Abstract
Objective: Aftercare interventions following self-harm may prevent subsequent self-harm and suicide deaths. However, previous research into the effectiveness of aftercare services on self-harm repetition and suicide mostly comprised a small sample size and showed inconsistent findings. We investigated the effectiveness of Taiwan’s national self-harm aftercare program on self-harm repetition and suicide among self-harm patients.
Methods: A cohort study of 90,413 index self-harm episodes (ie, the first episode during the study period) presented to hospitals and registered in the National Suicide Surveillance System (2012–2016) was performed. Cox regression models were used to evaluate the risk of self-harm repetition or suicide after receiving the aftercare, which was modeled as a time-varying variable.
Results: The aftercare was associated with a 17% (adjusted hazard ratio [aHR]=1.17, 95% confidence interval [CI] 1.14–1.21) increase in self-harm repetition risk and a 20% (aHR=0.80, 95% CI 0.74–0.86) decrease in suicide risk. The association of the aftercare with increased self-harm repetition risk was most marked in patients aged 45–64 years (aHR=1.34) and more marked in those with a history of psychiatric disorders (aHR=1.26). The association of aftercare with decreased suicide risk was most marked in patients aged 10–24 years (aHR=0.64) and more marked in those without a history of psychiatric disorders (aHR=0.76) than their counterparts.
Conclusion: The aftercare following self-harm was associated with an increased risk of repeat self-harm hospital presentation and decreased risk of suicide. The findings suggest that the aftercare intervention may increase help-seeking behaviors after self-harm and decrease suicide deaths, especially in specific subgroups.
J Clin Psychiatry 2026;87(3):25m16173
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Globally, an estimated over 700,000 people die by suicide every year,1 accounting for 2% of total years of life lost.2 Many more people attempt suicide.3 A history of suicide attempts is the single most important risk factor for suicide.3 A meta-analysis showed that the risk of suicide and nonfatal repeat self-harm within one year after the index self-harm episode was 1.6% and 16.3%, respectively, among self-harm patients.4 The recently published UK NICE guideline for the assessment and management of self-harm5 and the World Health Organization’s (WHO’s) guide for suicide prevention6 recommended follow-up care (ie, aftercare) for patients who self-harmed or attempted suicide, particularly for patients with ongoing safety concerns.
Although there are emerging interests in developing and promoting follow-up care for people with a potentially increased risk of suicide, studies on the effectiveness of such follow-up interventions in reducing subsequent suicidal behaviors have shown mixed results. Several meta-analyses indicated that active contacts and aftercare interventions for self-harm patients presenting to emergency departments,7 brief aftercare interventions for patients with identified suicide risk,8 and brief contact interventions for mental health patients9 were effective in reducing repeat self-harm episodes.
Nevertheless, a Cochrane review suggested that the effect estimate of telephone contacts on self-harm repetition at postintervention is limited; there is only uncertain evidence regarding a number of psychosocial interventions for self-harmed adults.10 A recent study from the US found that offering care management or brief dialectical behavioral therapy for adult outpatients with suicide ideation did not reduce but may increase the self-harm risk, when compared with usual care.11 An earlier study from the UK reported that self-harm repetition was more common in those who received aftercare intervention.12
The evidence of the effectiveness of aftercare interventions on reducing suicide has also been mixed. The WHO’s multisite intervention study in six low- and middle-income countries showed that the suicide attempters in the brief intervention and contact group presented with fewer subsequent suicide deaths than those in the treatment-as-usual group,13 while the two groups had a similar proportion of self-harm repetitions.14 Based on a pooled sample of 2,521 and 2,663 patients in the intervention and control groups, a recent meta-analysis of randomized controlled trials showed a statistically nonsignificant effect of brief contact interventions on reducing suicide deaths among discharged mental health patients (odds ratio=0.74, 95% confidence interval [CI] 0.20–2.81).9 A larger sample size is required when evaluating the suicide prevention effect of an intervention because of the rarity of the suicide death outcomes.15
In Taiwan, the National Suicide Surveillance System (NSSS) was launched in six pilot cities in 2006 and aimed to monitor and provide aftercare for people presenting with self-harm.16 Follow-up aftercare services, mainly by telephone calls and supplementally by in-person contacts, were provided to the registered individuals. A previous assessment of the NSSS aftercare intervention in the pilot phase (2006-2008) showed a 22%–64% reduction in the risk of subsequent suicide deaths among those who received aftercare compared with those who did not.16 The NSSS aftercare program was later rolled out to the whole country in 2009, while its effectiveness on reducing subsequent self-harm and suicide was never assessed.
This study aimed to investigate the effectiveness of Taiwan’s nationwide self-harm aftercare program on the risk of self-harm repetition and subsequent suicide. Findings from a nationwide program implemented in a real-world setting can inform suicide prevention strategies, resource allocation, and policy decisions in Taiwan and other countries considering the implementation or expansion of systematic aftercare services for individuals presenting to healthcare services with self-harm.
