Abstract
Cholesterol is the most important sterol in the body. In the brain, it is an essential component of nerve cell membranes, myelin sheaths, and synapses. It is also a precursor for adrenocortical hormones, sex hormones, and vitamin D. Hypothetically, therefore, disruption of sterol biosynthesis in utero may impair fetal brain development. In this context, a recent study found that gestational exposure to sterol biosynthesis–inhibiting medications (SBIMs) was associated with an increased risk of autism spectrum disorder (ASD) in offspring; the SBIMs included 4 antidepressants, 3 antipsychotics, 1 anxiolytic, 3 beta-blockers, and 4 statins. The study also reported that drugs that inhibited the final step of cholesterol biosynthesis resulted in elevated levels of 7-dehydrocholesterol, and that these levels were strongly correlated with the risk of ASD in offspring. The present article argues that the SBIM study did not use statistical methods, comparison groups, and research designs that could have helped address confounding by indication and confounding by severity of indication. As a result, the association between gestational exposure to SBIMs and risk of ASD in offspring could have resulted from confounding by maternal behavioral and physiological characteristics related to illness, genetic variables related to illness, and/or familial environmental variables related to illness. Furthermore, in the 7-dehydrocholesterol analysis, the authors used a statistical approach that was flawed in more than one way. The study found that gestational exposure to drugs that do not disrupt sterol biosynthesis also increased the risk of ASD in offspring; this weakens the SBIM hypothesis. The study had other limitations, as well. The authors nevertheless suggested that providers and women be educated about SBIM risks. This is premature. Recommendations against the use of necessary medications during pregnancy should not be based on speculations tested using inappropriate statistical and research methods. This is particularly important when the medications are necessary for the physical and mental health of the mother, and the well-being of the mother and of the pregnancy.
J Clin Psychiatry 2026;87(3):26f16520
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
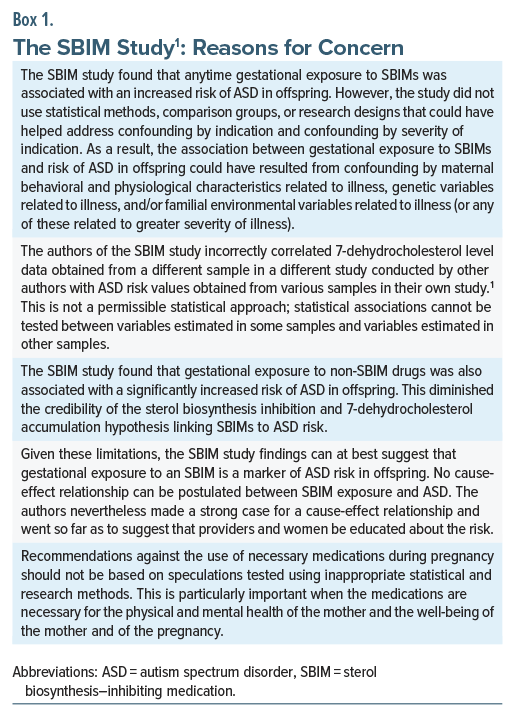
A recent study,1 published as an “immediate communication,” proposed a novel hypothesis: that gestational exposure to drugs that disrupt sterol biosynthesis may increase the risk of autism spectrum disorder (ASD) in offspring. The study examined and identified risks with a wide range of drugs, and, if the findings are valid, the implications are far-reaching. The present article, therefore, critically examines this study and suggests that whereas there is reason to consider further research, there are no grounds, as yet, for the reported findings to change clinical practice. Important messages are presented in Box 1.
Sterols
The steroid skeleton has a 4-ring, 17-carbon structure; when a hydroxyl ion is bound to the third carbon atom, the structure is known as a sterol. Sterols are essential components of cell membranes in plants and animals and differ from each other largely in their side chains.2
Cholesterol
Cholesterol is the best known sterol and is the most important sterol in the human body. It is an essential component of cell membranes and, in the brain, is an essential component not only of nerve cell membranes but also of myelin sheaths and synapses. Furthermore, cholesterol is a precursor for important biological agents such as the adrenocortical hormones, sex hormones, vitamin D, and bile acids.3–5
Cholesterol Biosynthesis
Most of the cholesterol in the human body is endogenous in origin; that is, not derived from diet. A widely cited figure here is 70%–80% for both serum cholesterol and total body cholesterol,6,7 though the original studies that led to this estimate are hard to identify.
