Objective: Trust, a fundamental part of human interpersonal relationships, is known to be associated with specific brain regions and demographic characteristics. Level of trust in medical professionals can alter population health outcomes and influence the nature of the doctor-patient relationship. This study utilized structural magnetic resonance imaging (MRI) and trust data from the Dallas Heart Study (DHS), a large community-based study, to determine brain regions associated with degree of trust in physicians and the medical profession. The first phase of the DHS was conducted from 2000 to 2002 and the second phase from 2007 to 2009.
Methods: The MRI data were analyzed as part of the DHS using automated FreeSurfer software. Forward stepwise binary logistic regression was performed to investigate the association between measures of trust and bilateral brain region volumes and thickness followed by confirmatory multiple regressions of significant brain regions. A total of 1,596 participants were included in the final analysis.
Results: Left caudal anterior cingulate cortex (ACC) thickness was inversely correlated with trust of physicians (P < .01). There were no significant associations between trust in physicians and age, race or ethnicity, or education.
Conclusions: The ACC is an integral part of the salience network, the brain network responsible for communication and social behavior. Trust in physicians did not appear to be influenced by demographic characteristics. The findings suggest there are neuroanatomical correlates of trust in physicians.
ABSTRACT
Objective: Trust, a fundamental part of human interpersonal relationships, is known to be associated with specific brain regions and demographic characteristics. Level of trust in medical professionals can alter population health outcomes and influence the nature of the doctor-patient relationship. This study utilized structural magnetic resonance imaging (MRI) and trust data from the Dallas Heart Study (DHS), a large community-based study, to determine brain regions associated with degree of trust in physicians and the medical profession. The first phase of the DHS was conducted from 2000 to 2002 and the second phase from 2007 to 2009.
Methods: The MRI data were analyzed as part of the DHS using automated FreeSurfer software. Forward stepwise binary logistic regression was performed to investigate the association between measures of trust and bilateral brain region volumes and thickness followed by confirmatory multiple regressions of significant brain regions. A total of 1,596 participants were included in the final analysis.
Results: Left caudal anterior cingulate cortex (ACC) thickness was inversely correlated with trust of physicians (P < .01). There were no significant associations between trust in physicians and age, race or ethnicity, or education.
Conclusions: The ACC is an integral part of the salience network, the brain network responsible for communication and social behavior. Trust in physicians did not appear to be influenced by demographic characteristics. The findings suggest there are neuroanatomical correlates of trust in physicians.
Prim Care Companion CNS Disord 2019;21(5):19m02461
To cite: Sadhu M, Jalalizadeh B, Fritz A, et al. Trust in physicians and regional brain volumes: a population-based study. Prim Care Companion CNS Disord. 2019;21(5):19m02461.
To share: https://doi.org/10.4088/PCC.19m02461
© Copyright 2019 Physicians Postgraduate Press, Inc.
aDepartment of Psychiatry, The University of Texas Southwestern Medical Center, Dallas, Texas
*Corresponding author: E. Sherwood Brown, MD, PhD, Department of Psychiatry, The University of Texas Southwestern Medical Center, 5323 Harry Hines Blvd, MC 8849, Dallas, TX 75390-8849 ([email protected]).
Trust is an integral part of any human relationship1 and as such extends to the relationship between patients and health care providers. Although a singular definition has been difficult to pinpoint, trust can be characterized as a process involving the combination of feelings, emotions, and thinking in relation to balancing risk versus reward based on expectations of another person’s behavior.2 Trust is influenced by situational and contextual factors, as well as knowledge of behavior or reputation.2 The imbalance of knowledge and power inherent in the relationship between patients and their health care provider means that patients must often rely on trust when seeking care,3 and this is recognized and respected by the ethical codes of professional organizations.4–6
The role of trust has been examined in numerous studies7–19 of the patient-physician relationship. Distrust can be a barrier to the use of available medical services and thus to optimal health.7–9 In patients with chronic conditions such as hemophilia,10 HIV,11 insulin-dependent diabetes,12 and sickle cell disease,13 those with less trust in physicians had lower adherence. Poor social trust has been linked to increased death rates from coronary heart disease, cancer, and infant mortality.14 On the other hand, greater trust in physicians is associated with medication adherence.15 Furthermore, trust in physicians may be a factor in the placebo response,16 perhaps acting through oxytocin.17–19 Thus, trust in physicians is an important aspect of patient care and clinical outcomes.
