Misophonia is a neurobehavioral condition with an estimated global prevalence of 6%–20%, underscoring its emerging relevance as a public health concern.1 It is characterized by intense negative emotional responses to specific auditory stimuli. Although not formally classified in the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), recent consensus criteria delineate its distinctive symptomatology, involving pronounced anger, disgust, or distress in response to particular trigger sounds.2,3 While commonly associated with repetitive human-generated sounds (eg, chewing, pen clicking), a subset of patients reports broader environmental triggers, particularly under cognitive or emotional duress.
The prevalence of misophonia symptoms ranges widely, from 33.3% reporting any auditory sensitivity to only 0.1% experiencing severe symptoms.4 Among psychiatric inpatients with depression, the prevalence ranges from 8.5% to 12.76%, with symptom severity positively correlated with anxiety, depression, and other psychiatric conditions.5
Pathophysiologically, misophonia is thought to involve hyperactivation of the anterior insular cortex and dysregulation of the salience network—mechanisms shared with anxiety and affective disorders.6,7 Despite growing recognition, misophonia remains underdiagnosed, particularly in low- and middle-income countries (LMICs), due to stigma, limited clinical awareness, and the absence of formal diagnostic frameworks. This report presents a case of atypical misophonia in a female medical student from an LMIC, complicated by comorbid generalized anxiety disorder (GAD), depression, and insomnia, with notable clinical improvement following combined pharmacologic and psychotherapeutic intervention.
Case Report
A female medical student in her mid-20s from rural South Asia presented with a 12-year history of emotional dysregulation, panic episodes, and distress triggered by ambient background sounds. Symptoms began around age 13, primarily during academic activities such as exam preparation. Specific triggers included birds chirping, background conversations, and footsteps.
Her responses comprised crying spells, intense rage, somatic symptoms (eg, headaches, palpitations), cognitive disorganization, and severe anxiety. Despite being academically gifted, she gradually withdrew from both academic and social engagements, missing multiple high-stakes medical exams due to incapacitating sound-induced anxiety and anticipatory fear of failure.
The patient’s family history was significant for epilepsy and psychiatric illness. She faced considerable psychosocial stress due to community stigma and lacked access to early psychiatric evaluation due to financial constraints.
Between 2018 and 2020, she consulted several general practitioners and was intermittently prescribed unspecified antidepressants without comprehensive psychiatric evaluation. In 2021, she was referred for psychiatric care due to worsening insomnia and academic decline.
The Patient Health Questionnaire-9 (PHQ-9), Generalized Anxiety Disorder-7 (GAD-7), and Insomnia Severity Index (ISI), which are validated screening measures for depression, anxiety, and insomnia, respectively, were administered to quantify symptom severity.9–11 The patient’s PHQ-9 score was 18, GAD-7 score was 16, and ISI score was 20.
The patient was cooperative and well groomed and displayed an anxious affect with tense posture. Her speech was coherent and goal directed. No perceptual disturbances or suicidal ideation were reported. Her thought content was notable for intrusive ruminations related to auditory stimuli; insight was fair. No signs of hearing deficits, tinnitus, or hyperacusis were observed. An audiological assessment was recommended but declined by the patient. Based on the criteria of Swedo et al,3 she was diagnosed with misophonia, comorbid GAD, persistent depressive disorder, and insomnia disorder.
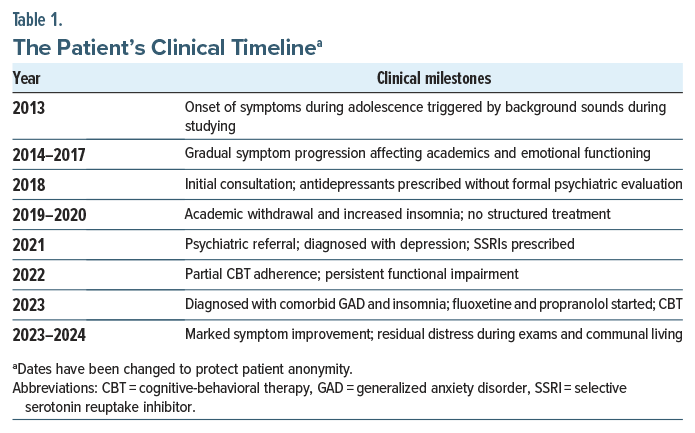
She was initiated on fluoxetine 20 mg/d and propranolol 10 mg twice/d, with occasional use of over-the-counter sleep aids. She completed 10 sessions of cognitive-behavioral therapy (CBT), which included desensitization to auditory triggers and graduated exposure, cognitive restructuring, emotion regulation and mindfulness, sleep hygiene, and academic stress management. Adjunctive strategies included white/ pink noise masking, breathing exercises, and structured academic planning. Table 1 provides the patient’s clinical timeline.
