ABSTRACT
Objective: To produce a qualitative description of the impact of moral injury on medical providers during the COVID-19 pandemic.
Methods: A convergent mixed-methods study design was used to explore experiences of health care workers during the first 12 months of the COVID-19 pandemic. Participants completed the Moral Injury Symptom Scale-HP (MISS-HP) and a 60-minute interview, in which they described their work experiences from March 2020 through January 2021. The study was conducted between May 2021 and August 2021.
Results: Eight physicians and 6 nurses were interviewed. Most participants (71%) worked in the emergency department, while 29% worked in the medical intensive care unit (MICU). MISS-HP scores were 49 on average and ranged from 29 to 73. Among the demographic groups, MICU participants scored the highest (56) and men scored the lowest (40). There were no significant differences in scores between any demographic group. The analysis of interview data showed how omissions and commissions in one’s professional duties created internal conflicts, which were inextricably linked to a deeper sense of feelings of guilt and blame around experiences of betraying or being betrayed and an inability to uphold one’s moral values.
Conclusions: The pandemic upended a previously reliable and imperceptible experience of a background of safety, in which the provision of both material resources and human presence was expected without question. Future directions generated from this study might examine the role of dependency on leadership structures and relationships with self and others that create the conditions for moral injury.
Prim Care Companion CNS Disord 2024;26(1):23m03651
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
During the COVID-19 pandemic, health care workers faced enormous pressures to fulfill their professional duties, safeguard the health of their loved ones, and maintain their own safety while deaths and hospitalizations rose around the world.1 Government mandates and recommendations, public opinion, and, perhaps most impactfully, a sense of personal risk overwhelmed the already difficult balance of patient-centric decision-making and hospital-centric priorities.2,3
Coined by psychiatrist Jonathan Shay, moral injury describes the distress experienced when someone’s sense of moral rightness is “betrayed” by leadership structures in situations involving great risk and consequence.4,5 The morally injurious act “transgress[es] deeply held moral beliefs and expectations”6(p700) about right/wrong and personal goodness,7 undermining one’s sense of personal integrity. Moral injury was conceptualized to distinguish experiences of trauma from those of moral dilemma, differentiating between the fear-based distress of posttraumatic stress disorder and the emotions arising from moral injury.7 While the traumatic event and the morally injurious one may often be the same, this distinction is particularly useful in describing the experiences of populations who may not struggle with posttraumatic distress. As experienced among health care workers, moral injury refers to “the challenge of simultaneously knowing what care patients need [while] being unable to provide it due to constraints that are beyond a provider’s control.”8(p401)
When moral injury is left unaddressed, providers face increased risk of professional burnout and trauma-related symptoms, as well as anxiety, depression, and posttraumatic stress disorder.6 The primary aim of this study was to qualitatively describe the impact of moral injury on medical providers during the COVID-19 pandemic. Our secondary aim was the collection of ethnographic data to identify variables and risk factors for future investigation of moral injury among medical providers.
METHODS
The study employed a convergent mixed-methods study design to explore experiences of health care workers during the first 12 months of the COVID-19 pandemic at a hospital in New York City. Participants (nurses and physicians) completed surveys, which included demographic details and the Moral Injury Symptoms Scale for Healthcare Professionals (MISS-HP).9 The MISS-HP, a validated scale assessing moral injury for health care professionals, comprises 10 items and produces a score from 10 to 100. A score ≥ 36 has an 86% sensitivity and 93% specificity for moral injury symptoms that cause moderate to severe functional impairments within family, social, or occupational domains.9
We obtained informed consent to interview each participant once about their experiences from March 2020 through January 2021 while employed as a health care professional (Supplementary Appendix A). Each interview took place over video, lasted approximately 60 minutes, and was carried out between May 2021 and August 2021. Study size was informed by data saturation, information power, and analytic and data sufficiency.10 Each transcript was read line-by-line within a day or 2 of the interview’s completion and transcription. The transcripts were then coded by 3 coders (G.A., Y.R.E., C.L.). To ensure internal validity of the data interpretation, the coders met to review and resolve any discrepancies. A secondary coding team (B.H.H., R.S., S.R.Z.) reviewed emerging codes twice per month to provide big picture feedback and resolve coding discrepancies. The codes were generated in an iterative process.
