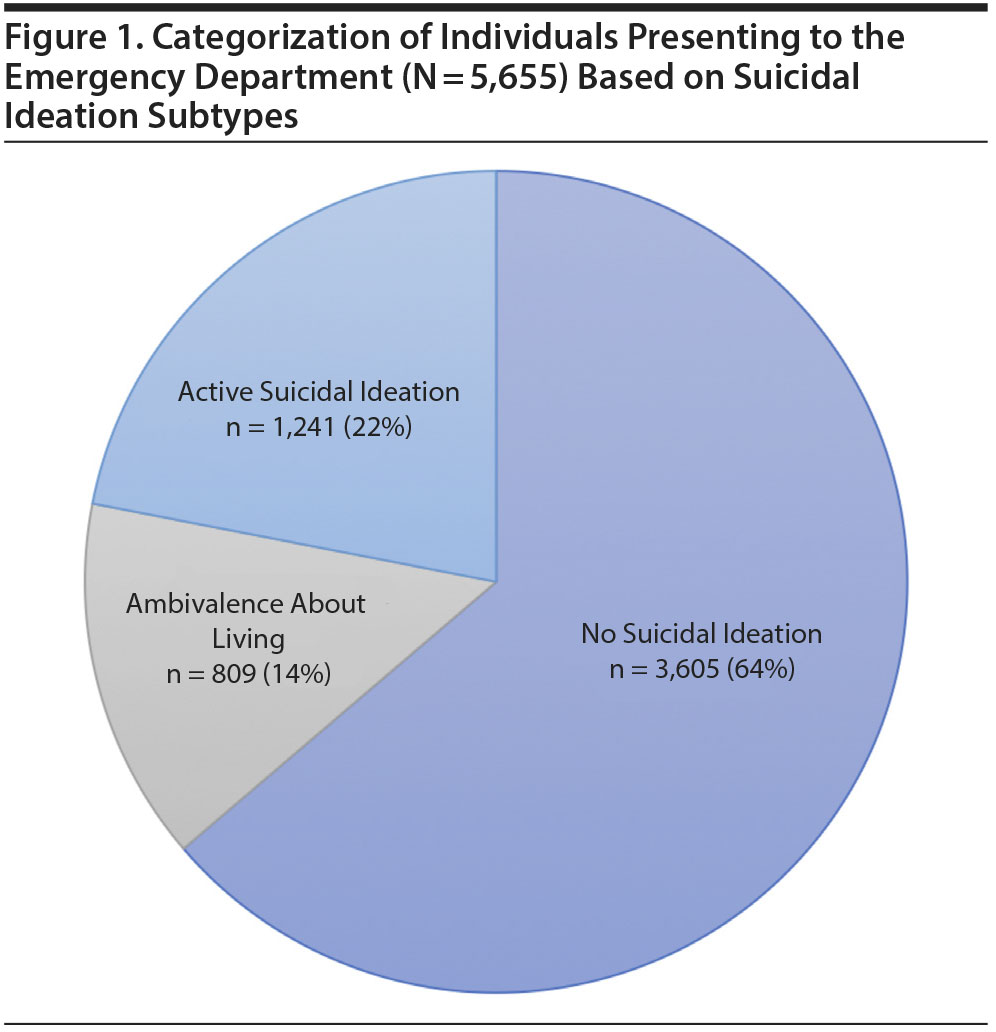
Table 2 displays the association between types of ideation and the baseline variables. Depression was strongly correlated with both groups: active suicidal ideation (OR = 12.56, 95% CI = 10.59–14.59, P < .001) and ambivalence about living (OR = 7.39, 95% CI = 6.19–8.82, P < .001). Younger age was associated only with active suicidal ideation (OR = 1.19, 95% CI = 1.04–1.36, P < .05). Psychosis was negatively associated with suicidal ideation in both groups when compared to individuals who were not suicidal (active suicidal ideation: OR = 0.35, 95% CI = 0.30–0.40, P < .001) or ambivalent about living (OR = 0.38, 95% CI = 0.31–0.46, P < .001). Physical illness and impulsivity were factors associated with both ambivalence about living (physical illness: OR = 1.35, 95% CI = 1.14–1.61, P < .001; impulsivity: OR = 1.24, 95% CI = 1.06–1.45, P < .001) and active suicidal ideation (physical illness: OR = 1.74, 95% CI = 1.49–2.01, P < .001; impulsivity: OR = 1.34, 95% CI = 1.18–1.53, P < .001).