METHODS
Patients
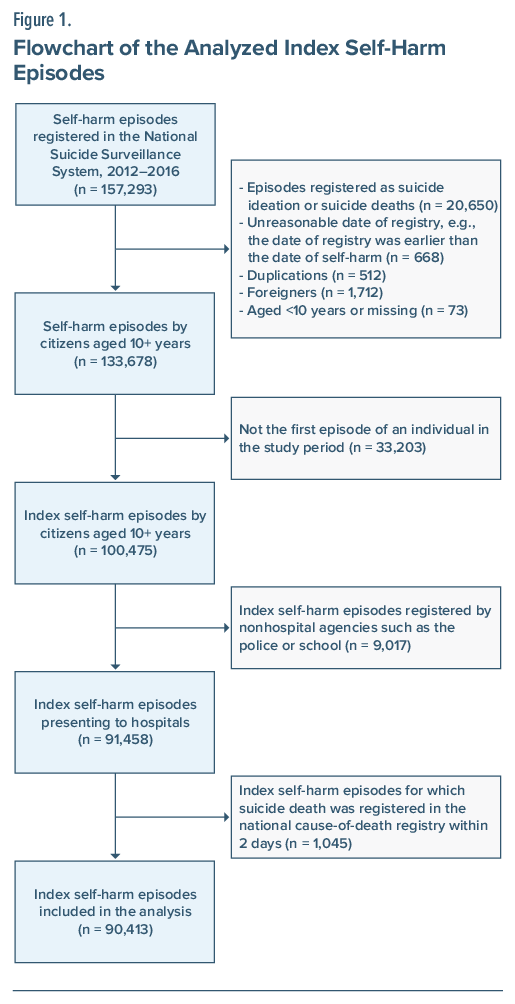
Data for self-harm patients in 2012–2017 were extracted from the NSSS. The NSSS was established in 2006 to monitor suicidal events, including suicide ideation, self-harm, and suicide deaths, and was expanded to the whole country in 2009.16 Information on the date and methods of self-harm, demographic characteristics, and residential address was collected for all registered suicidal events reported by agencies, including hospitals, the police, firefighters, and schools. We analyzed data of individuals’ first nonfatal self-harm episode during the study period (ie, the index episode) after excluding noneligible episodes (see Figure 1). Self-harm was defined as intentional self-poisoning or self-injury, irrespective of the motivation and degree of suicidal intent.17 We restricted our analysis to self-harm episodes presenting to hospitals only, for which the registration of self-harm was considered to be more comprehensive than those reported by other agencies. A previous report from Taoyuan, a major city in Taiwan, showed that self-harm episodes reported by individual nonhospital agencies, such as the police, firefighting services, or schools, accounted for less than 3% of all registered self-harm episodes prior to 2019, suggesting substantial underreporting of self-harm episodes from these nonhospital sources.18
Aftercare Intervention
The NSSS is linked to an aftercare service that provides follow-up care, in which the aftercare workers contact the self-harm patients by telephone or in person and provide brief suicide risk assessments, psychological support, and referrals to health or social services where appropriate. The aftercare workers mostly have bachelor’s degrees in psychology, social work, or nursing.19 According to the aftercare guideline issued by the Ministry of Health and Welfare, the first contact with the self-harm patients should occur within three days after the self-harm episode, and the aftercare service would last for three months (ie, around 90 days), with a minimum of two contacts per month over the period.20 During 2012–2016, 35.2% of the self-harm patients (n =36,321) did not receive aftercare; this could be because the person refused the care or could not be reached. Among those who received aftercare (n=54,092; 64.8% of the total sample), the majority received the first contact within 90 days (92.4%) or 180 days (99.3%) after self-harm. The median interval between the index self-harm and the first aftercare contact was 12 days (range 0–364 days) among self-harm patients who received the aftercare; the corresponding figure was 9 days (range 0–90 days) for those who received the aftercare within 90 days.
Outcome
Data of the self-harm patients (2012–2016) were linked to the national cause-of-death data files (2012–2017) using the unique identification number to identify subsequent suicides, ensuring at least one-year follow-up for all patients. If the registered date of suicide occurred within two days of the index self-harm episode, the index episode was classified as a fatal event and excluded from the analysis. These cases likely represent individuals who were alive at presentation but died shortly thereafter from the medical consequences of the initial suicidal act. Some deaths within this short interval may have resulted from a separate suicidal act; however, the NSSS data do not include sufficient detail to distinguish between these scenarios. Deaths by suicide were identified using the International Classification of Diseases, Tenth Revision (ICD-10), codes X60–X84. We additionally included deaths certified as undetermined death (Y10–Y34), accidental pesticide poisoning (X48), and accidental suffocation (W75–W76, W83–W84), as a previous study from Taiwan showed that many of these deaths were likely to be misclassified suicides.21 For simplicity, we used the term suicide when referring to both certified suicides and possible suicides throughout the paper.