In recognition of the importance of trust in the patient-physician relationship, multiple independent measures of patient-physician trust have been developed.20–23 Although the influence of experiential and historical factors affecting the development of patient trust of medical providers has been examined, little is known about the neurobiology involved. The neurobiological underpinnings of trust in general, however, have been examined using laboratory paradigms and imaging modalities. One study24 found that the prefrontal cortex, anterior insula, and amygdala played a role in the social-cognitive processing responsible for trust development. Another study25 showed that individuals with larger gray matter volume in the prefrontal cortex and anterior insula trust more easily. Additionally, multiple studies26,27 have identified the amygdala as crucial to the development of interpersonal trust. A functional magnetic resonance imaging (fMRI) study also implicated the dorsal striatum (caudate nucleus and putamen), anterior paracingulate cortex, and orbitofrontal cortex in the neural correlates of trust.28 Studies using both fMRI and electroencephalography (EEG) have identified the striatum and anterior cingulate cortex (ACC) as regions of interest in the formation of interpersonal trust.2 Within the ACC, the caudal/dorsal ACC and the rostral/ventral ACC may serve separate roles in emotional processing.29 This regional separation of function is supported by the caudal/dorsal ACC having extensive connections to cortical areas related to cognition and movement, while the rostral/ventral ACC has extensions to read brain areas important for emotion, memory, and reward functions.29 The external connections of the ACC as a whole suggest that the ACC may be implicated in developing trust, given the crucial role of evaluation and appraisal of emotion in that process.30,31 While not explicitly identified in interpersonal trust, increased activity in the right midfrontal gyrus has been associated with intention to conceal information,32 and greater interconnectivity of the right midfrontal gyrus and other regions predicts placebo response.33
The aim of this study was to identify brain regions associated with trust of a physician by a patient. The sample utilized data from the Dallas Heart Study (DHS), a large and multiethnic epidemiologic sample of Dallas County residents.
METHODS
Study Sample
The DHS is a large, multiracial, multiethnic, and socially diverse community-based study that included an epidemiologic sample of adults living in Dallas County, Texas. The first phase of the DHS (DHS-1), conducted from 2000 to 2002, was designed to examine cardiovascular disease risk factors and collect data for future research.34 The study intentionally oversampled African Americans to have power to examine cardiovascular disease risk factors in this subpopulation. The data obtained from DHS-1 included a question in which participants reported their level of trust in doctors and the medical profession in general.
The second phase of the Dallas Heart Study (DHS-2) was conducted from 2007 to 2009. In DHS-2, participants from the initial DHS-1 were asked to participate in a follow-up study approximately 7 years later. DHS-2 participants were either participants of DHS-1 or family members (or spouses) of DHS-1 participants so as to replace participants lost to attrition. As part of DHS-2, some participants underwent brain magnetic resonance imaging (MRI) at The University of Texas Southwestern Medical Center. The study sample included only volunteers who participated in both DHS-1 and DHS-2.
Demographic characteristics included in this study consisted of self-reported race/ethnicity (African-American, white, Hispanic, or other), level of education (quit high school, high school graduate, or post high school), age, and sex.
Exclusion criteria were lack of demographic data from DHS-1 such as age, sex, or education level; missing answer on the physician trust question in DHS-1; and missing MRIs from DHS-2. The Institutional Review Board at The University of Texas Southwestern Medical Center approved the study, and all participants provided written informed consent.
Measure of Trust
As part of a questionnaire administered to all participants in DHS-1, one particular item asked participants to “Think about doctors and the medical profession in general. Please rate the level of trust you feel toward them.” The possible answer choices were “Trust them completely,” “Trust them partially,” and “Not trust them at all.” Participants who responded to this physician trust question were included in the analysis. Responses to this particular question have been investigated previously in other contexts.35
MRI Protocol and Imaging Analysis
Brain MRIs were collected with a 3-T MRI system (3T Achieva, Philips Healthcare, Cleveland, Ohio) at The University of Texas Southwestern Medical Center using protocols and techniques previously discussed in detail.36 Quantification and separation of distinct brain MR regions were performed as part of the DHS study using FreeSurfer image analysis software, version 4.4 (Martinos Center for Biomedical Imaging, Boston, Massachusetts). The specific parameters of the FreeSurfer tool kit used for automated segmentation of brain regions have been described in detail previously.37 DHS recorded neuroimaging data by using gray-white matter segmentation, cortical surface models, and statistical analysis of morphometry differences. Images were reviewed during quality control by a trained observer and reviewed for exclusion by 2 neuroradiologists. Abnormalities flagged during image exclusion included lesions occupying a large space, cortical strokes, brain tissue loss, metal artifacts, and image processing errors.36 The current analysis used existing regional brain volume data from this large dataset.