Most of the cholesterol in the body is synthesized in the intestine and liver, but the cholesterol in the brain probably originates from synthesis in the brain, alone.5 The biosynthesis of cholesterol starts with acetyl coenzyme A and proceeds through nearly 30 enzymatic reactions, via an intermediary, lanosterol, to cholesterol.8 Importantly, there is more than one route along the biosynthesis path.3 Additionally, cholesterol homeostasis in both health and disease is complex and is dynamically regulated.8
Interference With Cholesterol Biosynthesis
Many drugs interfere with cholesterol biosynthesis. For example, bempedoic acid and statins act at an early stage along the biosynthesis pathway (side note: other cholesterol lowering drugs, ezetimibe and PCSK9 inhibitors, do not interfere with cholesterol biosynthesis). Some drugs, however, act at a late stage in the biosynthesis pathway; these drugs include antidepressants such as bupropion and fluoxetine, and antipsychotics such as aripiprazole and haloperidol.
Interference With Cholesterol Biosynthesis During Pregnancy
Given the structural importance of cholesterol in the human brain, and its functional importance as a precursor for important biological substances (discussed in an earlier section), Peeples et al1 speculated that interference with cholesterol biosynthesis during intrauterine life may adversely affect fetal brain development. They cited the Smith–Lemli–Opitz syndrome (SLOS) in support.
The Smith-Lemli-Opitz Syndrome
SLOS is a genetic disorder characterized by impaired conversion of 7-dehydrocholesterol (7-DHC) to cholesterol in the final step of the cholesterol biosynthesis pathway. This results in higher levels of 7-DHC and lower levels of cholesterol. Higher levels of 7-DHC may be potentially harmful to the developing brain.1 Interestingly, SLOS has been associated with ASD. In one small study of 14 children with SLOS, ASD was diagnosed in 71%–86% of children, depending on the method of evaluation.9 Peeples et al1 therefore examined the association between gestational exposure to drugs that disrupt sterol biosynthesis and risk of ASD in offspring.
Drugs That Disrupt Sterol Biosynthesis
Peeples et al1 studied 15 sterol biosynthesis–inhibiting medications (SBIMs). These were statins (atorvastatin, pravastatin, rosuvastatin, and simvastatin), antidepressants (bupropion, fluoxetine, sertraline, and trazodone), antipsychotics (aripiprazole, cariprazine, and haloperidol), anxiolytics (buspirone), and beta-blockers (metoprolol, nebivolol, and propranolol). They also studied 6 “comparator drugs” that do not interfere with sterol biosynthesis. These were diphenhydramine, docusate sodium, famotidine, ferrous sulfate, ondansetron, and polyethylene glycol.
As a critically important side note here, in pooled as well as in drug-specific analyses, the authors1 examined subjects exposed to SBIMs vs subjects unexposed to SBIMs; and they examined subjects exposed to the “comparators” vs subjects unexposed to the “comparators.” So, the “comparator” arms were not control arms; they were actually exposure arms examined in separate analyses that were unconnected with the SBIM analyses. Findings from the SBIM analyses were presented separately from findings from the comparator analyses.
The SBIM Study: Sample and Methods
The authors1 used the Epic Cosmos health systems database in the US to create multiple pregnancy cohorts that were exposed vs unexposed to the SBIM and comparator drugs during 2014–2023 and followed up to January 2026; pregnancies exposed to valproate were excluded. The overall sample included 6,135,213 subjects; sample size in individual analyses depended on SBIM (or comparator) exposure and so were far smaller.
The overall sample was 54% white. The mean age of the women was 30 years. Diabetes was the commonest (15%) medical comorbidity in these women. Hypertensive disorders of pregnancy occurred in 11%.
Anxiety (68% vs 18%), depression (50% vs 10%), and bipolar disorder (10% vs 2%) were commoner in pregnancies exposed (n=699,692) vs unexposed (n =5,435,521) to SBIMs. Exposure was defined as medication order, prescription, dispensation, or administration, the occurrence or duration of which overlapped with any period during pregnancy. No information was gathered for dose of drug, duration of use, period of pregnancy during which the exposure occurred, etc.
Delivery occurred at a mean of 39.1 weeks, but 11% of these deliveries were preterm. The offspring were 52% male. ASD was diagnosed in 5.0% vs 3.7% of pregnancies exposed vs unexposed to SBIMs.
Cox proportional hazard regression analyses were adjusted for maternal age, race, ethnicity, pre-pregnancy body mass index, diabetes, hypertensive disorders of pregnancy, birth year, urban/rural residence, social vulnerability, and alcohol and tobacco use during pregnancy. Sensitivity analyses adjusted for psychiatric diagnoses and their statistical interactions with drug exposure.