Data from the NSSS (2012–2017) were used to identify self-harm repetition after the index self-harm, defined as any subsequent self-harm episodes presenting to hospitals after the index episode (2012–2016), ensuring at least one-year follow-up for all episodes.
Covariates
The self-harm method, sex, age, marital status, educational level, area median household income, and a history of psychiatric disorders, physical comorbidities, and hospitalizations were included as covariates. The NSSS provided data for self-harm method, sex, age, marital status, and educational level. Data for area median household income were from the Income Tax Statistics (2012–2016) based on the district of residence (n=368). We linked the self-harm data to Taiwan’s National Health Insurance Research Database (NHIRD) to extract data for psychiatric disorders, physical comorbidities, and hospitalizations in the previous year of the index self-harm episode. Approximately 99.8% of Taiwan’s population was enrolled in the National Health Insurance.22 The NHIRD includes information on the beneficiaries’ medical contacts, using the ICD, Clinical Modification (ICD-CM), to code the physicians’ diagnoses (ICD-9-CM for 2012–2015 and ICD-10-CM for 2016). Six categories of psychiatric disorders—depressive disorders, anxiety disorders, bipolar disorders, schizophrenia, substance use disorders, and personality disorders—were identified using specific ICD codes. The details of ICD codes used are provided in Supplementary Table 1. Each self-harm patient could be diagnosed with more than one category of psychiatric disorders.
Physical comorbidities were assessed using the Charlson Comorbidity Index (CCI) score. The CCI score considers 19 physical conditions for which weighted scores equal to 1, 2, 3, or 6 are assigned based on the severity of the conditions.23 The CCI score was calculated by summing up the weighted scores for all comorbidities. Any psychiatric and nonpsychiatric hospitalizations in the previous year of the index self-harm episodes were identified.
Analysis
We calculated the number and percentage of patients according to the covariates in the total sample and two groups (ie, patients who received vs did not receive the aftercare within 90 days after self-harm). Chi-square tests were used to examine the differences in characteristics between the two groups. We calculated the number of events (self-harm repetition or suicide), the person-years of follow-up, and the incidence rates of events, in the total sample and by aftercare exposure status. In this study, we defined the patients’ aftercare exposure status as a time-varying variable. For patients who received the aftercare service and the first aftercare contact occurred within 90 days after self-harm, the follow-up period (person-time) before receiving the first aftercare contact was classified as the nonexposed group, and the follow-up period after receiving the first aftercare contact until the end of follow-up was classified as the exposed group. By contrast, for patients who received the aftercare and the first contact occurred more than 90 days after the self-harm and those who did not receive the aftercare throughout, all the follow-up periods were classified as the nonexposed group. The cutoff of 90 days was chosen as the aftercare guideline indicated that the duration of the aftercare service should be 90 days. The follow-up period started from the date of self-harm and ended on the date of repeat self-harm (in the analysis of using self-harm repetition as the outcome) or the date of death or the end of the study period (in the analyses of using self-harm repetition or suicide as the outcome), whichever came first.
Cox proportional hazards regression models with a time-varying covariate (ie, the aftercare exposure) were used to examine the association of the aftercare intervention with the risks of self-harm repetition or suicide during the follow-up period. Hazard ratios (HRs) and their 95% CIs were estimated before and after controlling for covariates. Stratified analyses by sex, age, and history of psychiatric disorders were also conducted. Three sensitivity analyses were conducted. The first sensitivity analysis included only certified suicides (ICD-10 X60–X84) when investigating the effect of the aftercare intervention on suicide. In the second sensitivity analysis, the cutoff of aftercare exposure status was defined as the first aftercare contact that occurred within 180 days after self-harm. The third sensitivity analysis adjusted for differences in characteristics between the exposed and nonexposed groups using the propensity score deciles when investigating the effect of the aftercare intervention on self-harm repetition or suicide. The propensity score was calculated by including all covariates in the logistic regression model. All the analyses were conducted using SAS version 9.4 (SAS Institute Inc., Cary, NC).
RESULTS
Taiwan’s NSSS registered a total of 157,293 self-harm episodes and suicidal events between 2012 and 2016 (Figure 1). After excluding noneligible episodes, a total of 90,413 index nonfatal self-harm episodes presenting to hospitals by Taiwanese citizens aged 10+ years were included in the analysis. In the study sample, 57,812 (63.9%) were females, and 42,536 (47.1%) were aged 25–44 years at the time of the index self-harm episode (Table 1). The main methods for self-harm were overdose (47.1%) and cutting (22.7%). A total of 42% of patients received a diagnosis of psychiatric disorders in the previous year; the prevalence of psychiatric disorders was highest for depressive disorders (27.3%) and lowest for personality disorders (2.1%). The majority (97.9%) had no physical comorbidities in the previous year. A total of 5.6% and 19.5% of patients had psychiatric and nonpsychiatric hospitalizations within one year prior to their self-harm, respectively.
