Abstract
Objective: To examine how health belief model constructs influence treatment adherence among patients with dissociative disorders and to explore how demographic variables influence the relationship.
Methods: This cross-sectional study used stratified random sampling to assess 130 patients with dissociative disorders at Allied Hospital 2, Faisalabad, Pakistan. Data were collected over a 4- month period (July 1 to October 31, 2024) via a standardized health belief model questionnaire and analyzed in SPSS v25. Health belief model constructs served as exposure variables, with treatment adherence as he outcome; correlation and regression analyses were performed.
Results: Of 130 dissociative patients, 65 were compliant and 65 were noncompliant. Perceived benefits correlated significantly with compliance (P=.003), with 61.6% of the compliant group reporting high benefits versus 38.3% of the noncompliant group. Perceived barriers were inversely related to adherence (P=.007). No significant associations were found for perceived severity (P=.104), susceptibility (P=.365), or cues to action (P=.588). The following demographic factors showed no significant correlations with adherence: age (P=.366), sex (P=.415), marital status (P=.514), education (P=.197), occupational status (P=.571), employment type (P=.437), and time since diagnosis (P=.189).
Conclusion: The results showed that perceived benefits and barriers within the health belief model had considerable effects on treatment adherence among people with dissociative disorders. Demographic characteristics and other health belief model components did not significantly correlate with compliance. Targeted interventions to strengthen perceived benefits and reduce perceived barriers could enhance adherence in this population.
Prim Care Companion CNS Disord 2026;28(2):25m04085
Author affiliations are listed at the end of this article.
Mental health disorders are among the major causes of disability globally, as well as a strong risk factor for suicide and all-cause mortality, ranked among the top 10 causes of global burden.1 Dissociative disorders are a prevalent mental health issue that often goes unnoticed, and they have been excluded from extensive epidemiological studies for many years.2 Patients with dissociative disorders have clinically substantial impairment.3
Dissociation is defined in terms of fragmentation and splitting of the mind and alterations in perception of the self and body. Clinical manifestations include altered perceptions and behavior such as derealization; depersonalization; distortions of perception of time, space, and body; and conversion hysteria.4 Dissociative illnesses are far more common than one might anticipate based on the diagnoses given at the time of hospital discharge.5 According to a study conducted in North America, dissociative disorders were highly prevalent with a rate of 29% among psychiatric outpatients.6 Another study involving psychiatric outpatients in Turkey reported that the incidence of dissociative disorders was 12%.7
Patients with dissociative disorders have complicated clinical presentations with numerous comorbidities,8 which can complicate treatment adherence. Comorbidities include personality disorders, somatic disorders, eating and food disorders, anxiety, depression, and conversion disorders.9 Patients with dissociative disorders pose management challenges, even for highly skilled practitioners.10 Treatment of dissociative disorders is linked to reduced symptoms and suicidality.11
Adherence to treatment, especially in psychiatric illnesses, is a widespread concern.12 Adherence to the regimen ensures treatment effectiveness, which also discourages relapses and prevents functional degradation.13 Patients with mental disorders adhere to their treatment less frequently than nonpsychiatric patients. Physicians frequently overestimate how well patients comply to their treatment plans. However, general psychiatry patients often have a mistrust toward medication.14 Despite positive response to early therapy, nonadherence for mental disorders ranges from 25% to 50%, which lowers recovery rates.1 Treatment noncompliance is closely linked to the belief that there are obstacles preventing someone from pursuing treatment.15 A study on the treatment of hypertensive patients found that perceived barriers were significant predictors of nonadherence to therapy.16
The health belief model is a psychosocial formulation developed to explain health-related behavior at the level of individual decision-making17 that was introduced in the 1950s and 1960s.18 During the 1950s, the cognitive theory of value expectancy was reformulated in relation to health-related activities, including an individual’s assessment of personal susceptibility and perceived severity of sickness, and their chances of being able to lessen the threat by personal action.19 The components of the health belief model include perceived susceptibility, perceived severity, perceived benefits, perceived barriers, and cues to action.20 These components facilitate comprehension of the elements that influence people to engage in health-related behavior or prevent them from seeking medical intervention.21
Various studies have assessed the relationship between the health belief model and treatment adherence in different medical and psychiatric conditions, such as diabetes22 and hypertension,23 and among outpatients receiving antipsychotic medications.24 However, no studies, to our knowledge, have applied the health belief model to dissociative disorders.
Treatment adherence and quality of life are related, and mental health services should take adherence into account to closely monitor noncompliant patients.25 Therefore, by identifying the key factors that influence adherence in dissociative patients, this research may help guide interventions for improved treatment outcomes. A better understanding of these dynamics could help clinicians design targeted strategies to promote adherence, in turn leading to better recovery and quality of life.
The primary objective of this study was to investigate how health belief model constructs influence treatment adherence among patients with dissociative disorders. The secondary objective was to explore how demographic variables influence the relationship between health belief model constructs and treatment adherence.
METHODS
Study Design
This cross-sectional study examined the association between the constructs of the health belief model and treatment adherence among patients with dissociative disorders. A validated health belief model questionnaire was administered via structured interview to a stratified random sample of outpatients and inpatients. Data analysis employed correlation and stepwise logistic regression to identify predictors of adherence. Ethical approval was obtained from the Ethical Review Committee of Faisalabad Medical University/Faculty of Psychiatry, Allied Hospital 2, Faisalabad, Pakistan (reference #48.ERC/FMU/2023-24/466). All participants provided informed oral consent. The principles of confidentiality were strictly maintained.
Setting and Sample
The study was conducted at Allied Hospital 2, Faisalabad, a large public-sector teaching hospital providing specialized psychiatric services to a diverse urban and rural population in the Faisalabad division. Data collection occurred over a 4-month period (July 1 to October 31, 2024) within both the psychiatric outpatient department (OPD) and the inpatient psychiatric ward.
Participants were recruited using a stratified random sampling method. Stratification was performed at the point of sample collection based on the clinical setting (OPD vs ward) to ensure proportional representation. All eligible patients presenting during the study period were listed within each stratum, and a random selection was made. Inclusion criteria were confirmed clinical diagnosis of a dissociative disorder, either attending the psychiatric OPD for follow-up or admitted to the psychiatric ward, and ability to understand the study purpose and provide informed consent. Exclusion criteria were a comorbid primary psychiatric diagnosis other than a dissociative disorder, severe cognitive impairment, language barriers precluding reliable interviewing, and unwillingness or inability to provide informed consent.
The sample size of 130 participants was determined through power estimation based on findings from previously published studies that examined health belief constructs and adherence in psychiatric populations. The sample was considered adequate to detect statistically significant associations between health belief model constructs and treatment adherence with acceptable power.
Variables
The primary exposure variables were the 5 health belief model constructs operationalized as continuous scores: perceived severity, perceived susceptibility, perceived benefits, perceived barriers, and cues to action. The primary outcome variable was treatment adherence as measured via the structured questionnaire. Potential confounders were age, sex, socioeconomic status, education level, and duration of illness. Clinical setting (OPD/inpatient) was also considered as a stratification variable.
Instruments and Data Collection
Data were collected using a standardized and validated health belief model questionnaire along with direct structured interviews. The health belief model questionnaire was adapted from previously validated instruments used in adherence and behavioral studies. The questionnaire was based on the study by Boulos and Hassan.26 We supplemented the original items with additional questions relevant to our study objectives and setting, including modifications to the treatment adherence and health belief model components. Responses were recorded on a Likert scale and for primary analysis were treated as continuous variables. Where necessary, responses were later categorized into high and low groups based on distribution and existing literature.
All interviews were conducted by trained interviewers to minimize interviewer bias and ensure uniformity. Interviews took place during either routine OPD follow-up visits or inpatient admission, depending on patient availability and clinical condition. No medical records were abstracted for the purpose of this study, and all data were obtained directly from participants through interviews and questionnaires.
Data Analysis
Data were entered and analyzed using SPSS version 25. Descriptive statistics including frequencies, percentages, means, and SDs were used to summarize patient demographics and key study variables. Missing data were minimal (less than 5%) and were handled using listwise deletion.
Initially, correlation and simple regression analyses were performed to examine the linear relationships between individual health belief model constructs and treatment adherence. For multivariate analysis, stepwise logistic regression was applied to identify independent predictors of adherence while controlling for potential confounding variables such as age, sex, socioeconomic status, and duration of illness. Results of the final regression model are expressed as odds ratios with corresponding CIs. To enhance interpretability for certain analyses, selected continuous variables were categorized (eg, high vs low adherence) based on statistical distribution and previously published literature.
RESULTS
The study revealed that while participants were predominantly young, female, single, educated, and unemployed, none of these sociodemographic variables demonstrated a significant association with treatment compliance. In contrast, treatment-related factors showed robust and statistically significant relationships with adherence: participants currently engaged in therapy and those taking medication were markedly more likely to exhibit high compliance (P < .001 for both). Analysis within the health belief model framework further indicated that perceived benefit was a strong positive predictor of treatment adherence, whereas perceived barriers were significantly and negatively associated with compliance, highlighting the crucial role of individuals’ beliefs about treatment efficacy and obstacles in shaping adherence behaviors. Perceived severity, perceived susceptibility, and cues to action did not demonstrate direct associations with compliance, though several significant correlations were observed among the health belief model constructs. Multiple regression analysis reinforced these findings, identifying perceived benefit as an independent positive predictor and perceived barriers as a significant negative predictor of treatment compliance. Overall, the results emphasize that psychological and treatment-engagement factors, rather than demographic characteristics, are central determinants of adherence among individuals with dissociative disorders.
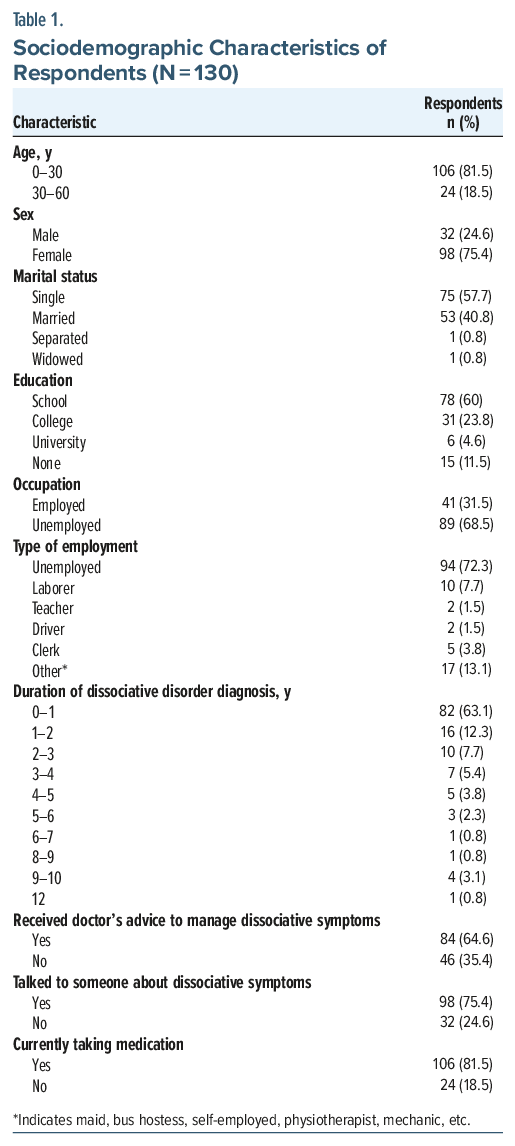
A total of 130 individuals diagnosed with dissociative disorders participated in the study. Most participants were aged 0–30 years (n=106, 81.5%), and there were more females (n=98, 75.4%) than males (n=32, 24.6%). Most respondents were single (n=75, 57.7%), while 53 (40.8%) were married. Regarding education, 78 (60%) had completed school, 31 (23.8%) had attended college, 6 (4.6%) had a university degree, and 15 (11.5%) had no formal education. Employment status showed that 89 (68.5%) were unemployed, while 41 (31.5%) were employed in various roles including laborers (n=10, 7.7%), clerks (n=5, 3.8%), teachers (n=2, 1.5%), and drivers (n=2, 1.5%). A small portion (n=17, 13.1%) reported other occupations such as maid, bus hostess, and self-employed. The majority of respondents (n=82, 63.1%) had been diagnosed with dissociative disorders within the past year, and 83 (63.8%) were currently receiving therapy. Additionally, 106 (81.5%) reported taking medication, while 24 (18.5%) were not. A substantial proportion (n=84, 64.6%) had received medical advice for managing their dissociative symptoms, and 98 (75.4%) had talked to someone about these symptoms (Table 1).
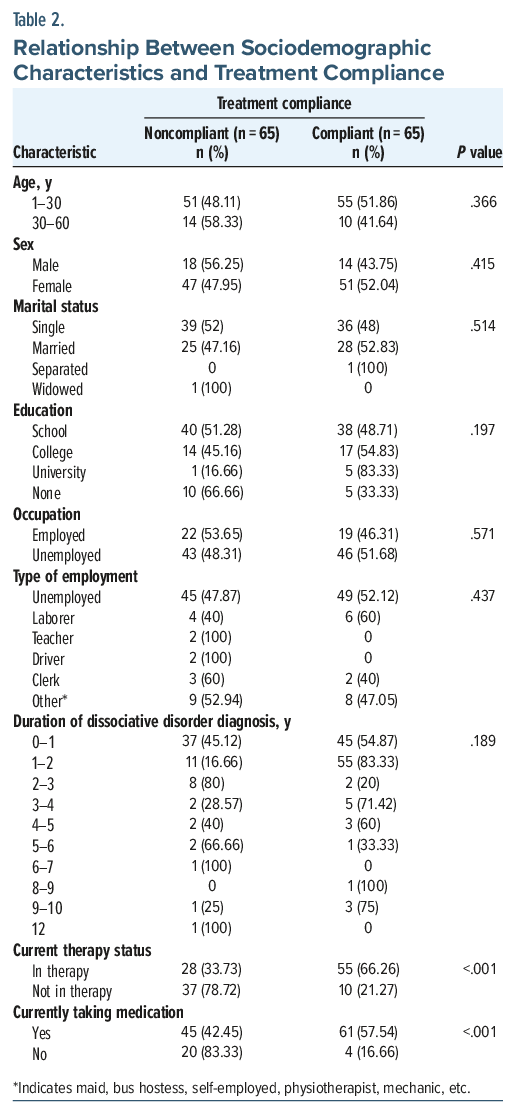
Current therapy status and current medication status were significantly associated with treatment adherence. Individuals currently in therapy were significantly more likely to fall in the “high adherence” group (55 of 83, 66.26%, P < .001), and those on medication also demonstrated higher adherence (61 of 106, 57.54%, P < .001). These findings suggest that active engagement in treatment has a strong, positive association with adherence levels.
There was no statistically significant association found between treatment compliance (measured via χ2) and variables such as age, sex, marital status, education, occupation, type of employment, and duration of diagnosis. For age, the χ2 test yielded a P value of .366, indicating no relationship between age and compliance. Similarly, sex (P=.415), marital status (P=.514), education level (P=.197), and occupational status (P=.571) also showed nonsignificant relationships. Type of employment (P=.437) and duration of diagnosis (P =.189) also did not significantly predict treatment adherence (Table 2).
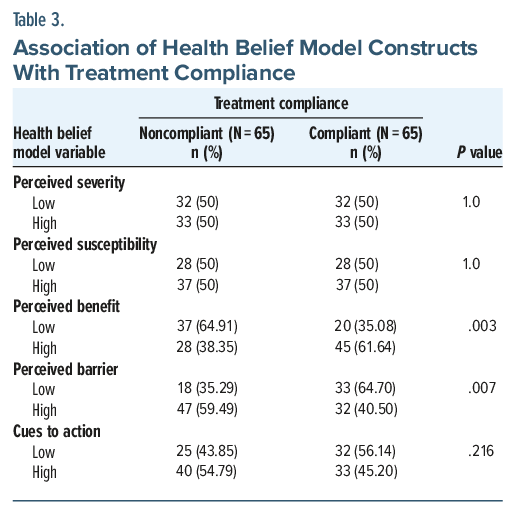
The study compared 65 treatment-compliant and 65 treatment-noncompliant participants. Perceived severity and perceived susceptibility showed no significant association with treatment compliance, as both compliant and noncompliant groups had equal distributions of responses (P=1.0 for both). However, perceived benefit was significantly associated with compliance (P=.003), with 45 (61.64%) participants in the compliant group reporting high perceived benefits compared to only 28 (38.35%) in the noncompliant group. Conversely, perceived barriers showed a significant inverse relationship with treatment compliance (P=.007), where 47 (59.49%) individuals in the noncompliant group reported high perceived barriers compared to only 32 (40.50%) in the compliant group. Although more compliant individuals reported high cues to action (n=33, 45.2%) than those with low cues (n=32, 56.14%), the association was not statistically significant (P=.216).
The negative association between perceived barriers and adherence (β=–1.633, P =.015) mirrors the broader psychiatric literature. Guo et al,27 in a meta-analysis of schizophrenia patients, found that nonadherence is driven by both illness-related factors (poor insight, severe symptoms, side effects) and psychosocial barriers (low support, stigma, financial strain).
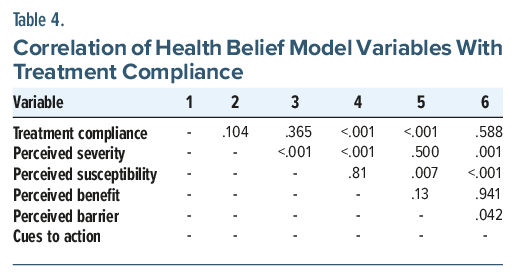
The results of the correlation analysis among the study variables are presented in Table 3. Treatment compliance was significantly correlated with perceived susceptibility (P = .365), perceived severity (P = .104), perceived benefit (P < .001), perceived barrier (P < .001), and cues to action (P = .588), though the strength and direction of these correlations vary.
Perceived severity showed significant correlations with perceived susceptibility (P < .001), perceived benefit (P < .001), and cues to action (P=.001). Perceived susceptibility was significantly correlated with perceived barrier (P=.007) and cues to action (P < .001). Furthermore, perceived benefit was not significantly associated with perceived barrier (P=.13) but showed no significant correlation with cues to action (P=.941). Finally, a significant correlation was observed between perceived barrier and cues to action (P =.042). These findings suggest multiple significant interrelations among health belief model constructs, with implications for understanding treatment compliance behavior (Table 4).
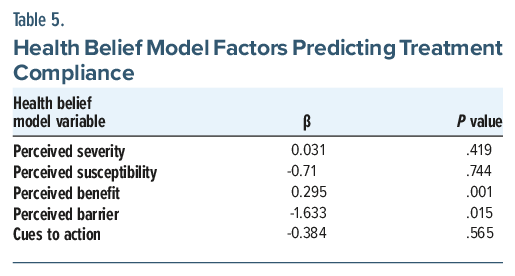
A multiple linear regression analysis was conducted to examine the influence of health belief model constructs on treatment compliance. The results indicated that perceived benefit (β=0.295, P =.001) is a significant predictor of treatment compliance. These findings highlight the importance of perceived benefits in influencing treatment adherence behavior. A negative β indicates a negative association between perceived susceptibility, perceived barrier, cues to action, and treatment compliance (Table 5).
Clinically, these results offer valuable insights into improving treatment outcomes. The strong impact of perceived benefits and barriers suggests that clinicians should systematically assess and address patients’ beliefs about treatment, including concerns related to stigma, cost, side effects, and the perceived usefulness of therapy and medication. Enhancing perceived benefits through targeted psychoeducation, motivational interviewing, and therapeutic alliance building may improve adherence. Similarly, reducing perceived barriers through practical support, problem-solving interventions, and continuity of care can strengthen treatment engagement. Given the strong association between active treatment involvement and adherence, clinicians should prioritize early connection to therapeutic services and consistent follow-up. Incorporating these findings into clinical practice can help create individualized, belief-informed care plans that enhance adherence and improve outcomes for individuals with dissociative disorders.
DISCUSSION
This study found that among individuals with dissociative disorders, perceived benefits and perceived barriers were the only health belief model constructs significantly associated with treatment adherence. Patients who believed that treatment would meaningfully improve their symptoms were substantially more likely to be adherent, while those perceiving greater barriers such as financial difficulties, limited access to specialized care, or psychosocial obstacles were markedly less likely to follow treatment. Other health belief model domains, including perceived severity, susceptibility, and cues to action, showed no significant association with adherence. Likewise, demographic characteristics such as age, sex, marital status, education, and employment status did not predict adherence. Engagement in current therapy and medication use, however, were strongly related to higher adherence, reflecting the reinforcing effect of ongoing care involvement.
While Adams and Scott28 emphasized perceived severity (eg, fear of relapse or hospitalization) as a key predictor, our study reported no significant association between compliance and perceived severity/ susceptibility (P =1.0). The absence of significance in our sample may reflect unique features of dissociative disorder symptomatology. Patients with dissociative disorders often exhibit impaired insight (eg, amnesia, identity fragmentation), potentially diminishing their perception of illness severity. This interpretation is aligned with that of Nester et al,29 who reported that individuals with dissociative symptoms frequently encounter misdiagnosis, lack of provider understanding, and limited access to specialized care, all of which can reduce engagement in treatment regardless of perceived severity.
Parallel to Nester and colleagues’ findings,29 our research highlights the importance of empathetic and compatible care for individuals with dissociative disorders. Although most participants in both studies were already receiving treatment (64% in our sample; 91% in Nester et al29), many continued to face barriers such as cost and lack of specialized providers. Our health belief model analysis confirms the clinical observation that patients’ belief in treatment efficacy (β = 0.295) and quality of therapeutic relationships outweigh demographic variables in predicting adherence.
Additionally, Bąk-Sosnowska et al30 demonstrated that psychological constructs such as health locus of control, coping styles, and mindfulness significantly influence treatment adherence in chronic conditions. Our findings support this finding, indicating that internal beliefs and coping mechanisms play a greater role in adherence than sociodemographic characteristics.
Abdisa et al31 reported that internalized stigma significantly reduced adherence among patients with mental illness, with higher stigma scores associated with lower medication use. While stigma was not directly measured in our study, the negative effect of perceived barriers may, in part, represent the impact of stigma on willingness to engage in treatment.
This study has several strengths. It is one of the first, to our knowledge, to apply the health belief model to dissociative disorders, contributing novel insights into an under-researched psychiatric group. The use of a standardized health belief model questionnaire and a stratified random sampling, as well as inclusion of both outpatient and inpatient populations, enhances the internal validity and representativeness of findings. Additionally, the equal distribution of compliant and noncompliant participants allowed balanced comparisons.
However, important limitations should be considered. The cross-sectional design restricts causal inference, and self-reported adherence may be influenced by recall bias or fluctuating insight, which is particularly relevant in dissociative disorders. The study did not assess culturally specific barriers such as stigma, family beliefs, or reliance on alternative healing practices, which may have interacted with health belief model constructs. Furthermore, the absence of qualitative data limits deeper understanding of personal narratives underlying perceived benefits and barriers. Finally, the study’s single-center setting may limit generalizability to broader populations.
In clinical practice, these findings highlight the value of strengthening patients’ belief in the benefits of treatment while actively identifying and reducing perceived barriers. Psychoeducation tailored to dissociative presentations, improved access to specialized care, reduction of logistical obstacles, and culturally sensitive communication may enhance adherence. Interventions that foster therapeutic alliance and regularly revisit patient beliefs may be particularly effective. Future research should investigate these constructs longitudinally, incorporate qualitative exploration, and examine cultural and systemic influences to create more targeted adherence-enhancing strategies.
CONCLUSION
Our findings reinforce and expand upon existing literature by demonstrating that perceived benefits and barriers are the most critical health belief model constructs influencing treatment adherence in dissociative disorders. Interventions that enhance treatment expectations, address perceived obstacles, and provide empathetic care may substantially improve adherence and outcomes in this underserved population.
Article Information
Published Online: March 24, 2026. https://doi.org/10.4088/PCC.25m04085
© 2026 Physicians Postgraduate Press, Inc.
Submitted: September 15, 2025; accepted December 18, 2025.
To Cite: Baig S, Sajjad H, Mehmood T, et al. Health belief model and treatment adherence in patients with dissociative disorders: a cross-sectional study. Prim Care Companion CNS Disord 2026;28(2):25m04085.
Author Affiliations: Allied Hospital Faisalabad, Pakistan (Baig, Sajjad, Mehmood, Anwar); Dr.Faisal Masood Teaching Hospital Sargodha, Pakistan (Eman); Texas Tech University Health Sciences Center (Sarangi).
Corresponding Author: Sajal Baig, MBBS, Allied Hospital Faisalabad, Pakistan ([email protected]).
Acknowledgements: Abstract presented at Association of Physicians of Pakistani Descent of North America 48th Annual Meeting Young Physicians Research Session; July 12, 2025; Dallas, Texas.
Financial Disclosure: None.
Funding/Support: None.
Clinical Points
- In patients with dissociative disorders, perceived benefits and barriers are the best indicators of treatment adherence; during sessions, therapists should purposefully emphasize treatment benefits.
- Adherence in dissociative patients may be greatly increased by addressing modifiable barriers, such as limited insight, stigma, logistical challenges, and inconsistent follow-up.
- When planning adherence-focused therapies, physicians should prioritize evaluating individual health beliefs rather than relying on patient characteristics because demographic factors do not consistently predict adherence.
References (31)

- Medication Adherence in Psychiatric Disorders: a Multidimensional Exploration of Patient, Treatment, and Environmental/Social Factors | Frontiers Research Topic. https://www.frontiersin.org/research-topics/61626/medication-adherence-in-psychiatric-disorders-a-multidimensional-exploration-of-patient-treatment-and-environmentalsocial-factors.
- Sar V. Epidemiology of dissociative disorders: an overview. Epidemiol Res Int. 2011;2011(1):404538.
- Johnson JG, Cohen P, Kasen S, et al. Dissociative disorders among adults in the community, impaired functioning, and axis I and II comorbidity. J Psychiatric Res. 2006;40(2):131–140. PubMed CrossRef
- Scaer RC. The neurophysiology of dissociation and chronic disease. Appl Psychophysiol Biofeedback. 2001;26(1):73–91. PubMed CrossRef
- Lipsanen T, Korkeila J, Peltola P, et al. Dissociative disorders among psychiatric patients. Eur Psychiatry. 2004;19(1):53–55. PubMed CrossRef
- Foote B, Smolin Y, Kaplan M, et al. Prevalence of dissociative disorders in psychiatric outpatients. AJP. 2006;163(4):623–629. PubMed CrossRef
- Sar V, Tutkun H, Alyanak B, et al. Frequency of dissociative disorders among psychiatric outpatients in Turkey. Compr Psychiatry. 2000;41(3):216–222. PubMed CrossRef
- Bozkurt H, Duzman Mutluer T, Kose C, et al. High psychiatric comorbidity in adolescents with dissociative disorders. Psychiatry Clin Neurosci. 2015;69(6):369–374. PubMed CrossRef
- 6.3: Dissociative Disorders - Comorbidity. Social Sci LibreTexts. https://socialsci.libretexts.org/Bookshelves/Psychology/Psychological_Disorders/Fundamentals_of_Psychological_Disorders_3e_(Bridley_and_Daffin)/02%3A_Part_II._Mental_Disorders__Block_1/06%3A_Dissociative_Disorders/6.03%3A_Dissociative_Disorders_-_Comorbidity. 2022.
- Turkus JA, Kahler JA. Therapeutic interventions in the treatment of dissociative disorders. Psychiatr Clin. 2006;29(1):245–262. PubMed CrossRef
- Brand BL, Classen CC, McNary SW, et al. A review of dissociative disorders treatment studies. J Nerv Ment Dis. 2009;197(9):646–654. PubMed CrossRef
- Willis E. Applying the health belief model to medication adherence: the role of online health communities and peer reviews. J Health Commun. 2018;23(8):743–750. PubMed CrossRef
- Sajatovic M, Velligan DI, Weiden PJ, et al. Measurement of psychiatric treatment adherence. J Psychosomatic Res. 2010;69(6):591–599. PubMed CrossRef
- Pogany L, Lazary J. Health control beliefs and attitude toward treatment in psychiatric and non-psychiatric clinical samples. Front Psychiatry. 2021;12:537309. PubMed CrossRef
- Suhat S, Suwandono A, Adi MS, et al. Relationship of health belief model with medication adherence and risk factor prevention in hypertension patients in Cimahi city, Indonesia. Evid Based Care. 2022;12(2):51–56.
- Obirikorang Y, Obirikorang C, Acheampong E, et al. Predictors of noncompliance to antihypertensive therapy among hypertensive patients Ghana: application of health belief model. Int J Hypertens. 2018;2018(1):4701097. PubMed CrossRef
- Mikhail B. The health belief model: a review and critical evaluation of the model, research, and practice. Adv Nurs Sci. 1981;4(1):65–82. PubMed CrossRef
- Becker MH, Maiman LA, Kirscht JP, et al. The health belief model and prediction of dietary compliance: a field experiment. J Health Soc Behav. 1977;18(4):348–366. PubMed CrossRef
- Glanz K, Rimer BK, Viswanath K. Heath Behavior and Health Education: Theory, Research, and Practice. 4th ed. San Francisco, CA: Jossey-Bass; 2008.
- Rosenstock IM. Health belief model. Encycl Psychol. 2000;4:78–80.
- Henshaw EJ, Freedman-Doan CR. Conceptualizing mental health care utilization using the health belief model. Clin Psychol Sci Pract. 2009;16(4):420–439. CrossRef
- Warren L, Hixenbaugh P. Adherence and Diabetes. In: Myers L, Midence K. Adherence to Treatment in Medical Conditions. CRC Press; 1998.
- Kamran A, Ahari SS, Biria M, et al. Determinants of patient’s adherence to hypertension medications: application of health belief model among rural patients. Ann Med Health Sci Res. 2014;4(6):922–927. PubMed
- Kelly GR, Mamon JA, Scott JE. Utility of the health belief model in examining medication compliance among psychiatric outpatients. Soc Sci Med. 1987;25(11):1205–1211. PubMed CrossRef
- Caqueo-Urízar A, Urzúa A, Mena-Chamorro P, et al. Adherence to antipsychotic medication and quality of life in Latin-American patients diagnosed with schizophrenia. PPA. 2020;14:1595–1604. PubMed CrossRef
- Boulos DNK, Hassan AM. Using the Health Belief Model to assess COVID-19 perceptions and behaviours among a group of Egyptian adults: a cross-sectional study. BMC Public Health. 2023;23(1):1624. PubMed CrossRef
- Guo J, Lv X, Liu Y, et al. Influencing factors of medication adherence in schizophrenic patients: a meta-analysis. Schizophr (Heidelb). 2023;9(1):31. PubMed CrossRef
- Adams J, Scott J. Predicting medication adherence in severe mental disorders. Acta Psychiatr Scand. 2000;101(2):119–124. PubMed CrossRef
- Nester MS, Hawkins SL, Brand BL. Barriers to accessing and continuing mental health treatment among individuals with dissociative symptoms. Eur J Psychotraumatol. 2022;13(1):2031594. PubMed CrossRef
- Bąk-Sosnowska M, Gruszczyńska M, Wyszomirska J, et al. The influence of selected psychological factors on medication adherence in patients with chronic diseases. Healthc (Basel). 2022;10(3):426. PubMed CrossRef
- Abdisa E, Fekadu G, Girma S, et al. Self-stigma and medication adherence among patients with mental illness treated at Jimma University Medical Center, Southwest Ethiopia. Int J Ment Health Syst. 2020;14:56. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!