The SBIM Study: Results
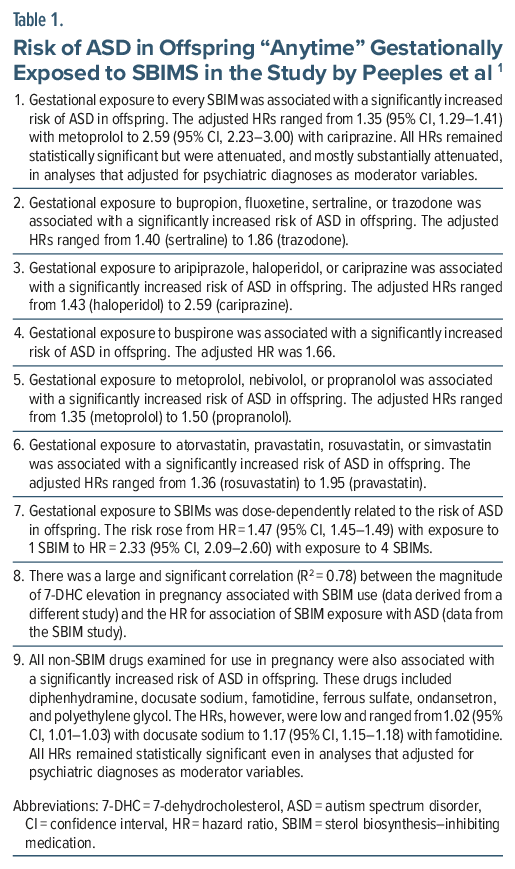
Important findings from the study are presented in Table 1. In summary, gestational exposure (anytime during pregnancy) to every SBIM was associated with a significantly increased risk of ASD in offspring (hazard ratio [HR] range, 1.35–2.59). The risk was dose-dependent, rising from HR =1.47 with exposure to 1 SBIM to HR =2.33 with exposure to 4 SBIMs. Higher levels of 7-DHC (with SBIMs) were strongly correlated with higher HR values for ASD risk. Interestingly, gestational exposure to non-SBIM drugs was also associated with a significantly increased risk of ASD in offspring, but the HR range was lower (from 1.02 to 1.17).
Limitations of the SBIM study
The authors1 acknowledged many limitations of their study. They could not study interactions between the SBIMs and known genetic variants in sterol biosynthesis. They adjusted their analyses for very few comorbidities, and very few of the very many known risk factors for ASD.10 They could not examine the effect of dose and duration of SBIM exposure, nor the effect of exposure during specific trimesters of pregnancy.
There were many far more important limitations that they did not acknowledge. These are addressed in the sections that follow.
Limitations: Confounding by Indication and Confounding by Severity of Indication
The authors 1 conducted more than two dozen time-to-event regressions. In each regression, they compared SBIM-exposed with SBIM-unexposed pregnancies. In all of these analyses, the composition of the unexposed cohorts did not address confounding by indication.
This is a critically important limitation because a large body of evidence suggests that, in pregnancies exposed to psychotropic drugs, adverse outcomes such as ASD may be due to inadequately measured, unmeasured, and unknown confounds. These confounds include parental genes, parental environment, and parental health-related variables. These confounds, rather than exposure to the psychotropic drugs, may be responsible for ASD in offspring.11
The authors presented sensitivity analyses that adjusted for psychiatric diagnoses, but the analyses remained vulnerable to confounding; that is, confounding by severity of indication for the psychiatric diagnoses (in the psychotropic drug SBIM analyses), and confounding by indication for diagnoses for which the statins and beta-blockers were indicated (in the nonpsychotropic drug SBIM analyses). This is considered further in the next section.
The authors found that gestational exposure to more than 1 SBIM was dose-dependently associated with risk of ASD in offspring. This finding could merely have been a result of confounding by more than 1 indication.
Given the known overlap between the genes for psychiatric disorders and the genes for ASD, and the possible relationship between exposure to maternal illness variables and familial environment variables on the one hand and risk of ASD on the other, the study findings (Table 1) can only suggest that gestational exposure to an SBIM is a marker of ASD risk in offspring. No cause-effect relationship can be postulated between SBIM exposure and ASD.
Approaches to Address Confounding by Indication: Adjustment for Diagnosis Using Regression
On the surface, it could seem that adjustment for diagnosis (in regressions) could address confounding by indication. However, this is not so (Box 2). As an example, consider that the SBIM cariprazine is prescribed to patients with major mental illness and not to healthy persons. So, if major mental illness is adjusted for, to whom would cariprazine have been prescribed?