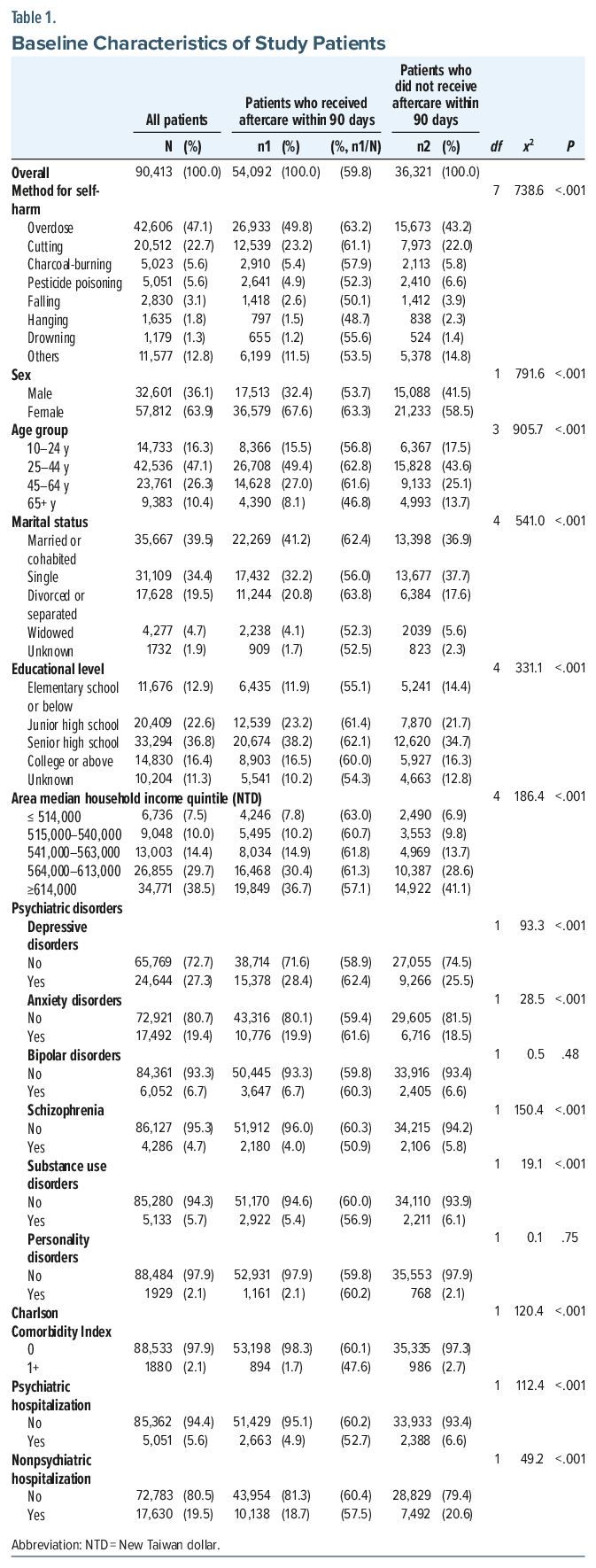
Approximately three-fifths (59.8%; n=54,092) of patients received aftercare within 90 days. Those who received aftercare within 90 days were more likely to use overdose or cutting for self-harm and be female, aged 25–64 years, and married/cohabited or divorced/separated than their counterparts (Table 1). They were also more likely to have a junior high school or above education and live in areas with lower household incomes. In the year before self-harm, they were more likely to receive a diagnosis of depressive disorders and anxiety disorders but were less likely to have schizophrenia, substance use disorders, comorbid physical conditions, or psychiatric or nonpsychiatric hospitalizations.
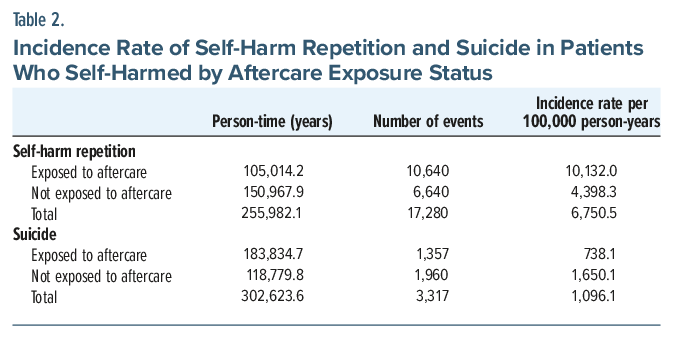
During a mean follow-up of 2.8 years, 17,280 (19.1%) patients repeated self-harm, while 3,317 (3.7%) died by suicide during a mean follow-up of 3.3 years (the average follow-up period was longer for suicide due to a much lower number of outcome events) (Table 2). The incidence rate of self-harm repetition for the exposed group was higher than that for the nonexposed group (10,132.0 vs 4,398.3 per 100,000 person-years). By contrast, the incidence rate of suicide for the exposed group was lower than that for the nonexposed group (738.1 vs 1,650.1 per 100,000 person-years).