Descriptive statistics were used to characterize the study sample with respect to demographic variables and survey score. Categorical variables are represented as frequency (%), and continuous variables are represented as median (interquartile range). The χ2/Fisher exact test was used to examine the association between frequency of umbrella codes discussed and demographic groups of interest. All P values are 2-sided with statistical significance evaluated at the .05 α level. Qualtrics (IBM, Armonk, New York) was used for survey response collection, and R Version 4.2.1 (R Foundation for Statistical Computing, Vienna, Austria) was used for analysis.
RESULTS
Demographics
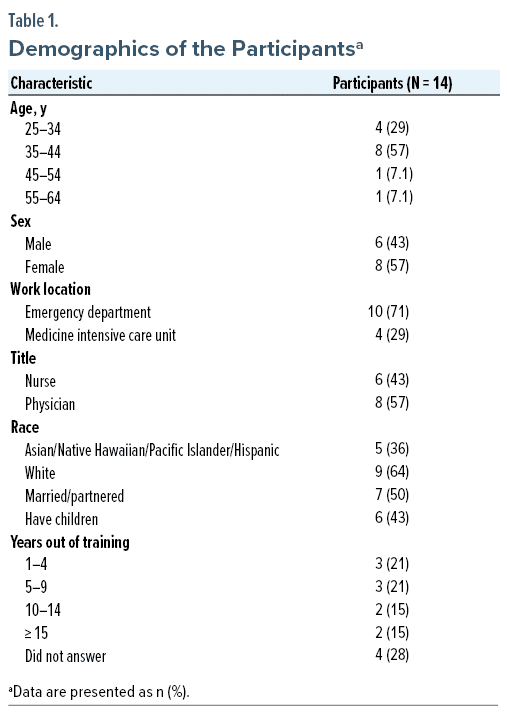
We interviewed 8 physicians and 6 nurses from the medical intensive care unit (MICU) and emergency department (ED). Most of the participants were between the ages of 35 and 44 years (57%); 43% identified as men, and 57% identified as women. Most participants (71%) worked in the ED, while the remaining 29% worked in the Department of Medicine (Table 1). Furthermore, 36% identified as Asian/Native Hawaiian/Pacific Islander or Hispanic, and 64% identified as White. About half of the participants were married or partnered, and 43% had children.
Qualitative Results
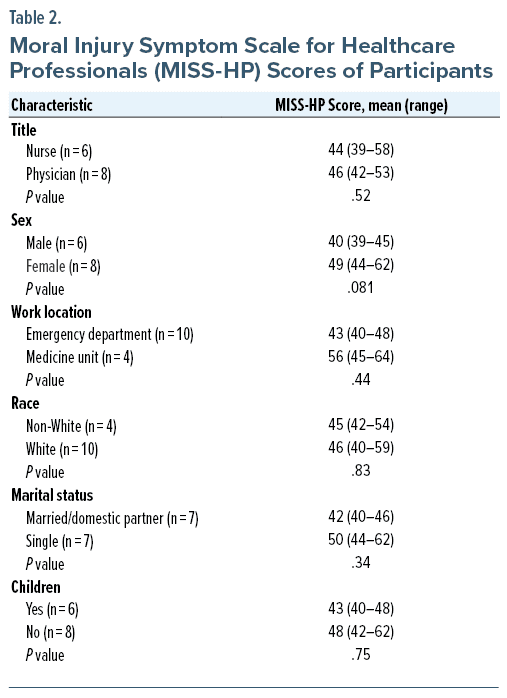
MISS-HP scores were 49 on average and ranged from 29 to 73. Among the demographic groups, MICU providers scored the highest (56), and men scored the lowest (40) (Table 2). There were no significant differences in scores between groups of women versus men, being partnered versus not, having children versus not, working in the MICU versus working in the ED, nurse versus physician, or non-White versus White. Half the respondents endorsed that experiences of moral injury had “moderately” or “very much” impaired their social or professional life, while half stated it had “not at all” or “mildly” affected them.