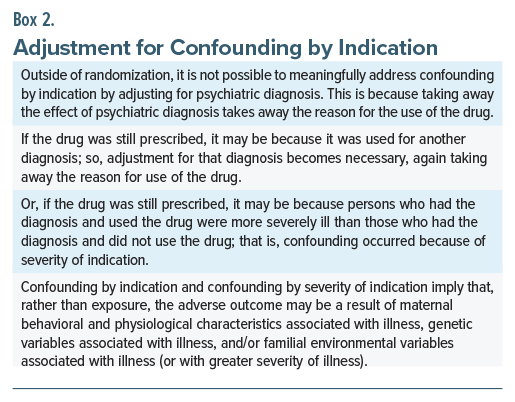
It is possible that, in some women, cariprazine was withheld during pregnancy to avoid gestational exposure to this drug. If so, this would allow meaningful adjustment for diagnosis in regression. However, if so, it is likely that cariprazine would have been withheld only in women with milder illness; so, confounding would persist, here, as confounding by severity of indication (Box 2). In such a situation, maternal behavioral and physiological characteristics associated with more severe illness may drive the risk of ASD in offspring. Or, genetic or familial environmental variables associated with greater severity of illness may drive the risk. Either way, cariprazine would remain a marker of risk rather than the cause of risk.
Other Approaches to Address Confounding by Indication
Statistical approaches, beyond adjustment for diagnosis, can help address confounding by indication. Propensity score matching is one such procedure. However, this method is based on matching for measured variables. It does not match for unmeasured and unknown confounds.12
Innovative research designs may be considered; target trial emulation is an example. However, target trial emulation is also limited by an inability to adjust for unmeasured and unknown confounds.13
The SBIM study authors1 could have considered alternatives as control groups. An example is disease controls; pregnancies with the diagnosis that were vs were not exposed to the SBIMs. This would remove the need to adjust for diagnosis but would not address confounding by severity of indication. Another and better possibility would have been to use, as controls, pregnancies exposed to other drugs from the same class, specifically drugs that have not been identified as SBIMs. As an example, pregnancies exposed to fluoxetine could have been compared with pregnancies exposed to escitalopram. The latter, at least in 1 study,14 has been suggested to not interfere with sterol biosynthesis and to not raise 7-DHC levels.
Other important approaches that address confounding by indication, confounding by parental genetic risk factors, and confounding by familial environmental risk factors include pre-pregnancy exposure analysis, postpregnancy exposure analysis, paternal exposure analysis, and discordant sibling pair exposure analysis.11
The SBIM study authors1 did not use any of the approaches considered in this section. So, their findings, at best, suggest scope for future research with no implications for change in current clinical practice.
Limitation: The 7-DHC Analysis
For the 7-DHC analysis (Table 1, Finding 8), the SBIM study authors1 took the values for a predictor (7-DHC; independent variable) from a different study15 and correlated those values with outcome values (HRs for ASD; dependent variable) from their own study. This is not a permissible statistical approach; statistical associations cannot be tested between variables estimated in one study and variables estimated from another study. The authors should have obtained 7-DHC data from their own cohorts and correlated these with the corresponding HRs obtained in these cohorts. An even better though more challenging approach would have been to study 7-DHC as a mediating variable.
As a relevant side note here, the data extracted from the external study15 were potentially fallacious. The authors15 did not study elevations of 7-DHC in blood samples of pregnancies exposed to SBIMs; rather, they studied a subset of blood samples in which 7-DHC levels were markedly elevated and then examined these samples for the presence of SBIMs. Interestingly, this subset comprised 302 (23%) of 1,312 samples (sampling criteria not stated) “showing 7-DHC levels above the 99% mean confidence of interval,” whatever that means.
The 7-DHC correlational analysis included just 7 data points; from a statistical perspective, correlations with such limited data are suspect. Furthermore, 2 data points were clearly outliers; if these are disregarded, the data points appear to aggregate randomly, without a clear indication of correlation.
Thus, the 7-DHC analysis and the conclusions drawn from the analysis were based on multiple erroneous processes.
The Verdict of the SBIM Authors
The SBIM authors,1 in the final section of their paper, argued strongly in favor of their hypothesis that gestational exposure to sterol biosynthesis disruptors increases the risk of ASD in offspring. They went so far as to recommend that providers be educated and women be advised about the potential effects of SBIMs on pregnancy and offspring outcomes.