The survival analysis (Figure 2) showed that over the course of the study, approximately 97% of the no suicidal ideation subgroup remained attempt free. With regard to the ambivalence about living subgroup, approximately 93% did not attempt suicide, with approximately 4% of this population making a suicide attempt within the first 6 months of the index presentation. Similar patterns were observed for the active suicidal ideation subgroup, with approximately 90% remaining attempt free and approximately 5% making an attempt within the first 2 months of the index presentation.
Table 3 presents the regression analysis showing the odds of suicide attempt within 6 months for each baseline ideation subgroup. The results reveal that presentations that featured active suicide ideation had a strong magnitude of association with future attempts, with a nearly 4-fold risk when compared to ED visits without suicidal ideation (adjusted OR = 3.82, 95% CI = 2.65–5.50, P < .001). Interestingly, ambivalence about living was correlated with future suicide attempts (adjusted OR = 2.61, 95% CI = 1.67–4.10, P < .001).
Figure 3A–C shows the subsequent presentations made to the ED after initial index presentations among the 3 baseline ideation subgroup members who presented on multiple occasions. Among people with no suicidal ideation at baseline who later returned to the ED, 10% of subsequent presentations featured suicide attempts and 23% featured suicidal ideation, indicating that one-third became suicidal over the course of the study period. Whereas one-quarter of people with ambivalence about living subsequently presented with no suicidal thoughts or self-harm behavior, that was only true for 12% of future presentations among the active suicidal ideation group.
DISCUSSION
The main objective of this article was to study the correlates and outcomes of suicidal ideation subtypes to determine if they suggest specific risk profiles among psychiatric patients in the ED. Using a very large sample of physician-assessed patients with longitudinal follow-up, this study showed that both ambivalent thoughts about living and active suicidal ideation are risk factors for future suicide attempts. Whereas previous studies26,39 and even clinical intuition suggest that ambivalence or passive suicidal ideation are less concerning than active plans for suicide, this study reveals that the former presentations are important markers of risk. Other findings include the high rate of suicidal ideation in psychiatric presentations to the ED and the observation that suicidal presentations change markedly over time among ED patients. Depression was a recurring marker in both ideation groups, highlighting the role played by mental disorders in suicidal ideation. However, psychosis was negatively associated with suicidal ideation in all 3 groups, suggesting the existence of unmeasured confounding.
These results question the clinical utility of distinguishing between active suicidal ideation and more ambivalent thoughts about life. In the ED, clinicians often use the terms active and passive when describing a patient’s suicidal thoughts and occasionally may even base disposition decisions on this distinction. This study suggests that even without a firm intent to suicide, ambivalent thoughts about life are not a reassuring presentation. Furthermore, this subtyping is misleading since passive suicidal ideation is traditionally thought to be less of a risk of future suicide attempt, yet our results found it to be associated with an increased risk. This finding is consistent with previous research, which has found the risk for lifetime suicide attempt is similar among those with passive suicidal ideation when compared to those with more active suicidal ideation.33 Further, although suicides are prevalent among high-risk patients, most suicides are completed by those never identified as high risk.40,41 Simon and colleagues42 suggest that “suicidal ideation should be viewed as an enduring vulnerability rather than simply a short-term crisis,”(p1201) emphasizing its importance as a risk factor for subsequent suicidal behavior.
Important limitations exist when interpreting these results. First, we did not measure completed suicides but rather only suicide attempts. It is possible that the rate of completed suicides may differ between the ideation subgroups, and, as such, their inclusion could influence the results. Also, we were unable to assess the influence of hospitalization, which may be correlated to both the presentation type and the outcome of suicide attempt. We were also limited to 2 EDs in this study. However, these EDs combined handle approximately 40% of all ED visits in the city, being the largest tertiary care hospitals in Winnipeg. Another area of limitation was that we did not use a standardized tool for assessing suicidal ideation, its type, or severity (ie, the Beck Scale for Suicide Ideation43 or the Suicide Intention Scale44). This lack of a standardized tool potentially introduces greater variability in the assessment of suicidal ideation and could lead to coding errors based on practitioner inquiry or skill. Correlates such as depression were dichotomously coded and, therefore, likely to yield both false positives and negatives. This method was employed as a way of rapidly capturing a variety of measures in a busy clinical setting wherein lengthier standardized assessments were not feasible on large volumes of patients. Additionally, we were limited in the sociodemographic variables that could be assessed in this study, including the inability to assess race or ethnicity. Research into the relationship between ethnicity and suicidal behavior shows a higher prevalence among the Canadian indigenous population, especially among indigenous women.45
In conclusion, psychiatric presentations to the ED often include suicidal ideation. While increasing the risk for future suicide attempts within 6 months from presentation, differentiating between active and passive suicidal ideation does not appear to help in predicting outcomes and may even provide a false sense of security by downplaying the severity of presentations that include ambivalence about living. Mental health professionals should view presentations involving any form of suicidal ideation as a serious risk for future attempts and consider appropriate resources, support, and treatment. Future studies looking at passive versus active suicidal ideation and completed suicides are warranted.
Submitted: July 30, 2018; accepted November 30, 2018.
Published online: March 7, 2019.
Author contributions: Ms Bhaskaran and Dr Bolton were primarily responsible for the data analyses. Dr Naherniak was responsible for writing the manuscript. All co-authors participated in preparation of the manuscript. All co-authors were also responsible for the conceptualization and design of the study and interpretation of the results.
Potential conflicts of interest: None.
Funding/support: Preparation of this article was supported by research grants from the Manitoba Health Research Council (Dr Bolton), a University of Manitoba Graduate Fellowship (Ms Bhaskaran), a Canadian Institutes of Health Research New Investigator Award (Dr Bolton), and a Brain and Behavior Research Foundation NARSAD Young Investigator Award (Dr Bolton).
Role of the sponsor: The funding sources had no role in the design and conduct of the study; the collection, management, analysis, and interpretation of data; or the preparation, review, and approval of the manuscript.
Previous presentation: An abridged version of these results was presented at the following conferences: 31st conference of the European Health Psychology Annual Conference; August 28–29, 2017; Padua, Italy ▪ Canadian Psychological Association Annual Conference; June 8–10, 2017; Toronto, Canada ▪ Canadian Psychiatric Association Annual Conference; September 14–16, 2017; Ottawa, Ontario, Canada ▪ European Health Psychology Annual Conference; August 23–27, 2016; Aberdeen, United Kingdom.
Acknowledgments: The authors acknowledge Daniel Palitsky, MD; Cara Katz, MD; Will Husarewycz, BSc; Nina Cianflone; and Morgan Rathwell from the Department of Psychiatry, University of Manitoba, Winnipeg, Manitoba, Canada, for data entry and management. They report no conflicts of interest related to the subject of this study. The authors also acknowledge the residents in the Department of Psychiatry at the University of Manitoba for their help with data collection.
Additional information: The Suicide Assessment Form in Emergency Psychiatry (SAFE) database is part of a research program at the University of Manitoba in the Department of Psychiatry. The database is the property of the University of Manitoba and resides within the laboratory of the Manitoba Population Mental Health Research Group. Requests for access should be sent to the corresponding author, Dr Bolton.
REFERENCES
1. The World Health Organization. Mental health: suicide data. 2017. WHO website. www.who.int/mental_health/prevention/suicide/suicideprevent/en/. Accessed December 18, 2017.
2. Government of Canada Statistics. (2017). Leading causes of death, by sex (both sexes). Government of Canada, Statistics Canada website. http://www.statcan.gc.ca/tables-tableaux/sum-som/l01/cst01/hlth36a-eng.htm. November 16, 2017.
3. The World Health Organization. SUPRE (n.d): The WHO worldwide initiative for the prevention of suicide. WHO website. http://www.who.int/mental_health/management/en/SUPRE_flyer1.pdf?ua=1. Accessed December 18, 2017.
4. Jollant F, Bellivier F, Leboyer M, et al. Impaired decision making in suicide attempters. Am J Psychiatry. 2005;162(2):304–310. PubMed CrossRef
5. Nock MK, Park JM, Finn CT, et al. Measuring the suicidal mind: implicit cognition predicts suicidal behavior. Psychol Sci. 2010;21(4):511–517. PubMed CrossRef
6. Hawton K, van Heeringen K. Suicide. Lancet. 2009;373(9672):1372–1381. PubMed CrossRef
7. Wilcox HC, Arria AM, Caldeira KM, et al. Prevalence and predictors of persistent suicide ideation, plans, and attempts during college. J Affect Disord. 2010;127(1–3):287–294. PubMed CrossRef
8. Harriss L, Hawton K, Zahl D. Value of measuring suicidal intent in the assessment of people attending hospital following self-poisoning or self-injury. Br J Psychiatry. 2005;186(01):60–66. PubMed CrossRef
9. Sokero T, Leskela U, Rytsala H, et al. Risk factors for suicidal ideation and attempts among psychiatric patients with major depressive disorder. Eur Psychiatry. 2002;17:204. CrossRef
10. Kessler RC, Berglund P, Borges G, et al. Trends in suicide ideation, plans, gestures, and attempts in the United States, 1990–1992 to 2001–2003. JAMA. 2005;293(20):2487–2495. PubMed CrossRef
11. Nock MK, Borges G, Bromet EJ, et al. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–154. PubMed CrossRef
12. Lee J-I, Lee M-B, Liao S-C, et al. Prevalence of suicidal ideation and associated risk factors in the general population. J Formos Med Assoc. 2010;109(2):138–147. PubMed CrossRef
13. Ben-Zeev D, Young MA, Depp CA. Real-time predictors of suicidal ideation: mobile assessment of hospitalized depressed patients. Psychiatry Res. 2012;197(1–2):55–59. PubMed CrossRef
14. Jenkins GR, Hale R, Papanastassiou M, et al. Suicide rate 22 years after parasuicide: cohort study. BMJ. 2002;325(7373):1155. PubMed CrossRef
15. Borges G, Angst J, Nock MK, et al. Risk factors for the incidence and persistence of suicide-related outcomes: a 10-year follow-up study using the National Comorbidity Surveys. J Affect Disord. 2008;105(1–3):25–33. PubMed CrossRef
16. Kessler RC, Borges G, Walters EE. Prevalence of and risk factors for lifetime suicide attempts in the National Comorbidity Survey. Arch Gen Psychiatry. 1999;56(7):617–626. PubMed CrossRef
17. Nock MK, Borges G, Bromet EJ, et al. Cross-national prevalence and risk factors for suicidal ideation, plans and attempts. Br J Psychiatry. 2008;192(2):98–105. PubMed CrossRef
18. Jeon HJ, Lee J-Y, Lee YM, et al. Unplanned versus planned suicide attempters, precipitants, methods, and an association with mental disorders in a Korea-based community sample. J Affect Disord. 2010;127(1–3):274–280. PubMed CrossRef
19. Lewinsohn PM, Rohde P, Seeley JR. Adolescent suicidal ideation and attempts: prevalence, risk factors, and clinical implications. Clin Psychol Sci Pract. 1996;3(1):25–46. CrossRef
20. ten Have M, de Graaf R, van Dorsselaer S, et al. Incidence and course of suicidal ideation and suicide attempts in the general population. Can J Psychiatry. 2009;54(12):824–833. PubMed CrossRef
21. De Leo D, Cerin E, Spathonis K, et al. Lifetime risk of suicide ideation and attempts in an Australian community: prevalence, suicidal process, and help-seeking behaviour. J Affect Disord. 2005;86(2–3):215–224. PubMed CrossRef
22. Gaynes BN, West SL, Ford CA, et al; U.S. Preventive Services Task Force. Screening for suicide risk in adults: a summary of the evidence for the US Preventive Services Task Force. Ann Intern Med. 2004;140(10):822–835. PubMed CrossRef
23. Brown GK, Beck AT, Steer RA, et al. Risk factors for suicide in psychiatric outpatients: a 20-year prospective study. J Consult Clin Psychol. 2000;68(3):371–377. PubMed CrossRef
24. Valtonen HM, Suominen K, Sokero P, et al. How suicidal bipolar patients are depends on how suicidal ideation is defined. J Affect Disord. 2009;118(1-3):48–54. PubMed CrossRef
25. Isometsä ET, Lönnqvist JK. Suicide attempts preceding completed suicide. Br J Psychiatry. 1998;173(06):531–535. PubMed CrossRef