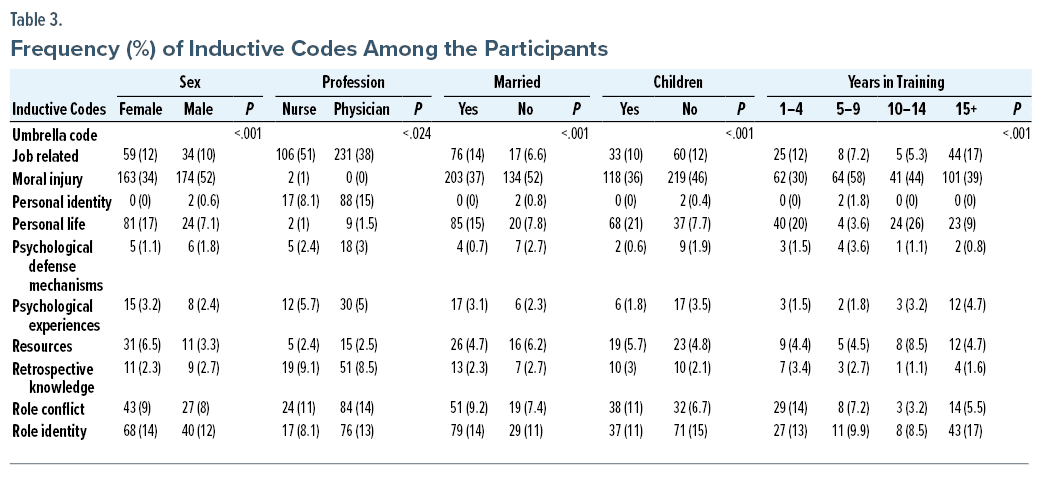
A total of 10 umbrella themes were coded, which included the following: job related, moral injury, personal identity, personal life, psychological defense mechanisms, psychological experiences, resources, retrospective knowledge, role conflict, and role identity. Participants aged 25–34 years and 55–64 years discussed moral injury more in comparison to those aged 35–54 years as measured by frequency of codes per interview (Table 3). Moral injury was also discussed more (as measured by frequency of codes) by men (52%) than women (34%), whereas personal life was discussed more by women (17%) versus men (7%). Regarding differences between professions, moral injury was discussed more by nurses (51%) than physicians (38%).
Interview Themes
Moral challenges in our participants often manifested through omissions and commissions—the actions that fail to align with or violate, respectively, one’s moral values.11 These actions can result in feelings of helplessness, guilt, and shame among health care workers.12 Though these emotions arise from conflict, they also ground and clarify a sense of identity, ie, “who I am” and “what I stand for.”
Omission, Unequal Exposures, and Guilt. Many participants observed inconsistencies in experiences of risk from hospital to hospital, between departments, and among colleagues. These discrepancies were challenging to accept whether one felt less exposed or more exposed. Guilt typically manifested in the context of recognizing one’s own position of being more protected from the risks of exposure that others endured. This guilt was often experienced as omission—a sense of doing less (by facing less exposure) than others were. It was common for participants to defend against these feelings of guilt by declaring their willingness to do more, if only they were not held back from this option or if only they had the opportunity.
Why aren’t we being redeployed anywhere? Redeploy us to the ICU. Redeploy us to the floor. . .Why are we sitting here . . . and there are bodies piling up [elsewhere]?
I felt sort of guilty that like we had [all these empty beds] . . . I should have just rented a bus and driven over [to other hospitals] and been like, come over!
This psychological defense preserves the health care worker’s sense of their own capability, integrity, and commitment to their values and responsibilities despite a more pervasive sense of helplessness and perhaps a deeper denial of fear. Others were able to acknowledge the relief that accompanied their sense of guilt for not being in more exposed positions.