General Conclusions and Take-Home Message
ASD is multifactorial; there are several dozen, perhaps more than a hundred risk factors for the disorder.10 This is crucial to recognize when attention and adverse opinion are focused only on medications, particularly medications that are important for the physical and mental health of the mother, and the well-being of the mother and of the pregnancy. Recommendations against the use of necessary medications during pregnancy should not be based on speculations tested using inappropriate statistical methods and research designs.
Article Information
Published Online: June 15, 2026. https://doi.org/10.4088/JCP.26f16520
© 2026 Physicians Postgraduate Press, Inc.
To Cite: Andrade C. Gestational exposure to sterol biosynthesis disrupting drugs and risk of autism spectrum disorder in offspring. J Clin Psychiatry 2026;87(3):26f16520.
Author Affiliations: Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India; Department of Psychiatry, Kasturba Medical College, Manipal Academy of Higher Education, Manipal, India.
Corresponding Author: Chittaranjan Andrade, MD, Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore 560029, India ([email protected]).
Relevant Financial Relationships: None.
Funding/Support: None.
 Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Each month in his online column, Dr Andrade considers theoretical and practical ideas in clinical psychopharmacology with a view to update the knowledge and skills of medical practitioners who treat patients with psychiatric conditions.
Department of Clinical Psychopharmacology and Neurotoxicology, National Institute of Mental Health and Neurosciences, Bangalore, India. Please contact Chittaranjan Andrade, MD, at Psychiatrist.com/contact/andrade.
References (15)

- Peeples ES, Anzalone AJ, Dai R, et al. Sterol pathway disruption in pregnancy: a link to autism. Mol Psychiatry. 2026. doi:10.1038/s41380-026-03610-7. PubMed CrossRef
- Yalcinkaya A, Öztaş YE, Sabuncuoğlu S. Sterols in inflammatory diseases: implications and clinical utility. Adv Exp Med Biol. 2024;1440:261–275. PubMed CrossRef
- Nes WD. Biosynthesis of cholesterol and other sterols. Chem Rev. 2011;111(10):6423–6451. PubMed CrossRef
- Ikonen E. Cellular cholesterol trafficking and compartmentalization. Nat Rev Mol Cel Biol. 2008;9(2):125–138. PubMed CrossRef
- Dietschy JM, Turley SD. Thematic review series: brain lipids. Cholesterol metabolism in the central nervous system during early development and in the mature animal. J Lipid Res. 2004;45(8):1375–1397. PubMed CrossRef
- Blesso CN, Fernandez ML. Dietary cholesterol, serum lipids, and heart disease: are eggs working for or against you? Nutrients. 2018;10(4):426. PubMed CrossRef
- Kapourchali FR, Surendiran G, Goulet A, et al. The role of dietary cholesterol in lipoprotein metabolism and related metabolic abnormalities: a mini-review. Crit Rev Food Sci Nutr. 2016;56(14):2408–2415. PubMed CrossRef
- Duan Y, Gong K, Xu S, et al. Regulation of cholesterol homeostasis in health and diseases: from mechanisms to targeted therapeutics. Signal Transduct Target Ther. 2022;7(1):265. PubMed CrossRef
- Sikora DM, Pettit-Kekel K, Penfield J, et al. The near universal presence of autism spectrum disorders in children with Smith-Lemli-Opitz syndrome. Am J Med Genet. 2006;140(14):1511–1518. PubMed CrossRef
- Andrade C. Autism spectrum disorder, 1: genetic and environmental risk factors. J Clin Psychiatry. 2025;86(2):25f15878. PubMed CrossRef
- Andrade C. Gestational exposure to antidepressants and neurodevelopmental disorders in offspring. J Clin Psychiatry. 2025;87(1):25f16226. PubMed CrossRef
- Andrade C. Propensity score matching in nonrandomized studies: a concept simply explained using antidepressant treatment during pregnancy as an example. J Clin Psychiatry. 2017;78(2):e162–e165. PubMed CrossRef
- Andrade C. Target trial emulation: a concept simply explained. J Clin Psychiatry. 2025;86(1):25f15796. PubMed CrossRef
- Korade Ž, Liu W, Warren EB, et al. Effect of psychotropic drug treatment on sterol metabolism. Schizophr Res. 2017;187:74–81. PubMed CrossRef
- Genaro-Mattos TC, Klingelsmith KB, Allen LB, et al. Sterol biosynthesis inhibition in pregnant women taking prescription medications. ACS Pharmacol Transl Sci. 2021;4(2):848–857. PubMed CrossRef
This PDF is free for all visitors!