Statistical Analysis
From the DHS-1 and DHS-2 data, several variables were defined for clear and standardized analysis. Due to the overrepresentation of African-Americans, the race variable in the present study was dichotomized into African-Americans and “other race.” Regarding the trust question, a new physician trust variable was established by dichotomizing the original answer choices. Responses of “trust them completely” were recorded as “complete trust,” and “trust them partially” and “not trust them at all” responses were collapsed into a single “partial or no trust” value. This dichotomization was performed because only 2.3% of responders answered “not trust them at all.”
A comparison of the included and excluded sample of participants was conducted. In this comparison, χ2 analyses were performed to assess for statistically significant differences in categorical variables, and independent sample t tests were performed to assess differences in the continuous variables. Statistical significance was defined by a P value < .05.
A forward stepwise binary logistic regression analysis was performed using SPSS version 25 software (IBM Corporation; Armonk, New York; 2017) to investigate the association between self-reported trust in physician and bilateral brain region volume and thickness in specific regions of interest (ROIs). Regions investigated were caudal and rostral anterior cingulate cortex volume and cortical thickness, posterior cingulate cortex volume, frontal pole volume, medial orbitofrontal volume, lateral orbitofrontal volume, rostral middle frontal volume, superior frontal volume and cortical thickness, inferior temporal volume, cuneus volume, amygdala volume, insula volume, thalamus volume, caudate volume, putamen volume, and accumbens volume. These brain regions had been implicated in prior research studies2,24–31 on trust. The objective was to determine which brain regions are related to trust of physicians and the medical profession. A single stepwise regression was used, in contrast to separate regressions, to explore numerous brain regions without requiring correction for multiple comparisons. This regression was followed by a confirmatory binary logistic regression of brain regions identified using the stepwise approach and including the same demographic covariates as well as intracranial volume. Finally, to explore the influence of the group with no trust on the findings and provide support for the decision to collapse the original trust choices “trust them partially” and “not trust them at all” into a single “partial or no trust” value, an additional binary logistic regression was conducted to assess how the emergent regions predict membership in 1 of the 2 no/low trust groups.
For all analyses, age, sex, race, education, and intracranial volume were used as independent covariates. Interaction terms between the specific ROI and covariates of age, sex, race, and education were conducted to evaluate a potential interaction effect between brain ROI and covariates. Statistical significance was defined by a P value < .05.
RESULTS
Of the initial cohort of 2,485 individuals who participated in both DHS-1 and DHS-2, 889 participants were excluded from the present analysis, with the remaining 1,596 participants included in the final analysis of the physician trust metric. Of those excluded, a majority (n = 854) were excluded due to lack of MRIs in DHS-2, and the remainder were excluded due to missing demographic information (n = 27) or missing data from the physician trust question (n = 8) in DHS-1. The final sample is described in Figure 1
 .
.
Participants excluded due to missing data had statistically significant differences in race, education, and age compared to the sample included in the analysis. There were no significant differences in sex, mean intracranial volume, or response to the physician trust question. The demographics of included and excluded participants are shown in Table 1. To evaluate for moderating effects between the specific ROI, covariates, and the possible need for subgroup analyses, interaction terms were created. Interaction terms of all the ROIs by age, sex, race, and education were conducted, and no significant interactions were found.