[Hospital leadership] made it too easy for me to do my job. . . . I’m grateful, but we have colleagues [elsewhere who] were doing CPR all night long.
The nurses were starting lines and doing procedures and getting up close and personal. They were the ones going into the rooms, and the docs would just write the orders and say, “Alright, carry on.” You would try to minimize your risk and try to survive.
The problem is you see the paramedics bringing patients in, and [they] had minimal protection and were being exposed 10 times more than we were. They were braver colleagues than I who were better at spending time with [patients].
Of course, many participants also experienced the indignation and anger of the other side of this dynamic, as they recognized they were themselves at greater risk of exposure than others.
What was really jarring was the anesthesiologists who do the intubations had the most insane protective equipment [because they’re at the highest risk of exposure]. And I was like, “Well, where am I? I’m literally right next to you pushing your induction meds.” I’m in my [mask] that’s been reused many times. . . . “Why are you getting all this stuff, and I’m in this room right next to you as you’re saying how exposed you are? I’m right next to you?” It isn’t fair.
Perhaps the deepest experiences of guilt expressed by participants were associated with not providing the level of care they were accustomed to due to the overwhelming volume of critically ill patients, initial lack of knowledge about the virus, and lack of treatment availability. These restricting circumstances were, of course, experienced across the country and felt intensely by our participants during the pandemic’s initial impact in New York City.
You’re used to treating [your job] with a certain respect and [performing] at a certain level. Now, I go into work, and I have 4 of the sickest patients that there could possibly be in a hospital when I usually have 2 at most, and [you just] give these meds and basically [try to] keep them alive. Don’t [try to] make them better, because you can’t. Don’t provide them with the care that you would if you had the time. Just go in there, make sure you’re not killing them, and make sure they’re not dead.
The lack of accurate understanding about COVID transmission and prevention compounded the fear of COVID among health care professionals, as it also did in society at large early in the pandemic. Paralleling anxieties among the public, health care workers also found themselves avoiding physical contact and minimizing time with patients and colleagues. They were torn between the guilt of not meeting the usual standards of care and feeling that to do so would not do much more than put themselves in danger. Some felt there was an understandable rationale to avoiding prolonged or frequent contact with potentially exposed patients with minimal loss of clinical benefit. Others struggled with the irrelevance or futility of previous clinical norms and standards such as physical examinations and other close contact that began to feel questionably helpful and potentially dangerous. They felt torn about following or not following standards that, at best, had lost meaning, and at worst, could seem to cause more suffering to patients or staff.
Obviously, you don’t want to do any harm, but is it really useful for me to listen to their lungs and to get physically close to them?
The younger [physicians] would continue [CPR], and the nurses would be freaked, they can’t say no. They would be like, “Why the hell did we go on for half an hour doing this?” And, so, you’re trying to find the appropriate and ethical sweet spot.
Commissions. Lack of action was described as repeated commissions of what felt like betrayals to their patients in not meeting previous standards of care or treatment.
I felt like I was like being deceptive; I wouldn’t want to do this to my grandma, not only from an intubation standpoint, but to put her in some room where she’s just going to die by herself, and we don’t know what’s happening because we have shitty vent[ilator]s. She’s just going to die, but sure, I’ll intubate her.
I was mad at myself because I made a lot of promises to [patients] that I don’t think we fulfilled. I struggled with that because I [said], “We will take care of you. I know your family’s not here. I got you. We’ll make sure you’re okay.” And then they’re not okay. I carry a lot of guilt with that.
Nurses especially found themselves in the vulnerable position of communicating new government and hospital policies that were intended to protect patients, visitors, and staff from the spread of infection, but that also created strains for ill patients and their families. Some described the pain of being caught in the conflict between human values like care, contact, and family support and the public health priorities of minimizing infectious contacts and decreasing the burden of illness on hospitals.
