The coexistence of focal and generalized epilepsies, such as mesial temporal sclerosis (MTS) and juvenile myoclonic epilepsy (JME), is uncommon but clinically relevant. We present a rare case of a 27-year-old man with the coexistence of right MTS and JME, who initially exhibited bilateral tonic-clonic seizures preceded by focal psychic auras. This case underscores the diagnostic and therapeutic challenges in dual epilepsy syndromes, emphasizing the importance of individualized, multidisciplinary management.
Case Report
A 27-year-old man presented with generalized tonic-clonic seizures preceded by focal psychic auras. His medical history included a febrile convulsion at age 14 months. Cranial magnetic resonance imaging demonstrated right hippocampal atrophy consistent with MTS. Cranial positron emission tomography revealed hypometabolism in the right mesial temporal area. He was taking levetiracetam, carbamazepine, and valproic acid.
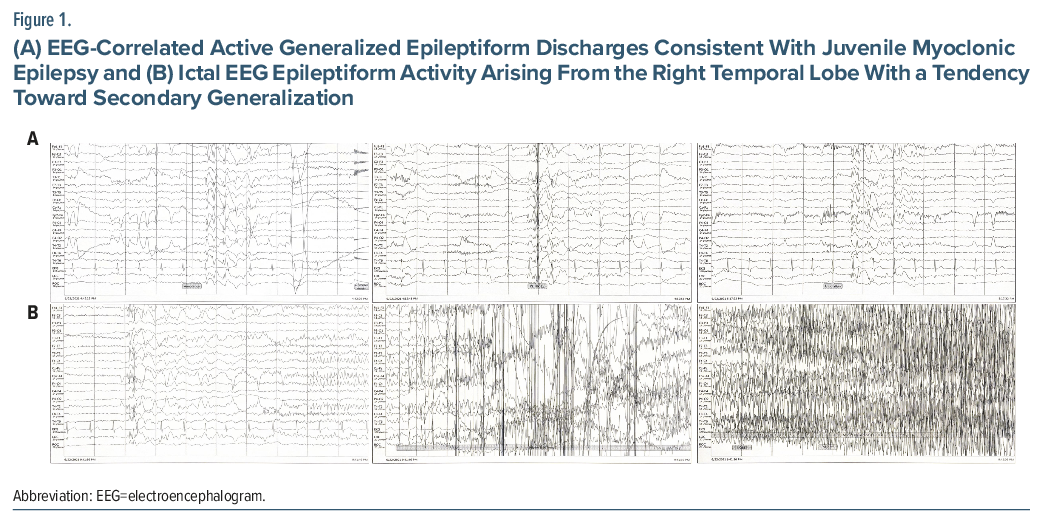
When the patient was admitted for preoperative video electroencephalogram (EEG) monitoring, medication doses were reduced, and seizures originating in the right temporal lobe and then secondarily generalized were recorded. However, as medication doses were further reduced, especially the dose of valproic acid, EEG recordings were obtained that clinically showed myoclonus and electrophysiologically demonstrated generalized epileptiform discharges compatible with JME (Figure 1A-B). Despite medical therapy, seizures persisted, and right temporal lobectomy was performed. Histopathology confirmed MTS. Following surgery, focal seizures were resolved. Postoperatively, apart from seizures triggered by infection, the patient may have rare myoclonic jerks in the hands. He continues regular neurological follow-up.
Discussion
MTS is a frequent cause of drug-resistant temporal lobe epilepsy (TLE), often associated with a history of febrile seizures.1 Clinical features typically include focal seizures with and without impaired awareness, often preceded by auras such as deja vu, jamais vu, fear, or epigastric sensations.2 This aligns with our patient’s reported prodromal psychic symptoms. Temporal lobe resection often results in favorable outcomes, with seizure control achieved in 70%–90% of cases.3 Conversely, JME is an idiopathic generalized epilepsy syndrome emerging in adolescence, characterized by myoclonic, generalized tonic-clonic, and absence seizures.4
In a PubMed database review in October 2024, we found only 7 publications on TLE and idiopathic generalized epilepsy coexistence.5–11 In one study, only 4 of 4,277 registered patients showed definite coexistence of TLE and idiopathic generalized epilepsy (IGE) (0.1% of all epilepsies [N = 3,760]; 95% CI, 0.0001–0.0021), with 2 of those patients specifically diagnosed with JME and TLE, 1 with left amygdala enlargement and 1 with right hippocampal sclerosis.5 In a cohort study of 664 patients who underwent anterior temporal lobectomy for drug-resistant TLE, 12 (1.8%) were found to have coexisting IGE. Notably, IGE was diagnosed preoperatively in only 5 patients, while the majority exhibited electroclinical features of IGE during postoperative follow-up.9 In another study of 350 temporal lobe resected patients, 1 case was similar to our patient with the coexistence of JME and TLE. However, that patient had clinical onset of JME after the surgical resolution of his partial seizures, which had been foreshadowed for at least 5 years by subclinical spontaneous and photically induced generalized spikewave discharges.8 Other reports describe focal epilepsy developing later in patients with preexisting childhood-onset IGE.6,7,10,11
The recognition of both syndromes is critical for guiding therapy, as surgical resection can resolve focal seizures but not generalized myoclonic activity. This case emphasizes comprehensive diagnostic evaluation including EEG, neuroimaging, and multidisciplinary management to optimize outcomes in complex epilepsy presentations.