Over 7–8 months, the patient reported reduced misophonia severity, improved emotional regulation, and fewer panic episodes. She resumed group-based academic and social activities. However, distress persisted during high-pressure academic contexts, particularly examinations and hostel stays. While overall coping and functionality improved, residual hypervigilance remained. Academic outcomes showed partial recovery, although performance anxiety persisted during critical assessments.
Discussion
This patient exhibited heightened responses to ambient, nonhuman auditory stimuli during cognitively demanding tasks. These findings support emerging literature suggesting misophonia extends beyond traditional triggers and may involve attentional and salience network dysfunction.6–8
Standardized tools (PHQ-9, GAD-7, ISI) proved instrumental in symptom quantification and treatment monitoring. Their validity in LMIC populations supports their broader implementation in resource-limited psychiatric settings.12,13 Comorbidity with GAD and depression is frequently documented in misophonia cohorts.14 While previous studies have examined misophonia within affective disorders, few have emphasized the degree of academic disability encountered in this case. Unlike existing literature that broadly describes symptom clusters, this case uniquely highlights missed national-level academic opportunities due to untreated misophonia.15
There are no formal treatment guidelines for misophonia, though selective serotonin reuptake inhibitors (SSRIs) and CBT are increasingly endorsed.16 Fluoxetine likely mitigated affective instability through serotonergic modulation, while propranolol dampened autonomic hyperarousal. Existing literature supports the efficacy of SSRIs and beta-blockers in similar cases.16–18
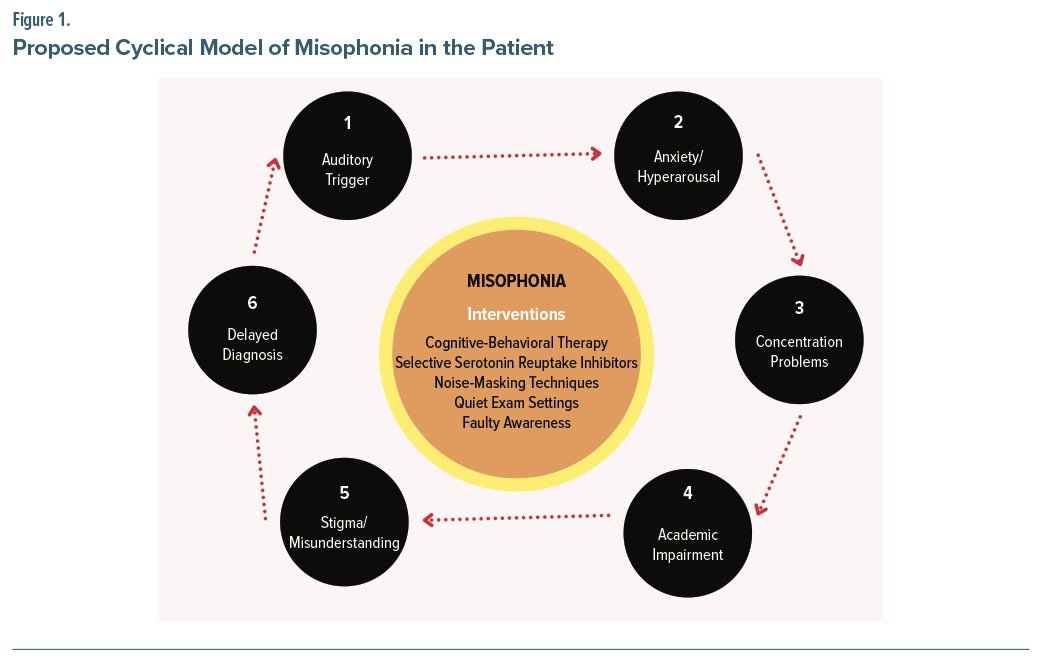
This case illustrates the adverse impact of stigma, inadequate mental health literacy among providers, and institutional limitations in LMICs. Timely diagnosis and early intervention might have prevented academic and psychosocial deterioration.19 Figure 1 illustrates a proposed cyclical model of misophonia in this case: sound-related triggers lead to anxiety and hyperarousal, followed by concentration problems and academic impairment. Stigma and misunderstanding delay proper diagnosis, perpetuating the cycle. This framework highlights key intervention points, including CBT, SSRIs, noise masking, and academic accommodations.
There is a pressing need for universally accepted diagnostic criteria, culturally adaptable screening tools, and evidence-based treatment guidelines for misophonia. Formal recognition in the DSM or International Classification of Diseases systems would improve access to care and insurance coverage. Misophonia-specific instruments (eg, Sussex Misophonia Scale)20 and international case registries could enhance early detection and cross-cultural research.
Article Information
Published Online: March 3, 2026. https://doi.org/10.4088/PCC.25cr04064
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04064
Submitted: August 20, 2025; accepted October 8, 2025.
To Cite: Asghar P. Atypical misophonia with psychiatric comorbidities in a medical student: a case from a low-resource setting. Prim Care Companion CNS Disord 2026;28(2):25cr04064.
Author Affiliations: Khyber Medical College, Peshawar, Pakistan.
Corresponding Author: Palwasha Asghar, MBBS, Khyber Medical College, Peshawar, Pakistan ([email protected]).
Relevant Financial Relationships: None.
Patient Consent: Consent was received from the patient to publish the case report, and information, including dates, has been de-identified to protect patient anonymity.
References (20)

- Pfeiffer E, Allroggen M, Sachser C. Misophonia in childhood and adolescence: a narrative review. Z fur Kinder-und Jugendpsychiatrie Psychother. 2022;51(3):222–232.
- Taylor S. Misophonia: a new mental disorder? Med hypotheses. 2017;103:109–117. PubMed CrossRef
- Paunovic KŽ, Milenković SM. The proposed criteria for high perceived misophonia in young healthy adults and the association between misophonia symptoms and noise sensitivity. Noise Health. 2022;24(113):40–48. PubMed CrossRef
- Pfeiffer E, Allroggen M, Sachser C. The prevalence of misophonia in a representative population-based survey in Germany. Soc Psychiatry Psychiatric Epidemiol. 2025;60(1):257–264. PubMed CrossRef
- Siepsiak M, Sobczak AM, Bohaterewicz B, et al. Prevalence of misophonia and correlates of its symptoms among inpatients with depression. Int J Environ Res Public Health. 2020;17(15):5464. PubMed CrossRef
- Schröder A, van Wingen G, Eijsker N, et al. Misophonia is associated with altered brain activity in the auditory cortex and salience network. Sci Rep. 2019;9(1):7542. PubMed CrossRef
- Kumar S, Tansley-Hancock O, Sedley W, et al. The brain basis for misophonia. Curr Biol. 2017;27(4):527–533. PubMed CrossRef
- Simner J, Koursarou S, Rinaldi LJ, et al. Attention, flexibility, and imagery in misophonia: does attention exacerbate everyday disliking of sound? J Clin Exp Neuropsychology. 2021;43(10):1006–1017. PubMed CrossRef
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. PubMed CrossRef
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Archives Intern Med. 2006;166(10):1092–1097. PubMed CrossRef
- Bastien CH, Vallières A, Morin CM. Validation of the Insomnia Severity Index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. PubMed CrossRef
- Steinman L, Phal O, Srou R, et al. Improving recognition of common mental health disorders in Cambodia: validation of the PHQ-9 and GAD-7 and development of a brief mental health screener. PLOS Ment Health. 2025;2(4):e0000228. PubMed CrossRef
- Sweetland AC, Belkin GS, Verdeli H. Measuring depression and anxiety in Sub-Saharan Africa. Depress anxiety. 2014;31(3):223–232. PubMedCrossRef
- Erfanian M, Kartsonaki C, Keshavarz A. Misophonia and comorbid psychiatric symptoms: a preliminary study of clinical findings. Nordic J Psychiatry. 4, 2019;73(4-5):219–228. PubMed CrossRef
- Guzick AG, Rast CE, Maddox BB, et al. “How can I get out of this?”: a qualitative study of the phenomenology and functional impact of misophonia in youth and families. Psychopathology. 2025;58(1):33–43. PubMed CrossRef
- Köroğlu S. Current trends in the treatment of misophonia. Psikiyatr Güncel Yaklaşımlar. 2024;16(2):251–257. CrossRef
- Webb J. β-Blockers for the treatment of misophonia and misokinesia. Clin Neuropharmacol. 2022;45(1):13–14. PubMed CrossRef
- Potgieter I, MacDonald C, Partridge L, et al. Misophonia: a scoping review of research. J Clin Psychol. 2019;75(7):1203–1218. PubMed CrossRef
- Mascayano F, Armijo JE, Yang LH. Addressing stigma relating to mental illness in low-and middle-income countries. Front Psychiatry. 2015;6:38. PubMed CrossRef
- Rinaldi LJ, Simner J. The Sensory Diversity Framework (SDF): A Synthesis and Predictive Model of Sensory Differences. 2025. https://sciety.org/articles/activity/10.31234/osf.io/6bycv_v1.
Enjoy this premium PDF as part of your membership benefits!