Abstract
Sleep is an important biological function. This article considers practical matters related to the prescription of sedative-hypnotic drugs to patients with insomnia. This article also presents practical suggestions for the management of excessive sedation in patients who need pharmacologic treatments with sedating adverse effects when dose reduction is not an option. Issues examined include the choice of drug for sleep-onset insomnia and for sleep-maintenance insomnia; the choice of drug for insomnia in patients with psychiatric disorders; sedative-hypnotic dosing in contexts such as perturbation of multiple neurotransmitter systems; metabolic drug interactions with sedative-hypnotic drugs; gastrointestinal absorption of hypnotic drugs and time to onset of drowsiness; the effect of food on absorption and time to onset of drowsiness; the effect of glucagon-like peptide-1 receptor agonist (GLP-1RA) drugs on absorption and time to onset of drowsiness; the importance of half-life for the duration of action of the sedative-hypnotic drug; strategies to address oversedation with sedating psychotropic drugs; treating insomnia with classical monoamine oxidase inhibitors, especially tranylcypromine; optimization of sedative-hypnotic therapy; provision of patient guidance; and related matters. Readers are also reminded that sleep hygiene and cognitive-behavioral approaches should routinely be combined with sedative-hypnotic drug therapy to optimize insomnia care and improve treatment outcomes.
J Clin Psychiatry 2026;87(2):26f16467
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
We spend approximately a third of our lives asleep; therefore, from an evolutionary perspective, sleep must be biologically important. Sleep is suggested to be neurorestorative, and a period during which the glymphatic system clears neurotoxic substances from the brain; these substances include amyloid-beta and tau.1 Good sleep is associated with better indices of mental health, cognitive function, endocrine function, immune function, metabolism, cardiovascular health, and other parameters.2 Poor sleep is associated with a wide range of medical and neuropsychiatric disorders.3,4
Scope of This Article
Much has been written about the diagnosis, classification, evaluation, and treatment of insomnia by pharmacologic and nonpharmacologic means.5–8 This article does not repeat what has already been well said; rather, it considers matters, including clinical pearls, that are usually omitted in formal articles; points that clinicians need to know when prescribing medications that induce sleep.
Approvals for treatments for insomnia are mostly based on studies that recruited subjects with primary insomnia or the equivalent thereof; however, medical and mental health professionals commonly treat patients with medical or psychiatric disorders that include insomnia as a symptom. So, it becomes necessary to improvise, and to understand the principles that should drive the improvisation.
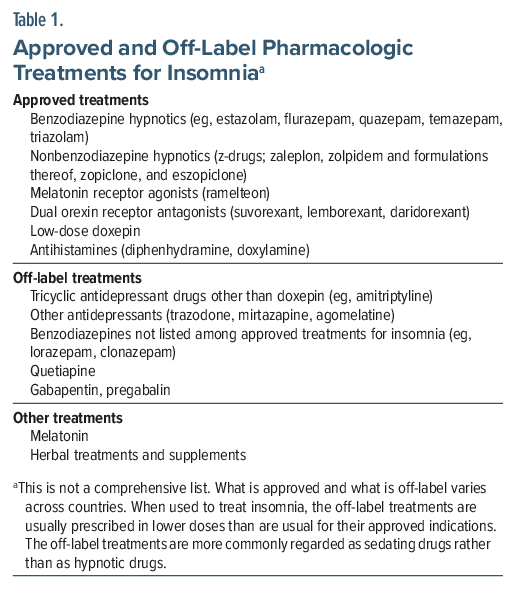
Much of this article presents practical suggestions for the use of approved hypnotics, primarily the z-drugs and the dual orexin receptor antagonists (DORAs); however, the principles apply to all drugs used to treat insomnia (Table 1). This article also presents practical suggestions for the management of excessive sedation in patients who need medications with sedating adverse effects.
Preliminary Notes
As a prelude to prescribing for insomnia, an attempt should be made to identify and address the 3P factors: the factors that predispose to insomnia, those that precipitate insomnia, and those that perpetuate insomnia. These have been well described in other articles.5,8
Some patients have difficulty in falling asleep, others fall asleep easily but awake often during the night, and still others awake early in the morning and cannot fall asleep afterwards. Treatments that work well for sleep-onset insomnia (initial insomnia, early insomnia) are not necessarily treatments that work well for sleep-maintenance insomnia (middle insomnia, late insomnia, terminal insomnia) and vice versa. So, the choice of hypnotic drug will depend on the patient’s need.