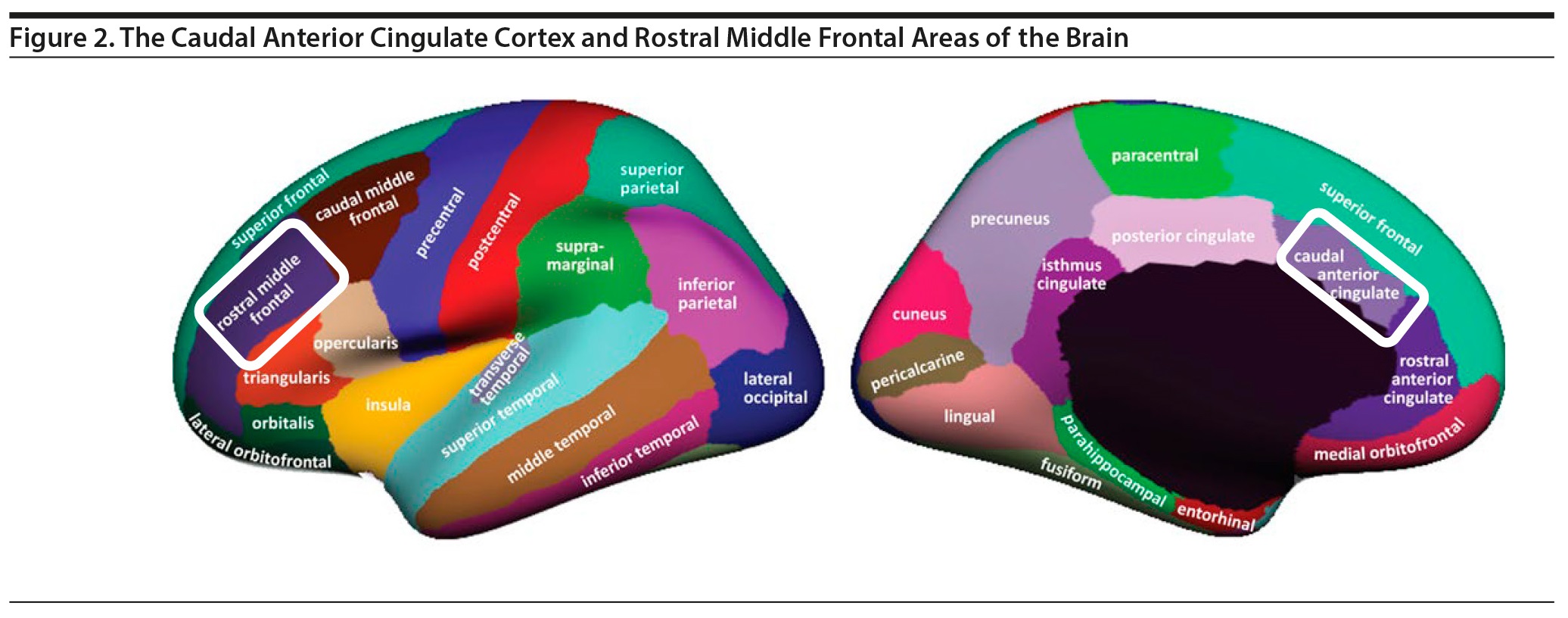
The primary finding of stepwise analysis was that left caudal ACC thickness and right rostral middle frontal volume were inversely associated with physician trust (P = .004 and P = .034, respectively). These results are described in Table 2. Figure 2 demonstrates the caudal ACC and rostral middle frontal areas of the brain as defined by FreeSurfer. In the stepwise regression, no other ROIs studied showed significance regarding the physician trust metric. Age, sex, race, and education were not significantly associated with physician trust. Confirmatory analyses using binary logistic regressions of left caudal ACC thickness, right rostral middle frontal volume, and demographic covariates revealed that left caudal ACC thickness was significantly associated with the trust question response (B = −0.453, P = .005, odds ratio [OR] = 0.636, 95% CI, 0.463–0.873) with a trend for right rostral middle frontal volume (B = −0.059, P = .057, 95% CI, 0.887–1.002). A binary logistic regression was used to compare the “not trust them at all” and “trust them partially” groups. The relationship of the 2 groups to left caudal ACC thickness (B = −0.006, P = .979, OR = 0.994) and right rostral middle frontal volume (B = −0.033, P = .455, OR = 0.967) was not significantly different.