In unadjusted analyses, aftercare intervention was associated with a 24% (HR =1.24, 95% CI 1.20–1.28) increase in self-harm repetition risk and a 28% (HR=0.72, 95% CI 0.66-0.77) decrease in suicide risk. After controlling for all covariates, aftercare intervention was associated with a 17% (HR =1.17, 95% CI 1.14–1.21) increase in self-harm repetition risk and a 20% (HR=0.80, 95% CI 0.74–0.86) decrease in suicide risk. The sensitivity analyses using certified suicides only (Supplementary Table 2A), using 180 days post-self-harm as the period to define a valid aftercare exposure status (Supplementary Table 2B), or using propensity score stratification (Supplementary Table 2C) all showed similar results.
No sex difference in the association with aftercare intervention was found for self-harm repetition or suicide. By contrast, differences were found between age groups and patients with and without a history of psychiatric disorders for both self-harm repetition and suicide.
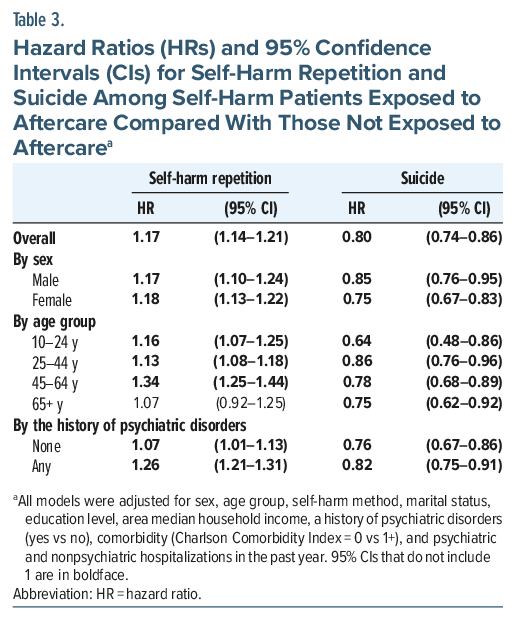
A greater increased risk of self-harm repetition associated with aftercare intervention was found in younger patients aged <65 years (HR ranged from 1.13 to 1.34) and patients with a history of psychiatric disorders (HR =1.26, 95% CI 1.21–1.31) than their counterparts (Table 3). By contrast, a more marked decrease in suicide risk associated with aftercare intervention was found in those aged 10–24 years (HR= 0.64, 95% CI 0.48–0.86) and patients without a history of psychiatric disorders (HR =0.76, 95% CI 0.67–0.86).
DISCUSSION
We found that Taiwan’s national self-harm aftercare program was associated with a 17% increase in the risk of repeat self-harm hospital presentation and a 20% decrease in suicide risk. The association of the aftercare intervention with increased self-harm repetition was more marked in patients aged <65 years (vs those aged 65+ years) and those who were diagnosed with psychiatric disorders in the previous year (vs those who were not). The association of the aftercare intervention with decreased suicide risk was most marked in the youngest patients aged 10–24 years and more marked in those without a history of psychiatric disorders (vs those with a history of psychiatric disorders).
This is the first study to investigate the association of aftercare intervention for self-harm presentations with the risk of nonfatal and fatal self-harm repetition in a national sample. This study has some limitations. First, this is an observational study using a nonexperimental design, and the causal relationships between aftercare and the risk of self-harm repetition or suicide could not be inferred directly. The exposed and nonexposed groups may not be fully comparable. Among the patients who died by suicide, 24.4% (n=809) had repeated self-harm before their death, with 52.2% of them having been exposed to aftercare. Those who had repeated self-harm before their death may have received aftercare multiple times and were associated with a higher risk of suicide. Unadjusted differences in their characteristics may confound the associations. However, our analysis already controlled for a number of important potential confounding factors such as the method of self-harm, socioeconomic variables, physical comorbidities, and a history of psychiatric disorders. Second, the aftercare intervention included a combination of risk assessment, psychological support, and referrals to external services, which prevented us from comparing the effects of specific components. Third, our sample was restricted to registered self-harm episodes presenting to hospitals; therefore, the findings may not be fully generalizable to self-harm occurring in the community, as not all episodes come to medical attention. Cases presenting to hospitals may involve attempts with greater clinical severity and higher suicidal intent, which are likely to be associated with an increased risk of subsequent nonfatal and fatal repetition. Conversely, hospital presentation may increase the likelihood of receiving a structured clinical assessment and timely referral to coordinated services, thereby reducing the risk of repetition. These opposing factors introduce uncertainty regarding the direction of bias. Nevertheless, evaluating the effectiveness of aftercare interventions among individuals who presented to hospitals remains an important focus for suicide prevention. Last, our data did not include information on the specific source (hospital unit) of self-harm reports (eg, emergency departments, outpatient clinics, or inpatient wards). However, most cases are likely to have presented to emergency departments, as Taiwan’s NSSS requires hospitals to report self-harm presentations to emergency departments but does not mandate reporting of events occurring in inpatient wards or outpatient settings.