Primary insomnia is best treated with z-drugs or the DORAs (Table 1). Insomnia secondary to psychiatric disorders may be treated with add-on sedating medications that are appropriate to the diagnosis, as with low-dose tricyclic antidepressant (TCA) drugs for anxiety or stress-related disorders, quetiapine for mania and nonaffective psychotic disorders, and mirtazapine or a low-dose TCA for depression.
The benzodiazepines and z-hypnotics are usually prescribed for short periods, usually not extending beyond 4 weeks; there is concern that longer use, especially with benzodiazepines, might result in tolerance and dependence. DORA drugs and off-label insomnia drugs are not associated with these concerns and are therefore more commonly used for longer duration prescribing. A list of common approved and off-label drugs for insomnia is presented in Table 1.
Simple clinical evaluations of the severity of insomnia and of the effectiveness of insomnia treatments include inquiries about retiring time and rising time, sleep latency (time between going to bed and sleep onset), number and duration of nighttime awakenings, and total sleep time. Inquiries can also be directed toward quality of sleep, restfulness on awakening, morning hangover, and daytime drowsiness. More enthusiastic clinicians may use any of many available rating scales, visual analog scales, and sleep diaries.
Dosing
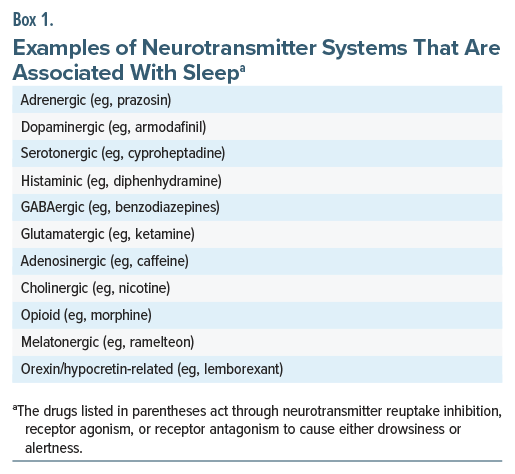
Sleep is an important biological function. Speculatively, this may be why it is regulated in many ways. About a dozen neurotransmitter systems are recognized to influence sleep (Box 1). The practical implication is that perturbation in different/multiple neurotransmitter systems in different patients may necessitate sedative-hypnotic drug doses that are higher than those approved for primary insomnia. As an example, patients with alcohol or substance use disorder may experience persistent insomnia for which conventional hypnotic dosing may be inadequate. Contrariwise, persons who are healthy and who use a hypnotic drug to facilitate sleep in “as-needed” situations may find that low doses suffice.
Z-hypnotics and DORA drugs are mostly metabolized by CYP3A4. Drugs that induce this enzyme may reduce hypnotic efficacy, and drugs that inhibit this enzyme may prolong sedative-hypnotic action; these metabolic drug interactions may necessitate dose adjustments. Cross-tolerance may affect the sleep-inducing properties of a specific dose of a sedative-hypnotic drug in persons with alcohol or substance use disorders or persons who are switching from one sleep-inducing drug to another. Dose discovery for sedative-hypnotic medication is further discussed in a later section.
Absorption of Hypnotic Drugs and Onset of Drowsiness
The z-drugs and DORA drugs are absorbed from the proximal small intestine. Ordinarily, if a patient has not eaten food during the previous 1.5 h to 2 h, the stomach is empty. If the hypnotic is then taken with a glass of water, there is rapid transit of the drug through the stomach and into the small intestine. As absorption occurs and blood levels rise, there is onset of drowsiness. If the patient now lies down and tries to sleep, onset of sleep is usually rapid, well before the drug reaches peak blood level.
Clinically, patients who take a hypnotic drug on an empty stomach commonly feel drowsy within 15–45 min and can fall asleep quickly if they seize the opportunity to lie down when they feel sleepy. Patients should therefore take their hypnotic medication 15–45 min before their planned bedtime.
As a side note, if patients do not lie down and try to sleep when they begin to feel sleepy, and if they wait to finish whatever activity they are engaged in before going to bed, then alertness mechanisms may take over to sustain the activity, the window of opportunity to sleep may be lost, and the benefit of the hypnotic for sleep-onset insomnia may be compromised.