DISCUSSION
In this study, we demonstrated an association between brain ROI volume/thickness and reported trust in physicians. ACC thickness is also positively related to alexithymia38 and posttraumatic stress disorder improvement.39 It is inversely related to aggression,40 obsessive-compulsive disorder severity,41 and attention-deficit/hyperactivity disorder42 and is inconsistently related to depression.43,44 The ACC, as a component of the salience network, is known to have extensive connections to multiple brain regions and has been implicated in processes relating to motor activity, cognition, emotion, reward, and memory.45,46 In particular, the dorsal-caudal region of the ACC is implicated in expression of fear and anxiety.30
The stepwise regression suggested that right rostral middle frontal volume was also associated with physician trust. However, a binary logistic regression including only this brain region and covariates showed a trend (P = .057) for an association between this brain region and trust. While middle frontal gyrus volume differences have not been previously implicated in trust, such differences are associated with age-related decline in episodic memory retrieval47 and first-episode depression.48 In healthy young adults, the process of context retrieval as a part of episodic memory has been associated with increased activity in the middle frontal gyrus.47 As middle frontal gyrus volume has been demonstrated to effect episodic memory retrieval (and thus context retrieval), along with affect and present cognition, volume differences may affect the development of trust in physicians.2
The current study found no association of age, sex, race, or education with self-reported trust in physicians. This finding is consistent with other research49 that demonstrates when trust in physicians is assessed directly (for example by asking “Do you trust your doctor?”) as in this study, or when multiple questions assessing trust are aggregated into 1 score, there tend to be no significant differences between US racial and ethnic groups. However, prior research49,50 demonstrates that when trust is assessed indirectly (when participants are asked about expected behaviors of others in a particular situation), racial and ethnic differences in trust are observed. For example, 1 study51 of patients with advanced liver disease found no significant difference in trust in health care providers when responses to multiple questions were aggregated into 1 score, but black participants were more likely to believe their doctor would let them die if they were an organ donor so that their organs could be given to others. By relying on 1 direct question to assess trust in physicians, we may not have uncovered the full extent of physician mistrust among our sample.
This study has some limitations. The greater exclusion of African-Americans and people with lower education levels due to missing data raises the concern for possible selection bias. While this possibility cannot be ruled out, interaction terms of ROI and race or education were not significant. This finding suggests that neither race nor education significantly influenced the relationship between the ROIs and trust. Because our sample comprised participants in a large, longitudinal, and invasive medical research study, individuals with the least trust in physicians, medical professionals, and medical research may have excluded themselves from participation. Individuals who underwent MRI but were excluded for not answering the physician trust question (n = 8) may be particularly untrusting in physicians. Nonetheless, 64.1% endorsed partial or no trust, suggesting that people with less than full trust in the medical profession participated in the study. The trust question was administered in DHS-1, while brain volumes were assessed in DHS-2, which could influence the findings since physician trust could vary over time. A dichotomized, rather than continuous, trust variable was used, which may have limited the ability of the analysis to detect subtle differences in trust.
The use of an automated method of imaging analysis, FreeSurfer, is a strength of the study and was needed to analyze such a large number of images. However, brain regions are defined somewhat differently by FreeSurfer than with a ROI subdividing system.37 While these differences in regions may have led to some differences in results, it has been shown that automated subdividing programs consistently demonstrate highly reliable results, lower variability, greater validity, and improved reproducibility compared to manual systems.37 This study used preexisting data from the large DHS study database, which is both a strength and a limitation. While the database provided neuroimaging and trust data on a large, diverse, community-based sample, the study was limited by the data included in the DHS.
CONCLUSION
This study uncovered new insight into brain regions associated with trust in physicians. The findings demonstrate an association between self-reported physician trust and brain regions previously known to be involved with affect processing and recollection of past experience. This finding is consistent with previous studies2,30,45,47 showing that both types of input contribute to the development of mistrust or trust. The findings suggest that trust in physicians may not be influenced greatly by demographic characteristics. However, more nuanced methods of assessing trust than the survey used here may have been able to identify more subtle distinctions. Nonetheless, even with 1-item self-report, there appear to be neuroanatomical correlates of trust in physicians. This understanding may be enhanced by further investigation of the left caudal ACC or right rostral middle frontal gyrus using neuroimaging techniques such as fMRI during a trust task and by employing more nuanced questionnaires that use multiple direct and indirect approaches to assess trust in physicians. We observed a relationship between caudal ACC thickness and physician trust. The ACC is a brain region implicated in the placebo response.52–54 However, to our knowledge, prior studies have not examined thickness. A better understanding of the neurobiology of trust in physicians may allow for the development of techniques that might serve to enhance this trust and improve the quality of the doctor-patient relationship, as well provide clues to the neurobiology of clinical outcomes including the placebo response.