The extant literature showed no consistent evidence for the effectiveness of brief contact interventions on self-harm repetition. Our results showed that the aftercare intervention was associated with increased risk of repeat self-harm hospital presentation, in keeping with a previous study showing higher self-harm repetition risk in those who received brief contact interventions than those who did not.12 The associations observed may be due to the increased help-seeking behaviors to hospitals following the aftercare. Self-harm patients reported that the trust established in the aftercare services can encourage their help-seeking behaviors when they are in crisis.24 Furthermore, the self-harm presentations that received aftercare may turn to use methods for self-harm with less lethality and therefore increase the likelihood of emergency department attendance. However, the findings from this study are in contrast to previous studies showing reduced self-harm repetition risk25,26 or no changes in self-harm repetition risk14,27 following the brief contact interventions. The differences in findings between the current study and previous studies may be attributable to the diverse components of the interventions and the measures of self-harm repetition. First, the components of the brief contact interventions implemented and the qualifications of the aftercare workers varied across these studies.14,25–27 Some interventions provided additional medical/counselling resources or written messages apart from telephone contacts, and most of the interventions were provided by physicians or nursing staff. Different components of the brief contact interventions and aftercare workers’ specialties may lead to different impacts on self-harm repetition risk. Second, some previous studies collected information on self-reported self-harm repetition thru telephone surveys25–27; in contrast, the current study used data for hospital presentations of self-harm repetition extracted from the NSSS, while not all self-harm episodes would present to the hospitals.
Mixed evidence was found for the effectiveness of brief contact interventions on suicide risk. Our results showed that the aftercare intervention was associated with decreased risk of suicide, consistent with the previous Taiwanese study of aftercare implemented in six pilot cities16 and the WHO’s brief contact intervention study conducted in six low- and middle-income countries.13 By contrast, other studies showed no evidence of the associations between brief contact interventions and suicide,9 which could be due to small samples and insufficient statistical power to detect the intervention effect. The reduction in suicide risk after the aftercare intervention shown in our study may be attributable to the increased likelihood of receiving treatments after seeking help at hospitals and the shift to less lethal methods for self-harm, while future research is needed to better understand the mechanisms. Furthermore, the aftercare intervention may not only be effective but also cost-effective in reducing suicide risk among the high-risk population.28
Analysis stratified by subgroups showed that the aftercare intervention was more strongly associated with an increase in the risk of repeat self-harm hospital presentation among younger patients <65 years and a decrease in the suicide risk in the youngest patients aged 15–24 years. The age differences may indicate that the younger population is more receptive to the aftercare intervention. Our results also showed that the aftercare intervention was more markedly associated with an increase in the risk of repeat self-harm hospital presentation among patients with a history of psychiatric disorders but a reduction in suicide risk among those without a history of psychiatric disorders. Patients with psychiatric disorders may have more severe and persistent problems, resulting in a continued high risk of repeated self-harm despite aftercare. Greater clinical contact may also increase detection of subsequent self-harm episodes. In contrast, patients without psychiatric disorders may be more responsive to aftercare support during acute crises. This may help reduce suicide risk by improving support and access to care.
In conclusion, Taiwan’s nationwide self-harm aftercare program was associated with reduced subsequent suicide risk but increased repeat self-harm hospital presentations, suggesting that aftercare may promote help-seeking and service engagement during crises. The findings support the potential value of systematic aftercare following self-harm, while highlighting the need for more tailored and intensive interventions for certain high-risk subgroups, eg. individuals with psychiatric disorders.
Article Information
Published Online: May 20, 2026. https://doi.org/10.4088/JCP.25m16173
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 7, 2025; accepted April 7, 2026.
To Cite: Lin CY, Chang YH, Hsu CY, et al. The effect of a nationwide aftercare program for self-harm presentations on the risk of self-harm repetition and suicide: a cohort study. J Clin Psychiatry 2026;87(3):25m16173.