We couldn’t have any visitors at bedside. In triage, their family would rush their loved one in. It would always be the nurse [who had] to say, “Unfortunately, you have to leave, due to federal regulations coming from the state.” The horrific and ugly things that we were called on a daily basis. . . . We were fileted. But, at the same time, you’re separating their family from that person, and you know that’s probably the last time they’re going to see them. . . . I had one woman say I’m a heartless, egotistical sadistic person: “When he dies, it’s not going to be from COVID. The cause of death is you because you separated us.”
They threatened litigation, and I understand the fear; people were lashing out because they were truly afraid. But when you hear those things again and again and again, you start thinking, “Is this the right thing that I’m doing? Is there any good that’s coming from it? Am I just following what is ordered down?”
Perceptions as Heroes and Villains. Health care providers found themselves simultaneously celebrated as health care heroes, while also targeted by the public’s anger around being controlled by masking mandates, lockdowns, and separation from their loved ones in the hospital. This experience evoked a range of emotions, including confusion, resentment, and a sense of not deserving the distorted positive or negative public perceptions. Being praised or blamed for circumstances beyond their control, given the psychological and physical demands they were already experiencing on the job, added further internal strain for our participants.
[We]’d go out at 7:00 at night and everyone would be cheering, and [we all] felt like a fraud, because all [we] did was pronounce people [dead] all day.
The hero narrative, or perhaps more accurately hero fallacy, served as a particularly powerful defense against shame and guilt used on a society-wide level. Identifying health care workers in general, or one’s more exposed colleagues specifically, as more heroic became a near universal way to manage the difficult feelings of recognizing when more was being asked of others than individuals were willing to do themselves. Though higher burdens of risk were more typically a result of one’s role or placements (nurses versus doctors, hospital location) rather than one’s choices, the narrative often returned to those more at risk as being “braver” or more honorable and often more underrecognized or underappreciated. The hero fallacy increased guilt for receiving recognition while being aware that others—the “real” heroes—were more at risk. For others, it sparked resentment that this feel-good narrative diminished their experiences of fear and danger.
I remember being very viscerally angry at this idea of being a health care hero. Because I was like when did we decide that I will die at my job? I don’t want to be a hero. Being a hero means that everybody before me has failed at their job.
In addition to their experiences on the job, some health care workers felt further endangered and distressed by public narratives around pandemic policies. There was a sense of disenchantment in the public’s failure to uphold their end of an unspoken deal. Anger at the experience of imperfect leadership at all levels of government and the hospital felt further embittering. Participants directed blame toward both the public and their leaders for their experience of inability to meet standards of care.
I’m broken and angry, really angry. I’m trying to find a way to use that anger, but the misinformation and attacking people for trying to keep you safe, I don’t understand that. Just wear the mask!
I know there are [colleagues] who get mad at people for not wearing masks or for not taking precautions or whatever. I think I just stopped caring. . .I would notice it, but I wouldn’t be the one to tell you to do anything. If I don’t know you, I’m not going to be able to change anything about you in our interactions, and I’m still going to be here if you get sick.
DISCUSSION
The ethnographic design chosen to examine moral injury enabled us to obtain a richer account of the participants’ experiences than could be gained from qualitative surveys about their perceived omissions and commissions. This stands in contrast to much of the recent research on moral injury in COVID-19 responders.
The major limitations of this study are due to small sample size. This affects the statistical power necessary to detect significant differences in the results of the survey data, while also affecting the extent to which our findings might be generalizable. Self-selection bias might have further compounded this issue, as participants may have held characteristics, motivations, or experiences distinct from those who chose not to enroll in the study. Future directions in studying moral injury might examine the role of dependency on leadership structures and relationships with self and others that create the conditions for moral injury.
CONCLUSION
The pandemic upended the previously reliable and imperceptible experience of a background of safety,13 in which the provision of both protective equipment and human presence at minimum were unquestioned. It shed light on the vulnerability of the relationships that undergird our current health care system—between doctors and patients, clinicians and administrators, and among colleagues. Our analysis of interview data highlights how omissions and commissions in one’s professional duties created internal conflicts, which were inextricably linked to deeper feelings of guilt and blame around experiences of betraying or being betrayed and a resultant inability to uphold one’s moral values. Both of these elements of moral injury provide a helpful lens to begin to more deeply understand the experiences of health care workers during the COVID-19 pandemic.