Submitted: March 19, 2019; accepted August 8, 2019.
Published online: October 17, 2019.
Potential conflicts of interest: Dr Brown reports grants from the National Institutes of Health, the Stanley Medical Research Institute, and Otsuka and serves on an advisory board for Allergan. Drs Sadhu, Jalalizadeh, Fritz, de Freitas Nicholson, Garcia, Lampley, Rain, and Van Enkevort report no conflicts of interest related to the subject of this article.
Funding/support: Research reported in this publication was supported by the National Center for Advancing Translational Sciences of the National Institutes of Health (award no. UL1TR001105).
Role of the sponsor: The funder had no role in study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclaimer: The content is solely the responsibility of the authors and does not necessarily represent the official views of the National Institutes of Health.
Acknowledgments: The authors thank Jayme Palka, BS, Department of Psychiatry, The University of Texas Southwestern Medical Center, Dallas, Texas, for providing statistical advice on the revised manuscript. Ms Palka reports no conflicts of interest related to the subject of this article.
Open practices statement: None of the data or materials for the experiments reported here are available, and none of the experiments were preregistered.
REFERENCES
1. Krueger F, McCabe K, Moll J, et al. Neural correlates of trust. Proc Natl Acad Sci U S A. 2007;104(50):20084–20089. PubMed CrossRef
2. Borum R. The Science of Interpersonal Trust. Mental Health Law & Policy Faculty Publications; 2010. https://scholarcommons.usf.edu/mhlp_facpub/574. Accessed September 17, 2019.
3. Goold SD. Trust, distrust and trustworthiness. J Gen Intern Med. 2002;17(1):79–81. PubMed CrossRef
4. Ethical Principals of Psychologists and Code of Conduct. Adopted August 21, 2002, Effective June 1, 2003: With the 2010 Amendments Adopted February 20, 2010, Effective June 1, 2010. American Psychological Association website. https://www.apa.org/ethics/code/principles.pdf. 2010. Accessed September 17, 2019.
5. Protection of the Rights and Privacy and Confidentiality. Provision 3.1. In: Code of Ethics for Nurses with Interpretive Statements. Silver Spring, MD: American Nurses Association; 2015.
6. Opinions on Patient-Physician Relationships. Opinion 1.1.1. In: Code of Medical Ethics. Chicago, IL: American Medical Association; 2016.
7. Whetten K, Leserman J, Whetten R, et al. Exploring lack of trust in care providers and the government as a barrier to health service use. Am J Public Health. 2006;96(4):716–721. PubMed CrossRef
8. Bell RA, Arcury TA, Ip E, et al. Correlates of physician trust among rural older adults with diabetes. Am J Health Behav. 2013;37(5):660–666. PubMed CrossRef
9. Musa D, Schulz R, Harris R, et al. Trust in the health care system and the use of preventive health services by older black and white adults. Am J Public Health. 2009;99(7):1293–1299. PubMed CrossRef
10. Tran DQ, Barry V, Antun A, et al. Physician trust and depression influence adherence to factor replacement: a single-centre cross-sectional study. Haemophilia. 2017;23(1):98–104. PubMed CrossRef
11. Dale SK, Bogart LM, Wagner GJ, et al. Medical mistrust is related to lower longitudinal medication adherence among African-American males with HIV. J Health Psychol. 2016;21(7):1311–1321. PubMed CrossRef
12. Halepian L, Saleh MB, Hallit S, et al. Adherence to insulin, emotional distress, and trust in physician among patients with diabetes: a cross-sectional study. Diabetes Ther. 2018;9(2):713–726. PubMed CrossRef
13. Haywood C Jr, Lanzkron S, Bediako S, et al; IMPORT Investigators. Perceived discrimination, patient trust, and adherence to medical recommendations among persons with sickle cell disease. J Gen Intern Med. 2014;29(12):1657–1662. PubMed CrossRef
14. Kawachi I, Kennedy BP, Lochner K, et al. Social capital, income inequality, and mortality. Am J Public Health. 1997;87(9):1491–1498. PubMed CrossRef
15. Reach G, Pellan M, Crine A, et al. Holistic psychosocial determinants of adherence to medication in people with type 2 diabetes. Diabetes Metab. 2018;44(6):500–507. PubMed CrossRef
16. Hunter P. A question of faith: exploiting the placebo effect depends on both the susceptibility of the patient to suggestion and the ability of the doctor to instill trust. EMBO Rep. 2007;8(2):125–128. PubMed CrossRef
17. Kessner S, Sprenger C, Wrobel N, et al. Effect of oxytocin on placebo analgesia: a randomized study. JAMA. 2013;310(16):1733–1735. PubMed CrossRef
18. Jneid S, Jabbour H, Hajj A, et al. Quality of life and its association with treatment satisfaction, adherence to medication, and trust in physician among patients with hypertension: a cross-sectional designed study. J Cardiovasc Pharmacol Ther. 2018;23(6):532–542. PubMed CrossRef
19. Cuthbertson L, Kowalewski K, Edge J, et al. Factors that promote and hinder medication adherence from the perspective of inmates in a provincial remand center: a mixed methods study. J Correct Health Care. 2018;24(1):21–34. PubMed CrossRef
20. Freburger JK, Callahan LF, Currey SS, et al. Use of the Trust in Physician Scale in patients with rheumatic disease: psychometric properties and correlates of trust in the rheumatologist. Arthritis Rheum. 2003;49(1):51–58. PubMed CrossRef
21. Dugan E, Trachtenberg F, Hall MA. Development of abbreviated measures to assess patient trust in a physician, a health insurer, and the medical profession. BMC Health Serv Res. 2005;5(1):64. PubMed CrossRef
22. Thom DH, Wong ST, Guzman D, et al. Physician trust in the patient: development and validation of a new measure. Ann Fam Med. 2011;9(2):148–154. PubMed CrossRef
23. Müller E, Zill JM, Dirmaier J, et al. Assessment of trust in physician: a systematic review of measures. PLoS One. 2014;9(9):e106844. PubMed CrossRef
24. Haas BW, Ishak A, Anderson IW, et al. The tendency to trust is reflected in human brain structure. Neuroimage. 2015;107:175–181. PubMed CrossRef
25. Adolphs R. Trust in the brain. Nat Neurosci. 2002;5(3):192–193. PubMed CrossRef
26. Adolphs R, Tranel D, Damasio AR. The human amygdala in social judgment. Nature. 1998;393(6684):470–474. PubMed CrossRef
27. Koscik TR, Tranel D. The human amygdala is necessary for developing and expressing normal interpersonal trust. Neuropsychologia. 2011;49(4):602–611. PubMed CrossRef
28. Dimoka A. Brain mapping of psychological processes with psychometric scales: an fMRI method for social neuroscience. Neuroimage. 2011;54(suppl 1):S263–S271. PubMed CrossRef
29. Stevens FL, Hurley RA, Taber KH. Anterior cingulate cortex: unique role in cognition and emotion. J Neuropsychiatry Clin Neurosci. 2011;23(2):121–125. PubMed CrossRef
30. Etkin A, Egner T, Kalisch R. Emotional processing in anterior cingulate and medial prefrontal cortex. Trends Cogn Sci. 2011;15(2):85–93. PubMed CrossRef
31. Heatherton TF. Neuroscience of self and self-regulation. Annu Rev Psychol. 2011;62(1):363–390. PubMed CrossRef
32. Matsuda I, Nittono H. The intention to conceal activates the right prefrontal cortex: an event-related potential study. Neuroreport. 2015;26(4):223–227. PubMed CrossRef
33. Tétreault P, Mansour A, Vachon-Presseau E, et al. Brain connectivity predicts placebo response across chronic pain clinical trials. PLoS Biol. 2016;14(10):e1002570. PubMed CrossRef
34. Victor RG, Haley RW, Willett DL, et al; Dallas Heart Study Investigators. The Dallas Heart Study: a population-based probability sample for the multidisciplinary study of ethnic differences in cardiovascular health. Am J Cardiol. 2004;93(12):1473–1480. PubMed CrossRef