Author Affiliations: Department of Public Health, College of Medicine, National Cheng Kung University, Tainan, Taiwan (Lin); Centre for Urban Transitions, Swinburne University of Technology, Melbourne, Australia (Lin); Faculty of Sport Sciences, Waseda University, Tokorozawa, Japan (Lin); Substance and Addiction Prevention Branch, Center for Healthy Communities, California Department of Public Health, Sacramento, California (Y.-H. Chang); Department of Psychiatry, School of Medicine, College of Medicine, Taipei Medical University, Taipei, Taiwan (Hsu); Psychiatric Research Center, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan (Hsu, Y.-H. Chang, S.-S. Chang); Department of Psychiatry, Wan Fang Hospital, Taipei Medical University, Taipei, Taiwan (Hsu); Taipei City Psychiatric Center, Taipei City Hospital, Taipei, Taiwan (Chen); Institute of Public Health and Department of Public Health, National Yang Ming Chiao Tung University, Taipei, Taiwan (Chen); National Center for Geriatrics and Welfare Research, National Health Research Institutes, Yunlin, Taiwan (Wu); Department of Psychiatry, National Taiwan University Hospital Yunlin Branch, Yunlin, Taiwan (Wu); Department of Psychiatry, MacKay Memorial Hospital, Taipei, Taiwan (Lee); Department of Medicine, MacKay Medical College, New Taipei City, Taiwan (Lee); Institute of Health Behaviors and Community Sciences, College of Public Health, National Taiwan University, Taipei, Taiwan (S.-S. Chang); Global Health Program, College of Public Health, National Taiwan University, Taipei, Taiwan (S.-S. Chang); Population Health Research Center, National Taiwan University, Taipei, Taiwan (S.-S. Chang).
Corresponding Author: Shu-Sen Chang, MD, MSc, PhD, Institute of Health Behaviors and Community Sciences and Global Health Program, College of Public Health, National Taiwan University, Room 623, No.17, Xu-Zhou Road, Zhongzheng Dist., Taipei City 10055, Taiwan ([email protected]).
Author Contributions: Writing – review & editing: (all authors); conceptualization: (all authors); formal analysis: (Lin); writing – original draft: (Lin, Y.-H. Chang, S.-S. Chang); data curation: (S.-S. Chang); funding acquisition: (S.-S. Chang).
Relevant Financial Relationships: The authors declare no competing interests.
Funding/Support: The study was funded by the National Science and Technology Council (NSTC), Taiwan (grant number MOST 109-2314-B-002-144-MY3), and the Ministry of Health and Welfare, Taiwan (M07B8350).
Disclaimer: The views expressed in this publication are those of the authors and not necessarily those of NSTC and the Ministry of Health and Welfare, Taiwan.
Availability of Data and Materials: The data were provided by the Ministry of Health and Welfare. The authors were not permitted to share the data.
Ethical Standards: The study was approved by the National Taiwan University Research Ethics Committee (201903HM001).
Use of AI-Assisted Technologies in the Writing Process: Artificial intelligence (AI) tools (ChatGPT, OpenAI, San Francisco, California) were used to assist with language editing and text refinement during manuscript preparation. The authors reviewed and take full responsibility for the content of the manuscript.
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- Evidence on the effectiveness of aftercare remains inconsistent, with limited large-scale, real-world data assessing both repeat self-harm and suicide outcomes.
- Aftercare following hospital presentations for self-harm may reduce suicide risk while increasing hospital-presenting self-harm, which may reflect improved help-seeking.
- In the management of self-harm, clinicians should prioritize early follow-up and sustained contact and interpret repeat presentations as opportunities for intervention rather than as indicators of treatment failure.
Editor’s Note: We encourage authors to submit papers for consideration as a part of our Focus on Suicide section. Please contact Philippe Courtet, MD, PhD, at Psychiatrist.com/contact/courtet.
References (28)

- World Health Organization. Suicide worldwide in 2019: global health estimates. World Health Organization; 2021.
- Naghavi M, Global Burden of Disease Self-Harm Collaborators. Global, regional, and national burden of suicide mortality 1990 to 2016: systematic analysis for the Global Burden of Disease Study 2016. BMJ. 2019 Feb 6;364:l94. PubMed CrossRef
- World Health Organization. Preventing suicide: a global imperative; 2014.
- Carroll R, Metcalfe C, Gunnell D. Hospital presenting self-harm and risk of fatal and non-fatal repetition: systematic review and meta-analysis. PLoS One. 2014;9(2):e89944. PubMed CrossRef
- National Institute for Health and Clinical Excellence. Self-harm: assessment, management and preventing recurrence [NICE Guideline 225]. 2022. Accessed September 14,2022. www.nice.org.uk/guidance/ng225
- World Health Organization. LIVE LIFE: An implementation guide for suicide prevention in countries. World Health Organization; 2021.
