Background
Measurement-based care (MBC) uses routinely administered standardized symptom assessments to characterize clinical status and inform treatment decisions.1–3 MBC is thought to improve outcomes partly by encouraging treatment changes when symptoms remain elevated.2 Newer symptom measures for bipolar disorder are gaining traction4; however, the relationship between measure scores and treatment changes remains unclear. We used data from a pilot randomized trial to examine this relationship and characterize types of treatment changes occurring with MBC for bipolar disorder.
Methods
We conducted a secondary analysis of data from a pilot randomized controlled trial comparing MBC for bipolar disorder to enhanced usual care. MBC involved administering the Patient Health Questionnaire-9 (PHQ-9)5 to assess depressive symptoms and the Patient Mania Questionnaire-9 (PMQ-9)6 to assess manic symptoms for each visit. Usual care involved administration of the PHQ-9 only, as participating clinics were already using this measure. The PHQ-9 and PMQ-9 are each scored from 0 to 27 points, with a higher score indicating greater severity of symptoms. For both symptom measures, a score of 10 or higher was considered “elevated” in severity.5–7
The trial was conducted at 5 primary care clinics offering integrated behavioral health services. Participating clinicians were psychiatrists or psychiatric advanced practice nurses. Patient inclusion criteria were age ≥18 years and clinician diagnosis of bipolar disorder. Exclusion criteria were inability to provide informed consent or plans to discontinue care. Study procedures were approved by the University of Washington Human Subjects Division.
Thirty patients were randomized to 6 months of treatment with MBC (n = 15) or usual care (n = 15). Patients were asked to complete the designated measures at or up to 72 hours prior to scheduled appointments. Clinicians were recommended to review results, compare them to previous scores, and discuss them with patients.
One psychiatrist reviewed patients’ medical records to extract treatment changes and medications (Supplement 1). Treatment change categories included initiation of, adjustments to, or discontinuation of medications used to treat bipolar disorder, and initiation of, change in frequency of, or intensification of psychosocial interventions. Frequencies of symptoms and treatment changes were reported at treatment change, patient, and visit levels. Given the small sample size, we were underpowered for inferential statistics and therefore reported descriptive statistics and effect sizes with 95% CIs. Data management and statistical analysis were conducted with Python (version 3.10) in Google Colaboratory.8
Results
Visits and Demographics. Over the 6-month study period, 71 visits were completed by 30 patients (mean=2.37; median=2; interquartile range=2; range=1–8). All patients had ≤4 visits, except for 1 outlier. Eleven patients had only 1 visit during the study. The mean age was 39.7 years (SD=12.8). Most patients identified as non-Hispanic, white, and female. Supplement 2 contains additional information about patient characteristics and baseline medications.
Symptom Measure Scores. Over two-thirds of visits where symptom measures were completed (67.6%) had a PHQ-9 score ≥10, including 17 of 29 MBC visits (58.6%) and 29 of 39 usual care visits (74.4%). Additionally, 22 of 29 patients who completed symptom measures (75.9%) had a PHQ-9 score ≥10 at 1 or more visits, comprising 11 patients receiving MBC and 11 patients receiving usual care. PHQ-9 scores ranged from 1 to 25, and PMQ-9 scores ranged from 2 to 13.
Approximately one-third of MBC visits where symptom measures were completed had a PMQ-9 score ≥10 (10 of 29 visits, 34.5%). Eight of 15 MBC-group patients (53.3%) reported a PMQ-9 score ≥10 at least once. Seven of these 8 patients (87.5%) had concurrently elevated PHQ-9 scores at the same visit, encompassing 8 of the 10 visits with elevated PMQ-9 scores (80.0%).