When hypnotics are taken on an empty stomach, the 15–45 min lag in onset of drowsiness depends on many factors. The z-drugs tend to act faster than the DORA drugs. Among different drugs within a group, speed of onset of action may differ; for example, zaleplon is associated with faster onset of action among the z-drugs whereas suvorexant is associated with slower onset of action among the DORAs. Higher doses of hypnotics are associated with faster onset of action because the quantity of drug absorbed per unit time is higher (higher doses will also have a longer duration of action because blood levels take longer to fall below the threshold for efficacy). Onset of drowsiness may be faster in persons who are already preparing to retire to bed relative to those who are engaged in activity.
Once patients understand what their medication does to them and when, they can more easily plan the timing of dosing with regard to their desired bedtime.
The Effect of Food on Absorption and Onset of Drowsiness
If patients take the hypnotic shortly after a meal, because of the time that it takes for the stomach to empty, transit of the hypnotic drug from the stomach to the small intestine is delayed. Worse, the transit occurs in small quantities spread across a longer period of time, perhaps 30–120 min. As a result, absorption of the hypnotic occurs slowly and late. Because the rate of absorption is slower, the rise in blood levels is slower, and the onset of drowsiness is blunted. This may result in reduction in or loss of benefit for sleep-onset insomnia.
The compromise in sleep-onset latency is smaller when the meal is small in quantity and when it is made up more of liquids than solids; the compromise is greater when the meal is large in quantity and high in solid and especially fat content. This is because gastric emptying is faster in the former contexts and slower in the latter contexts.
The clinical message, therefore, is that patients should wait for at least 30–60 min after a small meal or a high liquid meal, at least 60–90 min after a regular meal, and at least 90–120 min after a large or high fat meal before taking a hypnotic drug. Here, “after” refers to after the end of the meal, and not after the start of the meal.
The hypnotic drug should be taken with 100–200 mL of water. If the quantity of water is small, it is less efficient as a vehicle to dissolve the tablet and carry the drug into the small intestine. If the quantity of water is large, nighttime sleep may be disturbed by the need to void urine. After the hypnotic drug has been swallowed, the patient should not snack because the food newly ingested may slow down the transit of the drug into the intestine, and because the surge in glucose levels after the snack may have an activating effect.
This guidance may sound elaborate but is simple, once understood. However, it does call for nighttime meal time, hypnotic dosing time, and bedtime planning. Knowledge about this guidance is important for patients who vary the timing of their nighttime meal, those who tend to snack later at night, and those who do not have a fixed bedtime (the last being a predisposing factor for sleep-onset insomnia).
The Effect of GLP-1RA Drugs on Absorption and Onset of Drowsiness
GLP-1RA and related drugs, such as semaglutide and tirzepatide, delay gastric emptying.9 This effect is greater for solids than for liquids, greater with each dose escalation, and greater earlier during treatment than later during treatment. There is variability between drugs, doses, and time on treatment, and there is interindividual variability, as well. So, it is hard to be precise about the duration of delay in gastric emptying. Patients on GLP-1RAs and related drugs would therefore need to discover on their own what the best time is to take a hypnotic drug after a meal.
The Importance of Drug Half-Life
Zaleplon and immediate-release zolpidem are rapidly absorbed, have short half-lives, and work well for sleep-onset insomnia but are less effective and even ineffective against early morning awakening. Extended-release zolpidem, zopiclone, eszopiclone, and the DORA drugs (especially lemborexant) have longer formulated or actual half-lives and address sleep-maintenance insomnia, as well. Many of the off-label treatments for insomnia are more slowly absorbed than the z-drugs, have longer half-lives, and tend to work better for sleep-maintenance insomnia than for sleep-onset insomnia.
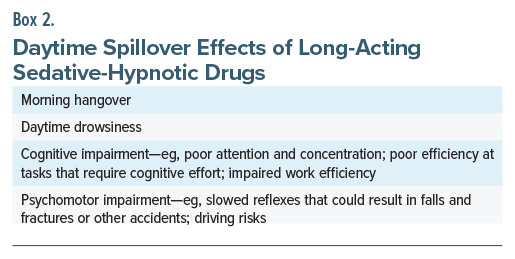
When drug half-life is long, when the drug has active metabolites, and when the sedating effect of the drug is consequently prolonged, patients may sleep for longer than usual. More problematic is when they are drowsy when they awake or are awakened in the morning, when they have an early morning hangover, and when they experience daytime drowsiness. Such spillover effects and their consequences are presented in Box 2.
The choice of drug and dose should therefore be individually optimized, particularly when off-label medications are used. Some strategies are considered in the next section.