- Inagaki M, Kawashima Y, Yonemoto N, et al. Active contact and follow-up interventions to prevent repeat suicide attempts during high-risk periods among patients admitted to emergency departments for suicidal behavior: a systematic review and meta-analysis. BMC Psychiatry. 2019 Jan 25;19(1):44. PubMed CrossRef
- Doupnik SK, Rudd B, Schmutte T, et al. Association of suicide prevention interventions with subsequent suicide attempts, linkage to follow-up care, and depression symptoms for acute care settings: a systematic review and meta-analysis. JAMA Psychiatry. 2020;77(10):1021–1030. PubMed CrossRef
- Tay JL, Li Z. Brief contact interventions to reduce suicide among discharged patients with mental health disorders: a meta-analysis of RCTs. Suicide Life Threat Behav. 2022 Jul 28.
- Witt KG, Hetrick SE, Rajaram G, et al. Psychosocial interventions for self-harm in adults. Cochrane Database Syst Rev. 2021;4(4):Cd013668. PubMed CrossRef
- Simon GE, Shortreed SM, Rossom RC, et al. Effect of offering care management or online dialectical behavior therapy skills training vs usual care on self-harm among adult outpatients with suicidal ideation: a randomized clinical trial. JAMA. 2022;327(7):630–638. PubMed CrossRef
- Kapur N, Gunnell D, Hawton K, et al. Messages from Manchester: pilot randomised controlled trial following self-harm. Br J Psychiatry. 2013;203(1):73–74. PubMed CrossRef
- Fleischmann A, Bertolote JM, Wasserman D, et al. Effectiveness of brief intervention and contact for suicide attempters: a randomized controlled trial in five countries. Bull World Health Organ. 2008 Sep;86(9):703–709. PubMed CrossRef
- Bertolote JM, Fleischmann A, De Leo D, et al. Repetition of suicide attempts: data from emergency care settings in five culturally different low-and middle-income countries participating in the WHO SUPRE-MISS Study. Crisis. 2010;31(4):194–201. PubMed CrossRef
- Gunnell D, Frankel S. Prevention of suicide: aspirations and evidence. BMJ. 1994 May 7;308(6938):1227–1233. PubMed CrossRef
- Pan YJ, Chang WH, Lee MB, et al. Effectiveness of a nationwide aftercare program for suicide attempters. Psychol Med. 2013 Jul;43(7):1447–1454. PubMed CrossRef
- Hawton K, Harriss L, Hall S, et al. Deliberate self-harm in Oxford, 1990-2000: a time of change in patient characteristics. Psychol Med. 2003 Aug;33(6):987–995. PubMed CrossRef
- Chang SS. Report of suicide prevention strategies in Taoyuan City: an analysis of suicide attempt and suicide. Taipei, Taiwan: National Taiwan University; 2023.
- Chang SS. Report of suicide aftercare services and effectiveness evaluation; 2018.
- Ministry of Health and Welfare. Guideline for aftercare services; 2014.
- Chang SS, Sterne JA, Lu TH, et al. ’Hidden’ suicides amongst deaths certified as undetermined intent, accident by pesticide poisoning and accident by suffocation in Taiwan. Soc Psychiatry Psychiatr Epidemiol. 2010 Feb;45(2):143–152. PubMed CrossRef
- National Health Insurance Administration MoHaW. Unversal health coverage in Taiwan. 2019. Accessed May 17, 2022. https://www.nhi.gov.tw/English/Content_List.aspx?n=4D7051840BF42F52&topn=ED4A30E51A609E49
- Charlson ME, Pompei P, Ales KL, et al. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40(5):373–383. PubMed CrossRef
- Cully G, Leahy D, Shiely F, et al. Patients’ experiences of engagement with healthcare services following a high-risk self-harm presentation to a hospital emergency department: a mixed methods study. Arch Suicide Res. 2022 Jan–Mar;26(1):91–111. PubMed CrossRef
- Miller IW, Camargo CA Jr., Arias SA, et al. Suicide prevention in an emergency department population: the ED-SAFE Study. JAMA Psychiatry. 2017;74(6):563–570. PubMed CrossRef
- Vaiva G, Ducrocq F, Meyer P, et al. Effect of telephone contact on further suicide attempts in patients discharged from an emergency department: randomised controlled study. BMJ. 2006;332(7552):1241–1245. PubMed CrossRef
- Mousavi SG, Zohreh R, Maracy MR, et al. The efficacy of telephonic follow up in prevention of suicidal reattempt in patients with suicide attempt history. Adv Biomed Res. 2014;3:198. PubMed CrossRef
- Ross EL, Zuromski KL, Reis BY, et al. Accuracy requirements for cost-effective suicide risk prediction among primary care patients in the US. JAMA Psychiatry. 2021;78(6):642–650. PubMed CrossRef
This PDF is free for all visitors!