35. Vaeth PA, Willett DL. Illness risk perceptions and trust: the association with blood pressure self-measurement. Am J Health Behav. 2011;35(1):105–117. PubMed CrossRef
36. Gupta M, King KS, Srinivasa R, et al. Association of 3.0-T brain magnetic resonance imaging biomarkers with cognitive function in the Dallas Heart Study. JAMA Neurol. 2015;72(2):170–175. PubMed CrossRef
37. Desikan RS, Ségonne F, Fischl B, et al. An automated labeling system for subdividing the human cerebral cortex on MRI scans into gyral based regions of interest. Neuroimage. 2006;31(3):968–980. PubMed CrossRef
38. Demers LA, Olson EA, Crowley DJ, et al. Dorsal anterior cingulate thickness is related to alexithymia in childhood trauma-related PTSD. PLoS One. 2015;10(10):e0139807. PubMed CrossRef
39. Dickie EW, Brunet A, Akerib V, et al. Anterior cingulate cortical thickness is a stable predictor of recovery from post-traumatic stress disorder. Psychol Med. 2013;43(3):645–653. PubMed CrossRef
40. Ducharme S, Hudziak JJ, Botteron KN, et al; Brain Development Cooperative Group. Right anterior cingulate cortical thickness and bilateral striatal volume correlate with child behavior checklist aggressive behavior scores in healthy children. Biol Psychiatry. 2011;70(3):283–290. PubMed CrossRef
41. Kühn S, Kaufmann C, Simon D, et al. Reduced thickness of anterior cingulate cortex in obsessive-compulsive disorder. Cortex. 2013;49(8):2178–2185. PubMed CrossRef
42. Bledsoe JC, Semrud-Clikeman M, Pliszka SR. Anterior cingulate cortex and symptom severity in attention-deficit/hyperactivity disorder. J Abnorm Psychol. 2013;122(2):558–565. PubMed CrossRef
43. Schmaal L, Hibar DP, Sämann PG, et al. Cortical abnormalities in adults and adolescents with major depression based on brain scans from 20 cohorts worldwide in the ENIGMA Major Depressive Disorder Working Group. Mol Psychiatry. 2017;22(6):900–909. PubMed CrossRef
44. Reynolds S, Carrey N, Jaworska N, et al. Cortical thickness in youth with major depressive disorder. BMC Psychiatry. 2014;14(1):83. PubMed CrossRef
45. Margulies DS, Kelly AM, Uddin LQ, et al. Mapping the functional connectivity of anterior cingulate cortex. Neuroimage. 2007;37(2):579–588. PubMed CrossRef
46. Vogt B. Cingulate Neurobiology and Disease. London, UK: Oxford University Press; 2009.
47. Rajah MN, Languay R, Grady CL. Age-related changes in right middle frontal gyrus volume correlate with altered episodic retrieval activity. J Neurosci. 2011;31(49):17941–17954. PubMed CrossRef
48. Han KM, Choi S, Jung J, et al. Cortical thickness, cortical and subcortical volume, and white matter integrity in patients with their first episode of major depression. J Affect Disord. 2014;155:42–48. PubMed CrossRef
49. Stepanikova I, Mollborn S, Cook KS, et al. Patients’ race, ethnicity, language, and trust in a physician. J Health Soc Behav. 2006;47(4):390–405. PubMed CrossRef
50. Sewell AA. Disaggregating ethnoracial disparities in physician trust. Soc Sci Res. 2015;54:1–20. PubMed CrossRef
51. Jones P, Kanwal F. Communication and trust: critically important to eliminate disparities in liver transplantation. Liver Transpl. 2016;22(7):881–883. PubMed CrossRef
52. Benedetti F. Placebo and the new physiology of the doctor-patient relationship. Physiol Rev. 2013;93(3):1207–1246. PubMed CrossRef
53. Eippert F, Bingel U, Schoell ED, et al. Activation of the opioidergic descending pain control system underlies placebo analgesia. Neuron. 2009;63(4):533–543. PubMed CrossRef
54. Mayberg HS, Silva JA, Brannan SK, et al. The functional neuroanatomy of the placebo effect. Am J Psychiatry. 2002;159(5):728–737. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