Article Information
Published Online: February 27, 2024.
https://doi.org/10.4088/PCC.23m03651
© 2024 Physicians Postgraduate Press, Inc.
Submitted: August 23, 2023; accepted October 19, 2023.
To Cite: Appel G, Han BH, Re’Em Y, et al. Omission and commission in morally injurious experiences among COVID-19 health care professionals. Prim Care Companion CNS Disord. 2024;26(1):23m03651.
Author Affiliations: Department of Psychiatry, Weill Cornell Medicine, New York, New York (Appel, Han, Re’Em, Louka, Tom, Difede, Avery); Department of Emergency Medicine, Weill Cornell Medicine, New York, New York (Sundararajan, Zaidi); Department of Population Health Sciences, Weill Cornell Medicine, New York, New York (An).
Corresponding Author: Giselle Appel, BA, Department of Psychiatry, Weill Cornell Medical College, 525 East 68th St, New York, NY 10065 ([email protected]).
Funding/Support: None.
Relevant Financial Relationships: None.
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- The concept of moral injury involves the distress arising when an individual’s sense of moral rightness is betrayed by leadership structures, leading to a transgression of deeply held moral beliefs.
- Despite the emotional distress associated with them, moral challenges and associated emotions also have the purpose of grounding and clarifying a sense of identity for health care workers.
- Actions inconsistent with one’s moral values resulted in a range of emotions, including helplessness, guilt, and shame among health care workers; recognizing and understanding these emotions is crucial for addressing the psychological impact of moral challenges in health care settings.
References (13)

- Murphy SL, Kochanek KD, Xu J, et al. Mortality in the United States, 2020. NCHS Data Brief. 2021;(427):1–8. PubMed
- Talbot S, Dean W. Physicians aren’t “burning out.” They’re suffering from moral injury [Internet]. STAT. 2018. Accessed August 19, 2023. https://www.statnews.com/2018/07/26/physicians-not-burning-out-they-are-suffering-moral-injury/
- The Moral Crisis of America’s Doctors. The New York Times [Internet]. Accessed June 15, 2023. https://www.nytimes.com/2023/06/15/magazine/doctors-moral-crises.html
- Shay J. Moral injury. Intertexts. 2012;16(1):57–66. CrossRef
- Shay J. Learning about combat stress from Homer’s Iliad. J Trauma Stress. 1991;4(4):561–579. CrossRef
- Litz BT, Stein N, Delaney E, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev. 2009;29(8):695–706. PubMed CrossRef
- Molendijk T, Kramer EH, Verweij D. Moral aspects of “moral injury”: analyzing conceptualizations on the role of morality in military trauma. J Mil Ethics. 2018;17(1):36–53. CrossRef
- Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract. 2019;36(9):400–402. PubMed
- Mantri S, Lawson JM, Wang Z, et al. Identifying moral injury in healthcare professionals: the moral injury symptom scale-HP. J Relig Health. 2020;59(5):2323–2340. PubMed CrossRef
- Guest G, Bunce A, Johnson L. How many interviews are enough? An experiment with data saturation and variability. Field Methods. 2006;18(1):59–82. CrossRef
- Feldman G, Kutscher L, Yay T. Omission and commission in judgment and decision making: understanding and linking action-inaction effects using the concept of normality. Soc Personal Psychol Compass. 2020;14(8):e12557. CrossRef
- Williamson V, Lamb D, Hotopf M, et al. Moral injury and psychological wellbeing in UK healthcare staff. J Ment Health. 2023;32(5):890–898. PubMed CrossRef
- Sandler J. The background of safety. Int J Psychoanal. 1960;41:352–356. PubMed
Please sign in or purchase this PDF for $40.