Addressing Oversedation With Sedating Psychotropic Drugs
Many psychotropic drugs not listed in Table 1 are sedating but are not used to treat insomnia; examples include olanzapine and clozapine. Sedation observed with these drugs may be desirable when patients are acutely ill and agitated or violent. Sedation that occurs with these drugs is problematic when patients improve, attain stability, enter the maintenance phase of pharmacotherapy, and return to everyday activity, including work.
There are several ways in which prolonged sleep and daytime drowsiness can be addressed in patients who require medications with sedation as an adverse effect, when dose reduction is not an option. The easiest strategy is to administer the nighttime dose during the evening, or shortly before the nighttime meal, such that the onset of drowsiness coincides with planned bedtime. The earlier administration of the drug results in earlier attenuation of morning blood levels, and hence shorter duration of sleep and/or less drowsiness during the morning and daytime.
A second strategy is to split the dose into one or more small doses during the day and the rest of the dose at night. The daytime dose(s) should be sufficiently low as to avoid daytime sedation; and the lower dose administered at night could then be expected to reduce the duration of sleep and the next day sedation. A useful variation of this strategy is to administer part of the dose in the late evening and the rest of the dose at night.
A third strategy is to advise early morning modafinil or armodafinil; a limitation of this strategy is that these drugs are associated with metabolic drug interactions. Modafinil induces CYP1A2, CYP2B6, and CYP3A4, and it inhibits CYP2C9, and CYP2C19. Armodafinil induces CYP3A4 to a moderate extent but does not induce CYP1A2; however, it does inhibit CYP2C19. So, for example, modafinil (and to a lesser extent, armodafinil) could reduce exposure to and hence the efficacy of olanzapine and clozapine.10
As observed in an earlier section, the z-drugs and the DORA drugs are mostly metabolized by CYP3A4. However, these drugs, with the possible exception of lemborexant, are not expected to produce daytime drowsiness, and so modafinil and armodafinil are unlikely to be needed by patients who use these drugs.
A Special Situation: Treating Insomnia with Tranylcypromine
Tranylcypromine (TCP) is a classical monoamine oxidase inhibitor (MAOI) that is associated with risk of all the drug interactions described with the classical MAOIs. Insomnia is a common adverse effect of MAOIs, especially TCP.11 The risk is higher at higher doses.
Most of the approved and off-label treatments for insomnia (Table 1) are compatible with TCP. The TCAs, including doxepin, are important exceptions. Although it is suggested that TCAs in low doses may be used along with MAOIs by clinicians who are experts with MAOIs, this strategy is unlikely to help because sedation with low-dose TCA may not suffice to treat insomnia with TCP.
The use of diphenhydramine is also discouraged because this drug weakly inhibits serotonin reuptake12; there is a risk of serotonin syndrome when diphenhydramine is combined with TCP. The use of quetiapine may also be of concern because quetiapine is metabolized to norquetiapine, which is a norepinephrine reuptake inhibitor.13 Amplification of the noradrenergic activity of norquetiapine by TCP may trigger noradrenergic adverse effects, including constipation and, in men, urinary hesitancy.
The use of trazodone, carefully uptitrated to up to 100 mg/d, may be safe. This is because meaningful serotonin reuptake inhibition with trazodone probably starts from doses of 150 mg/d and above.14 Melatonergic drugs are probably too “mild” to be useful for TCP-induced insomnia.
It is quite likely that, in some patients with TCP-induced insomnia, sedative-hypnotic medications may need to be combined, or prescribed in doses higher than those approved for primary insomnia.
Optimization
When treating conditions such as depression and schizophrenia, we uptitrate the dose, based on efficacy and tolerability, and we augment or switch, based on need. Working with sedative-hypnotic medications can be much the same. It may be necessary to experiment with the suggestions offered in earlier sections of this article to determine what dose of what drug administered in which way works best for which patient. Patients will need to be counseled to observe how taking the drug at different times with regard to meal timing and content, and with regard to planned bedtime, works best for them. Experimentation is best done during the weekend, when suboptimal results will not affect weekday activities.
Reminders to Patients
Patients should be warned that too little sleep as well as too much sleep (with daytime drowsiness) may be associated with cognitive and psychomotor impairments, and with the risks associated therewith (Box 2). Patients who use sedative-hypnotic drugs should also be warned that their psychomotor reflexes may be poor during the night, should they awake to use the bathroom; so, necessary precautions should be taken, such as leaving a dim nightlight on in appropriate places.