Article Information
Published Online: March 26, 2026. https://doi.org/10.4088/PCC.25cr04138
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04138
Submitted: November 12, 2025; accepted December 29, 2025.
To Cite: Mengeliboga B, Ucar MB, Midi I. Coexistence of mesial temporal sclerosis and juvenile myoclonic epilepsy. Prim Care Companion CNS Disord 2026;28(2):25cr04138.
Author Affiliations: Faculty of Medicine, Istanbul Okan University, Istanbul, Turkey (Mengeliboga); Department of Neurology, Marmara University School of Medicine, Istanbul, Turkey (Ucar, Midi).
Corresponding Author: Ipek Midi, MD, Fevzi Çakmak Mh. No:10 34899, Pendik, Istanbul, Turkey ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was obtained from the patient to publish the case report, and information has been de-identified to protect patient anonymity.
ORCID: Bariscan Mengeliboga: https://orcid.org/0009-0004-9027-1062; Merve B. Ucar: https://orcid.org/0009-0003-1319-2048; Ipek Midi: https://orcid.org/0000-0002-5125-3708
References (11)

- Liu Z, Mikati M, Holmes GL. Mesial temporal sclerosis: pathogenesis and significance. Pediatr Neurol. 1995;12(1):5–16. PubMed CrossRef
- Mbaba AN, Ogolodom MP, Abam R, et al. Mesial temporal sclerosis and epilepsy-a case report. Health Sci J. 2019;13(2):645.
- Mesial Temporal Sclerosis | American Journal of Neuroradiology. https://www.ajnr.org/ajnr-case-collections-diagnosis/mesial-temporal-sclerosis.
- Grünewald RA, Panayiotopoulos CP. Juvenile myoclonic epilepsy. Archives Neurology. 1993;50(6):594–598. PubMed CrossRef
- Asadi-Pooya AA, Malekpour M, Taherifard E, et al. Coexistence of temporal lobe epilepsy and idiopathic generalized epilepsy. Epilepsy Behav. 2023;151:109602. PubMed CrossRef
- Lie OV, Holmes MD. Late-onset temporal lobe epilepsy in a patient with juvenile myoclonic epilepsy. Epileptic Disord. 2012;14(2):190–194. PubMed CrossRef
- Khaing M, Lim K, Tan C. Focal epilepsy recruiting a generalised network of juvenile myoclonic epilepsy: a case report. Epileptic Disord. 2014;16(3):370–374. PubMed CrossRef
- Koutroumanidis M, Hennessy MJ, Elwes RDC, et al. Coexistence of temporal lobe and idiopathic generalized epilepsies. Neurology. 1999;53(3):490–495. PubMed CrossRef
- Radhakrishnan A, Menon RN, Radhakrishnan K. Coexistence of idiopathic generalized epilepsy among surgically treated patients with drug-resistant temporal lobe epilepsy. Epilepsy Res. 2011;96(1-2):151–157. PubMed CrossRef
- Enatsu R, Wyllie E, Kotagal P, et al. Surgically proven coexistence of focal and generalized epilepsy: a case report. Epilepsy Behav. 2012;26(1):61–63. PubMed CrossRef
- Ladino LD, Gleadow A, Téllez-Zenteno JF. A unique ictal EEG pattern in a patient with the coexistence of generalized and focal epilepsy. Clin EEG Neurosci. 2014;46(2):136–141. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!