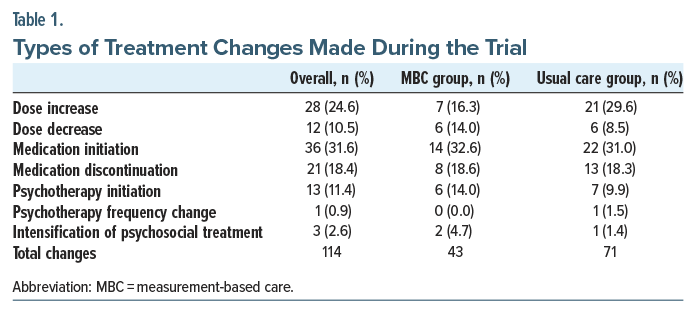
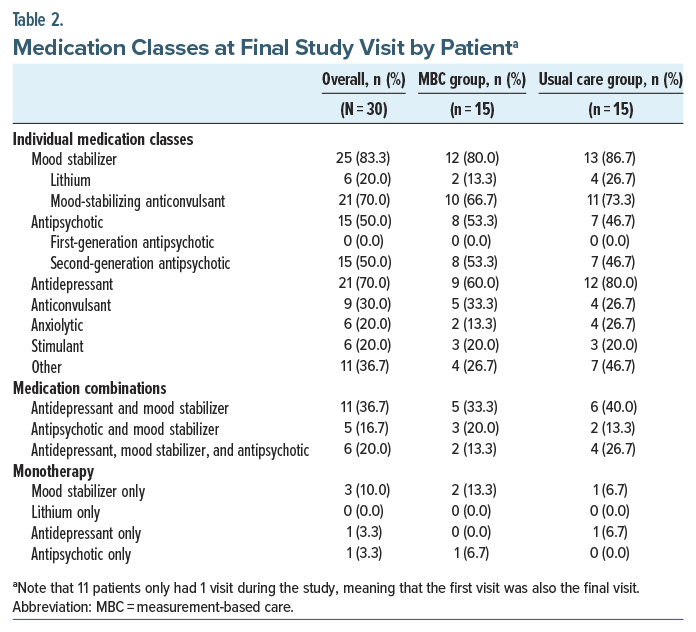
Treatment Changes and Medications. Treatment changes occurred at 37 of 48 visits with an elevated symptom measure (77.1%) and 12 of 20 visits without elevated symptoms (60.0%), with an odds ratio of 2.242 (95% CI, 0.732–6.869). Altogether, 114 changes (97 medication changes and 17 psychosocial changes) were made, involving 51 study visits and 25 patients. Medication initiations were most common overall (31.6%), followed by dose increases (24.6%), medication discontinuations (18.4%), psychotherapy initiations (11.4%), dose decreases (10.5%), psychosocial intervention intensifications (2.6%), and psychotherapy frequency changes (0.9%). These distributions were similar at the study group level, except that dose increases (16.3%) and dose decreases (14.0%) were equally common in the MBC group (Table 1). Moreover, similar percentages of patients in each group were prescribed treatment with mood stabilizers (80% in the MBC group, 86.7% in the usual care group), antipsychotics (53.3%, 46.7%), and antidepressants (60.0%, 80.0%) at the study’s conclusion (Table 2); see Supplement 3 for a visit-level breakdown of treatment changes.
Discussion
We explored treatment changes occurring with MBC for bipolar disorder and found that treatment changes were more common at visits with elevated symptom measures. Distributions of treatment change categories and medication classes prescribed were similar across groups, for which there are 2 possible explanations. First, elevated depressive symptoms were more prevalent than elevated manic symptoms, and most patients with the latter had concurrently elevated depressive symptoms, consistent with the phenomenology of bipolar disorder symptoms.9 Second, treatment changes in the usual care group (with depressive symptom monitoring) were already very common. As such, there were relatively few opportunities for manic symptom monitoring to identify additional visits with indications for change.
Treatment changes occurred frequently and consisted mainly of medication changes; a nonprimary care setting offering additional psychotherapy services may have resulted in more psychosocial interventions. Medication changes occurred at over two-thirds of visits, consistent with a 1995–2005 bipolar disorder clinical trial that recorded medication changes at 69% of outpatient visits.10
Although treatment changes occurred at the majority of visits with elevated symptom scores, the lack of treatment changes at certain visits with elevated symptom scores may be attributable to several factors. One possibility is that symptom severity at a visit, while elevated, may have been an improvement compared to prior visits (change in symptom scores over time was not accounted for in this analysis). Alternatively, clinicians and/or patients may have opted to monitor elevated symptoms for longer before deciding to make a change. Elevated symptom scores could also be due to a variety of factors, including normal response to stressors, and thus may not always indicate a need for treatment change.
Study strengths include usage of multiple units of analysis (patients, visits, treatment changes) and assessment of a range of treatment changes. Limitations include small sample size and minimal demographic diversity. One-third of patients only had 1 visit, limiting opportunities for change. Treatment change rationales were incompletely assessed, so we could not ascertain why a change did or did not occur. Finally, all patients completed the PHQ-9, precluding comparison to a group without MBC.
Conclusion and Future Directions
Among patients receiving MBC for bipolar disorder in primary care, treatment changes were more common in the presence of elevated symptoms. Similar types of treatment changes occurred in both groups.
Having established the feasibility of MBC involving the PMQ-9 and PHQ-9 for monitoring treatment of patients with bipolar disorder in primary care settings, the next steps would be to conduct a fully powered trial to assess the effectiveness of MBC. A larger or longer trial might also enroll individuals with a wider range of manic symptoms. Follow-up studies could also assess, through interviews, how clinicians incorporated symptom measure results into the clinical decision-making process.
Article Information
Published Online: February 24, 2026. https://doi.org/10.4088/PCC.25br04095
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(1):25br04095
Submitted: September 3, 2025; accepted November 25, 2025.
To Cite: Xue I, Blanchard BE, Park JH, et al. Measurement-based care for bipolar disorder: symptoms and treatment changes. