LESSONS LEARNED AT THE INTERFACE OF MEDICINE AND PSYCHIATRY
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2023;25(4):22f03471
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
In this report, we present the case of a 70-year-old woman who presented with symptoms of catatonia that were refractory to traditional treatment. She was found to have a cerebral venous sinus thrombosis (CVST), which most likely contributed to her presentation. Using this case, we examine potential neuro-medical etiologies of catatonia, as well as treatment options. Finally, we also discuss CVST and how it may affect both the diagnosis and treatment of catatonia. As catatonia is a complex condition, it is important to better understand how other neuro-medical conditions such as CVST may interact with and confound the treatment of catatonia in the general hospital.
Have you ever wondered what can cause an altered mental status with abnormal movements? Have you been uncertain about when and how to evaluate a patient with such signs and symptoms? Have you been perplexed by how to treat such an individual over the short and long term, especially when first-line treatments are ineffective or contraindicated? If you have, then the following case vignette and discussion should prove useful.
CASE VIGNETTE
Ms C, a 70-year-old woman, was admitted to a community hospital with headaches and myoclonic jerking and was transferred to a large tertiary academic medical center 1 week later when her mental status became altered and she developed severe hypertension (200/120 mm Hg).
On arrival to our emergency department (ED), she was awake, but essentially unresponsive to physical or verbal stimuli; she closed her eyes tightly with vigorous stimulation. Initial physical examination was notable for lead pipe rigidity. Episodically, she responded to “yes/no” questions. Initially, she was able to drink without difficulty and eat with staff assistance. She was labile and inappropriately tearful while watching television or when her name was called. She was minimally responsive to pain, made whimpering noises, manifested posturing, and was rigid. Given her recent history of myoclonus, a continuous electroencephalogram (EEG) was obtained.1 It demonstrated generalized slowing consistent with nonspecific encephalopathy. Neither seizure nor subclinical seizure activity was detected.
Her medical history was notable for the diagnosis of an adenocarcinoma (treated with a left lower lobectomy 4 years earlier) and a hemorrhagic infarct in the left frontoparietal lobe and right medial frontal lobe 2 years before this current admission that led to parkinsonian features (including a shuffling gait, impaired balance, and bradykinesia). Subsequently, she had a bladder stimulator placed to treat symptoms of urinary retention and was started on carbidopa-levodopa (37.5–150 mg by mouth 3 times daily). Her psychiatric history included only a remote history of anxiety and depression.
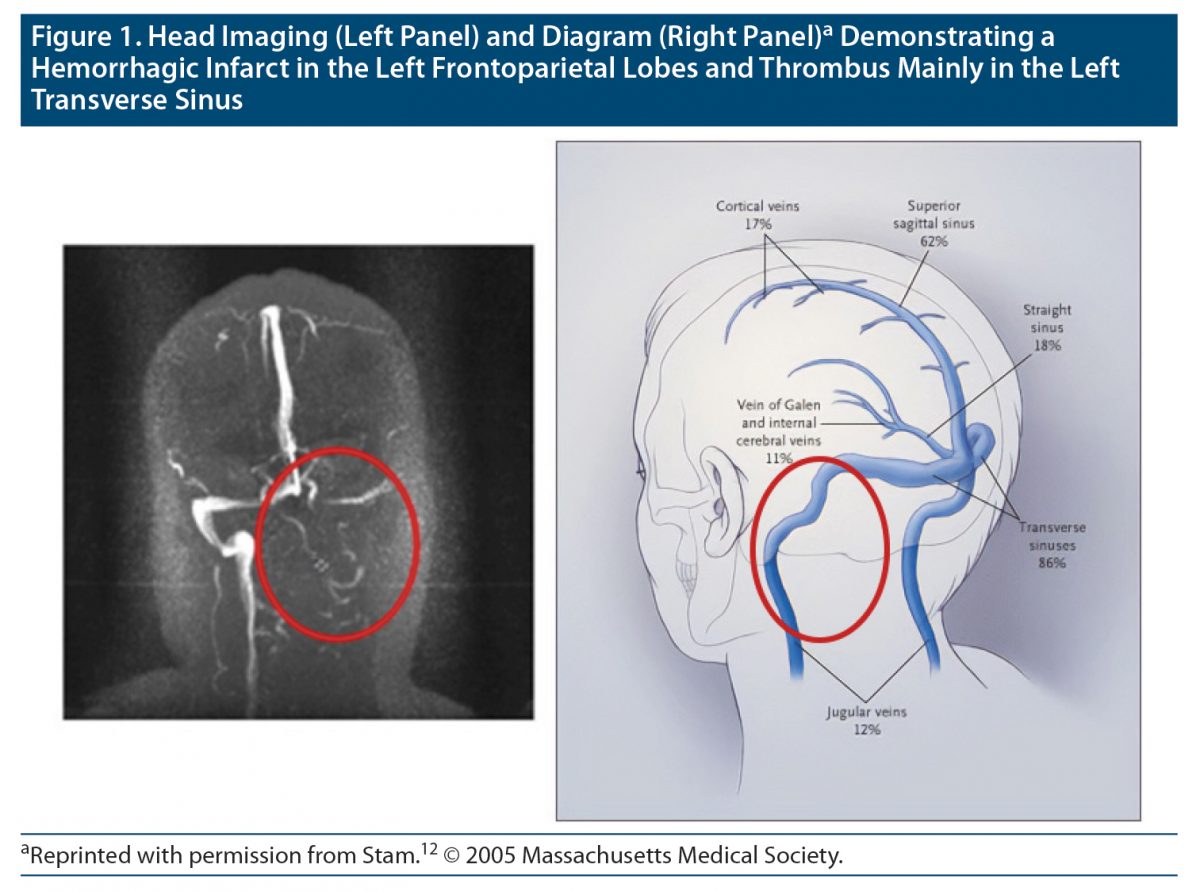
A head computed tomography (CT) scan revealed a subacute hemorrhagic infarct in the left frontoparietal lobe. Due to concerns regarding incompatibility with the patient’s bladder stimulator, a magnetic resonance imaging (MRI) scan was not initially obtained. Following medical clearance for MRI, a large dural venous sinus thrombosis occupying the left transverse and sigmoid sinuses was evident; however, there was no suggestion of autoimmune encephalitis. (Figure 1).
Due to Ms C’s history of stroke-associated parkinsonian features, her carbidopa-levodopa dosage was increased to 62.5–250 mg by mouth 4 times daily, but it was without clinical effect. This led the neurology team to think that undertreated Parkinson’s disease was unlikely.
Given her history of lung cancer, CT scans of her chest, abdomen, and pelvis were obtained, as was a paraneoplastic panel and a cerebrospinal fluid analysis via a lumbar puncture. Each of these tests was unrevealing for a paraneoplastic process or an occult malignancy, rendering the diagnosis of an autoimmune encephalitis unlikely. The neurology team ruled out the possibility of hemorrhagic stroke as an explanation for her presentation, given that there was no asymmetry found on the neurologic examination and that she failed to improve despite resolving imaging findings.
Ms C was placed on a heparin drip, and intravenous (IV) lorazepam was administered (initially at 0.5 mg 3 times daily and then increased up to 1.75 mg 3 times daily) for agitation and a presumptive diagnosis of catatonia. Over the next 2 weeks, her condition continued to deteriorate. She stopped eating and was unable to swallow pills; this required placement of a nasogastric tube. Owing to a lack of response to lorazepam and the team’s concern for worsening sedation, lorazepam was weaned and discontinued. Given that two-thirds of patients respond to lorazepam in primary catatonia, but that it is much less effective in secondary catatonia, we believed the diagnosis of catatonia was appropriate.2
Since several suspected causes of her presentation had been ruled out after a month-long hospital stay, the remaining most plausible diagnosis was of secondary catatonia associated with a subacute hemorrhagic stroke and CVST. Although electroconvulsive therapy (ECT) was considered, she failed to manifest malignant features of catatonia (such as elevated creatine phosphokinase [CPK] or fever), and the risk of cerebral edema associated with ECT in the setting of a hemorrhagic stroke and CVST was deemed too great. Over the next 3 weeks, her medical care was optimized with the addition of memantine (10 mg twice daily) followed by amantadine (100 mg daily), and an empiric 5-day course of methylprednisolone (1,000 mg)—though without a beneficial effect. Intravenous immunoglobulin (IVIG) and plasmapheresis were considered, but due to her tenuous condition, IVIG and plasmapheresis were ruled out as therapeutic options due to risk of clotting and bleeding, respectively. Infection risk from steroids was deemed to be the least unacceptable risk. Figure 2 demonstrates our treatment approach to Ms C’s catatonia.
What Is Catatonia, and How Is It Diagnosed?
Catatonia, now a well-described syndrome with motor and behavioral signs and symptoms, may be associated with a psychiatric condition (eg, major depressive disorder or schizophrenia) or be associated with a neuro-medical condition (eg, a seizure disorder or systemic lupus erythematosus).3 Catatonia can be further subtyped into stuporous or excited catatonia depending on the accompanying level of psychomotor activity (hypokinetic or hyperkinetic). Malignant catatonia is a potentially life-threatening subtype marked by the triad of fever, autonomic instability, and an elevated creatine kinase level.4 According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), 3 or more of the following must be present to make a diagnosis of catatonia, regardless of subtype: stupor, catalepsy, waxy flexibility, mutism, negativism, posturing, mannerism, stereotypy, agitation, grimacing, echolalia, or echopraxia—and while the criterion is controversial,4 it must not occur during an episode of delirium.5 A working diagnosis of catatonia is often made utilizing the Modified Bush-Francis Catatonia Rating Scale.6 While this scale was not used in the case of Ms C, she presented with numerous catatonic features (eg, grimacing, posturing, waxy flexibility, mutism, stupor, and agitation) with little variation in her symptoms throughout her hospital stay.
How Is Catatonia Usually Treated?
Treatment of catatonia should be tailored to its underlying etiology,7 since patients with neuro-medically induced catatonia may not respond as well to treatment with benzodiazepines.8,9 The first-line treatment for neuro-medical catatonia is to address the underlying medical condition and treat any remaining catatonic features with a benzodiazepine or, in malignant or resistant cases, ECT.10 While underlying causes of secondary catatonia should be addressed, the first-line treatment for all forms of catatonia is lorazepam.11 Though not approved by the US Food and Drug Administration (FDA) for this purpose, a typical starting dose is often higher than that used for other indications—on the order of 2 mg IV—often with an immediate and dramatic response. However, if symptoms persist beyond 5 days or malignant features are observed, ECT is considered as the definitive and most effective treatment. It should be noted that abrupt discontinuation of certain medications, such as antipsychotics, could precipitate catatonia in patients who have been prescribed and are taking these medications for an extended period. Other medications that have been trialed with some success include amantadine, memantine, topiramate, and zolpidem.4
What Is CVST, and How Is It Diagnosed?
CVST is a rare condition often with a nonspecific presentation; however, severe headache is the most common presenting symptom.11 If it is recognized and treated promptly, the prognosis is favorable. CVST is readily diagnosed with neuroimaging techniques, including MRI or CT venography, and is generally treated with systemic anticoagulation and management of the underlying cause. Our patient, Ms C, had chronic impairments of balance and ambulation over several years, which limited her mobility and raised her risk for hypercoagulability. CVST is seen more commonly in women, likely due to the elevated coagulation risk of oral contraceptives and pregnancy.12
How Does CVST Alter the Treatment of Catatonia?
While the underlying CVST and hemorrhagic stroke that likely contributed to Ms C’s catatonia were being addressed by heparin, methylprednisolone, and consideration of IVIG and plasmapheresis, the treatment team also attempted to alleviate her catatonic symptoms. Catatonia involves basal ganglia neural network interactions with the cortex and thalamus. These impairments have been shown to extend to prefrontal, orbitofrontal, and parietal cortices in neuroimaging studies.4 The main neurotransmitters responsible for impairments in these networks are decreased activity of γ-aminobutyric acid A (GABAA), decreased activity of dopamine D2 receptors, and increased N-methyl-d-aspartate (NMDA) receptors.4,9,13 Given this information, our initial treatment with lorazepam aimed to address the decreased GABAA activity. When that trial failed, we added memantine and amantadine, which we hoped would alleviate symptoms by increasing dopamine transmission in the striatum and also decreasing glutamate in the striatum.14,15 It is ultimately unclear what agent or process led to a reduction in her symptoms, or to what extent her history of parkinsonian symptoms and treatment with dopamine agonists may have uniquely influenced her presentation or response to treatment. It is possible that the combination of slow thrombus resorption along with the brain’s dynamic ability to restore neural networks and decrease local neuroinflammation could explain the seemingly spontaneous improvement of her catatonic presentation.
An additional MRI scan obtained 2 weeks before discharge failed to demonstrate a significant resolution of the thrombus. Remarkably, 1 day prior to her hospital discharge Ms C became more responsive and was able to interact and answer questions. At discharge, she was oriented to self, but she still required reorientation to location, time, and situation with no apparent memory of the previous events. In collaboration with her family and the neurology team, she was administered anticoagulant medication with a plan to reimage her in several months and to monitor her for CVST resolution and ongoing catatonic symptom evolution.
Diagnostic Clarification
When considering a diagnosis of catatonia, several disease processes must be considered. Delirium will top the differential of every patient, but in the case of Ms C, parkinsonism was also considered.
Delirium is characterized by a waxing and waning course as well as by impaired attention and awareness.16 There is a marked reduction in the ability to sustain, redirect, and focus attention. There are also additional cognitive deficits, notably of memory, language, and perception. The pathophysiology of the condition is based on hypoactivity of the cholinergic system. Delirium is most common in those with advanced age, an infection, or use of myriad medications. Like with catatonia, there are hypoactive and hyperactive subtypes that can present with a wide range of symptoms, such as perplexity, increased sympathetic activity, and emotional dysregulation. Unlike with catatonia, the presentation does not persist throughout the day. Serial examinations show a fluctuating course throughout a hospitalization. That is not the case with catatonia. Without intervention, the symptoms of a catatonic person will persist.
Parkinsonism was another condition under consideration for our patient. Parkinsonism is caused by an impairment in the dopaminergic transmission of the D2 receptor. This disruption is most commonly in the striatum and changes the output of the basal ganglia–thalamocortical system. The cause of parkinsonism can be idiopathic, secondary to a medical condition (such as stroke), or, most commonly, due to a medication side effect. The most prominent symptoms reflect the physical symptoms of catatonia, such as rigidity and bradykinesia. Resting tremor is a symptom that is common in parkinsonism and would increase the likelihood of this condition over catatonia if present. A thorough review of medications should be conducted to determine if medication could be contributing to these physical symptoms. Medications that most commonly cause parkinsonism are antipsychotics, antiemetics, and dopamine-depleting agents such as tetrabenazine, deutetrabenazine, and valbenazine.
CONCLUSION
Ms C presented with CVST and catatonia but without systemic lupus erythematosus (SLE) or a recognizable autoimmune encephalitis. This is an infrequently reported combination, and it is not a widely reported potential neuro-medical cause of catatonia. One case report from de Figueiredo et al17 described a patient with catatonic symptoms who was later found to have had a CVST in the left transverse sinus but who was suspected of having a co-occurring seizure. The patient was given phenytoin with complete remission of behavioral and catatonic symptoms. Another report,18 of a patient with SLE, had a hypercoagulable state and a consequent CVST that induced catatonic symptoms. A CVST on imaging was found in the left transverse sinus. That patient was already being treated with lorazepam for an anxiety disorder. Resolution of her catatonic symptoms occurred after administration of heparin. Authors of that study noted the importance of imaging when other causes of catatonia cannot be found.18 Another report19 described an 18-year-old who presented with the sudden onset of restlessness, altered behavior, stereotyped movements, insomnia, semimutism, and negativism who had a partial response to lorazepam. Imaging showed an upper, transverse, and sigmoid right sagittal sinus thrombosis. Resolution of symptoms occurred with anticoagulant therapy.19 One additional case20 raised concern for catatonia with CVST; however, the patient died, and no further workup or resolution of symptoms could be achieved.
In acute medical and surgical settings, more than half of the cases of catatonia are of neuro-medical, rather than primary psychiatric, origin.21,22 Over two-thirds of these cases involve central nervous system (CNS)–specific diseases.21 Additionally, catatonia may mimic other diagnoses—especially when it is secondary to a medical condition. Ms C’s lack of SLE, and thus lupus cerebritis, or autoimmune encephalitis with a presentation consistent with the sparse literature, lends evidence that CVST may be a rare etiology of catatonia. If a secondary (nonpsychiatric) etiology of catatonia is suspected, a neuro-medical workup (including head imaging) is typically warranted, and depending on the clinical suspicion, we suggest ruling out CVST.
Article Information
Published Online: August 3, 2023. https://doi.org/10.4088/PCC.22f03471
© 2023 Physicians Postgraduate Press, Inc.
Submitted: December 19, 2022; accepted March 21, 2023.
To Cite: Gardner SM, Pavisian B, Ho PA, et al. Dynamic evolution of catatonia in the context of cerebral venous sinus thrombosis. Prim Care Companion CNS Disord. 2023;25(4):22f03471.
Author Affiliations: The Ohio State University College of Medicine, Columbus, Ohio (Gardner); Now with the Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati Medical Center/College of Medicine, Cincinnati, Ohio (Gardner); The Ohio State University Department of Psychiatry and Behavioral Health, Columbus, Ohio (Pavisian, Kasick); Department of Psychiatry, Geisel School of Medicine at Dartmouth, Lebanon, New Hampshire (Ho, Rustad); Department of Psychiatry, Larner College of Medicine at the University of Vermont, Burlington (Rustad); Department of Mental Health and Behavioral Sciences, White River Junction VA Medical Center, White River Junction, Vermont (Rustad); Department of Psychiatry, Massachusetts General Hospital and Harvard Medical School, Boston, Massachusetts (Stern).
Corresponding Author: Spencer M. Gardner, MD, MS, University of Cincinnati College of Medicine, Department of Psychiatry, 260 Stetson St, Suite 3200, Cincinnati, OH 45267 ([email protected]).
Relevant Financial Relationships: Dr Stern has received royalties from Elsevier for editing textbooks on psychiatry. No other authors have conflicts of interest to disclose.
Funding/Support: There are no funding sources for this manuscript.
Clinical Points
- Catatonia is a complex and easily overlooked but life-threatening syndrome.
- Clinicians should be vigilant for neuro-medical etiologies of catatonia, as more than half of the cases of catatonia are not psychiatric in origin and over two-thirds of neuro-medical catatonia cases involve a central nervous system (CNS)–specific disease.
- The first-line treatment for neuro-medical catatonia is to address the underlying medical condition and treat any remaining catatonic features with benzodiazepines or, in malignant or resistant cases, electroconvulsive therapy (ECT). However, benzodiazepines are often ineffective in cases of neuro-medical catatonia, and ECT is often contraindicated in complicated neuro-medical cases (eg, stroke) due to the risk of inducing cerebral edema.
References (22)

- Restrepo D, Kochav J, Goodheart AE, et al. The importance of identifying myoclonus in the setting of mental status abnormalities: differential diagnosis and treatment. Prim Care Companion CNS Disord. 2016;18(5). PubMed CrossRef
- Raffin M, Zugaj-Bensaou L, Bodeau N, et al. Treatment use in a prospective naturalistic cohort of children and adolescents with catatonia. Eur Child Adolesc Psychiatry. 2015;24(4):441–449. PubMed CrossRef
- Carroll BT, Anfinson TJ, Kennedy JC, et al. Catatonic disorder due to general medical conditions. J Neuropsychiatry Clin Neurosci. 1994;6(2):122–133. PubMed CrossRef
- Stern TA, Freudenreich O, Smith F, et al. The Massachusetts General Hospital Handbook of General Hospital Psychiatry. Seventh. Elsevier; 2017.
- Schizophrenia Spectrum and Other Psychotic Disorders. In: Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association Publishing; 2022:87–122. Accessed December 7, 2022. https://dsm.psychiatryonline.org/doi/epdf/10.1176/appi.books.9780890425596
- Bush G, Fink M, Petrides G, et al. Catatonia, I: rating scale and standardized examination. Acta Psychiatr Scand. 1996;93(2):129–136. PubMed CrossRef
- Pelzer AC, van der Heijden FM, den Boer E. Systematic review of catatonia treatment. Neuropsychiatr Dis Treat. 2018;14:317–326. PubMed CrossRef
- Rosebush PI, Hildebrand AM, Furlong BG, et al. Catatonic syndrome in a general psychiatric inpatient population: frequency, clinical presentation, and response to lorazepam. J Clin Psychiatry. 1990;51(9):357–362. PubMed
- Beach SR, Gomez-Bernal F, Huffman JC, et al. Alternative treatment strategies for catatonia: a systematic review. Gen Hosp Psychiatry. 2017;48:1–19. PubMed CrossRef
- Gross AF, Smith FA, Stern TA. Dread complications of catatonia: a case discussion and review of the literature. Prim Care Companion J Clin Psychiatry. 2008;10(2):153–155. PubMed CrossRef
- Saposnik G, Barinagarrementeria F, Brown RD Jr, et al; American Heart Association Stroke Council and the Council on Epidemiology and Prevention. Diagnosis and management of cerebral venous thrombosis: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke. 2011;42(4):1158–1192. PubMed CrossRef
- Stam J. Thrombosis of the cerebral veins and sinuses. N Engl J Med. 2005;352(17):1791–1798. PubMed CrossRef
- Rustad JK, Landsman HS, Ivkovic A, et al. Catatonia: an approach to diagnosis and treatment. Prim Care Companion CNS Disord. 2018;20(1):17f02202. PubMed CrossRef
- Peeters M, Maloteaux JM, Hermans E. Distinct effects of amantadine and memantine on dopaminergic transmission in the rat striatum. Neurosci Lett. 2003;343(3):205–209. PubMed CrossRef
- Carpenter SS, Hatchett AD, Fuller MA. Catatonic schizophrenia and the use of memantine. Ann Pharmacother. 2006;40(2):344–346. PubMed CrossRef
- Oldham MA, Lee HB. Catatonia vis-à-vis delirium: the significance of recognizing catatonia in altered mental status. Gen Hosp Psychiatry. 2015;37(6):554–559. PubMed CrossRef
- de Figueiredo NSV, Angst DBM, Lima Neto AM, et al. Catatonia, beyond a psychiatric syndrome. Dement Neuropsychol. 2017;11(2):209–212. PubMed CrossRef
- Butala J, Swanson G, Chopra A. Catatonia as a manifestation of cerebral venous sinus thrombosis. Prim Care Companion CNS Disord. 2018;20(1):17l02148. PubMed CrossRef
- Orihuela PO, Morenilla ALP, González CH. Report of clinical case: catatonic symptoms as a result of cerebral venous sinus thrombosis. Eur Psychiatry. 2017;41(S1):S500. CrossRef
- Gangadhar BN, Keshavan MS, Goswami U, et al. Cortical venous thrombosis presenting as catatonia: a clinicopathologic report. J Clin Psychiatry. 1983;44(3):109–110. PubMed
- Oldham MA. The probability that catatonia in the hospital has a medical cause and the relative proportions of its causes: a systematic review. Psychosomatics. 2018;59(4):333–340. PubMed CrossRef
- Jaimes-Albornoz W, Serra-Mestres J. Prevalence and clinical correlations of catatonia in older adults referred to a liaison psychiatry service in a general hospital. Gen Hosp Psychiatry. 2013;35(5):512–516. PubMed CrossRef
Please sign in or purchase this PDF for $40.