26. Gask L, Morriss R. Assessment and immediate management of people at risk of harming themselves. Psychiatry. 2009;8(7):241–245. CrossRef
27. Desseilles M, Perroud N, Guillaume S, et al. Is it valid to measure suicidal ideation by depression rating scales? J Affect Disord. 2012;136(3):398–404. PubMed CrossRef
28. Silverman MM, Berman AL, Sanddal ND, et al. Rebuilding the tower of Babel: a revised nomenclature for the study of suicide and suicidal behaviors, part 2: suicide-related ideations, communications, and behaviors. Suicide Life Threat Behav. 2007;37(3):264–277. PubMed CrossRef
29. O’Connor SS, Jobes DA, Yeargin MK, et al. A cross-sectional investigation of the suicidal spectrum: typologies of suicidality based on ambivalence about living and dying. Compr Psychiatry. 2012;53(5):461–467. PubMed CrossRef
30. Szanto K, Mulsant BH, Houck P, et al. Occurrence and course of suicidality during short-term treatment of late-life depression. Arch Gen Psychiatry. 2003;60(6):610–617. PubMed CrossRef
31. Menon V. Suicide risk assessment and formulation: an update. Asian J Psychiatr. 2013;6(5):430–435. PubMed CrossRef
32. Szanto K, Reynolds CF 3rd, Frank E, et al. Suicide in elderly depressed patients: is active vs passive suicidal ideation a clinically valid distinction? Am J Geriatr Psychiatry. 1996;4(3):197–207. PubMed CrossRef
33. Schulberg HC, Lee PW, Bruce ML, et al. Suicidal ideation and risk levels among primary care patients with uncomplicated depression. Ann Fam Med. 2005;3(6):523–528. PubMed CrossRef
34. Morgan HG, Stanton R. Suicide among psychiatric in-patients in a changing clinical scene. Suicidal ideation as a paramount index of short-term risk. Br J Psychiatry. 1997;171(6):561–563. PubMed CrossRef
35. Bruce G. How Winnipeggers Use the Emergency Room. Winnipeg Free Press website. www.winnipegfreepress.com/local/Why-do-we-go-to-the-ER-448276913. September 30, 2017.
36. Posner K, Oquendo MA, Gould M, et al. Columbia Classification Algorithm of Suicide Assessment (C-CASA): classification of suicidal events in the FDA’s pediatric suicidal risk analysis of antidepressants. Am J Psychiatry. 2007;164(7):1035–1043. PubMed CrossRef
37. SPSS Statistics [computer program]. Armonk, NY: IBM Corporation; 2012.
38. Turecki G, Brent DA. Suicide and suicidal behaviour. Lancet. 2016;387(10024):1227–1239. PubMed CrossRef
39. Brown GK, Steer RA, Henriques GR, et al. The internal struggle between the wish to die and the wish to live: a risk factor for suicide. Am J Psychiatry. 2005;162(10):1977–1979. PubMed CrossRef
40. Baca-Garcia E, Perez-Rodriguez MM, Oquendo MA, et al. Estimating risk for suicide attempt: are we asking the right questions? passive suicidal ideation as a marker for suicidal behavior. J Affect Disord. 2011;134(1–3):327–332. PubMed CrossRef
41. Sakinofsky I. The current evidence base for the clinical care of suicidal patients: strengths and weaknesses. Can J Psychiatry. 2007;52(suppl 1):
7S–20S. PubMed
42. Simon GE, Rutter CM, Peterson D, et al. Does response on the PHQ-9 Depression Questionnaire predict subsequent suicide attempt or suicide death? Psychiatr Serv. 2013;64(12):1195–1202. PubMed CrossRef
43. Beck AT, Kovacs M, Weissman A. Assessment of suicidal intention: the Scale for Suicide Ideation. J Consult Clin Psychol. 1979;47(2):343–352. PubMed CrossRef
44. Beck AT, Herman I, Schuyler D. Development of suicidal intent scales. In: Beck AT, Resnik HLP, Lettieri DJ, eds. The Prediction of Suicide. Bowie, MD: Charles Press; 1974a:45–56.
45. Statistics Canada. Aboriginal Peoples Survey, 2012; Lifetime Suicidal Thoughts among First Nations Living off Reserve, Métis and Inuit Aged 26 to 59: prevalence and associated characteristics. Statistics Canada, Government of Canada website. www150.statcan.gc.ca/n1/pub/89-653-x/89-653-x2016008-eng.htm. January 19, 2016.
Enjoy this premium PDF as part of your membership benefits!