Parting Note
Sleep hygiene and cognitive-behavioral approaches should routinely be combined with sedative-hypnotic drug therapy to optimize insomnia care and improve treatment outcomes (of note, good sleep hygiene is usually not sufficient to effectively treat insomnia but is nonetheless a necessary element). These nonpharmacological interventions have been outlined in the scientific literature,5,8,15 presented as patient information material,16 and presented as therapist training material.17 All these resources are freely available online.
Article Information
Published Online: May 25, 2026. https://doi.org/10.4088/JCP.26f16467
© 2026 Physicians Postgraduate Press, Inc.
To Cite: Andrade C. Insomnia, sleep, and the use of sedative-hypnotic drugs: practical notes. J Clin Psychiatry 2026;87(2):26f16467.
Author Affiliations: Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India; Department of Psychiatry, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
Corresponding Author: Chittaranjan Andrade, MD, Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore 560029, India ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
References (17)

- Worth T. Sleep is essential - researchers are trying to work out why. Nature. 2025. doi:10.1038/d41586-025-00964-w. CrossRef
- Knutson KL. Sleep health in human biology research. Am J Hum Biol. 2025;37(3):e70025. PubMed CrossRef
- Gottesman RF, Lutsey PL, Benveniste H, et al. Impact of sleep disorders and disturbed sleep on brain health: a scientific statement from the American Heart Association. Stroke. 2024;55(3):e61–e76. PubMed CrossRef
- Shah AS, Pant MR, Bommasamudram T, et al. Effects of sleep deprivation on physical and mental health outcomes: an umbrella review. Am J Lifestyle Med. 2025:15598276251346752. PubMed CrossRef
- Krystal AD, Prather AA, Ashbrook LH. The assessment and management of insomnia: an update. World Psychiatry. 2019;18(3):337–352. PubMed CrossRef
- Krystal AD. Insomnia medications: history, characteristics, and guidelines for optimal use in clinical practice. J Sleep Res. 2023;32(6):e14084. PubMed CrossRef
- Riemann D, Espie CA, Altena E, et al. The European Insomnia Guideline: an update on the diagnosis and treatment of insomnia 2023. J Sleep Res. 2023;32(6):e14035. PubMed CrossRef
- Sharma MP, Andrade C. Behavioral interventions for insomnia: theory and practice. Indian J Psychiatry. 2012;54(4):359–366. PubMed CrossRef
- Jalleh RJ, Plummer MP, Marathe CS, et al. Clinical consequences of delayed gastric emptying with GLP-1 receptor agonists and tirzepatide. J Clin Endocrinol Metab. 2024;110(1):1–15. PubMed CrossRef
- Andrade C. Modafinil and armodafinil in schizophrenia. J Clin Psychiatry. 2012;73(8):e1062–e1064. PubMed CrossRef
- Birkenhäger TK, van den Broek WW, Mulder PG, et al. Efficacy and tolerability of tranylcypromine versus phenelzine: a double-blind study in antidepressant-refractory depressed inpatients. J Clin Psychiatry. 2004;65(11):1505–1510. PubMed CrossRef
- Tanaka T, Takasu A, Yoshino A, et al. Diphenhydramine overdose mimicking serotonin syndrome. Psychiatry Clin Neurosci. 2011;65(5):534. PubMed CrossRef
- Nyberg S, Jucaite A, Takano A, et al. Norepinephrine transporter occupancy in the human brain after oral administration of quetiapine XR. Int J Neuropsychopharmacol. 2013;16(10):2235–2244. PubMed CrossRef
- Goldberg JF, Steinman MQ, Stahl SM. Trazodone once-a-day: a formula for addressing challenges in antidepressant safety and tolerability. Neurosci Appl. 2023;2:101127. PubMed CrossRef
- Walker J, Muench A, Perlis ML, et al. Cognitive behavioral therapy for insomnia (CBT-I): a primer. Klin Spec Psihol. 2022;11(2):123–137. PubMed CrossRef
- Centre for Clinical Interventions; Psychotherapy, Research, and Training. Sleep hygiene. https://www.cci.health.wa.gov.au/∼/media/CCI/Mental-Health-Professionals/Sleep/Sleep—Information-Sheets/Sleep-Information-Sheet—04—Sleep-Hygiene.pdf. Accessed April 10, 2026
- Edinger JD. Treatment Manual: Cognitive-Behavioral Insomnia Therapy. https://www.med.unc.edu/neurology/wp-content/uploads/sites/716/2018/05/jdedingrCBTManual.pdf. Accessed April 10, 2026
This PDF is free for all visitors!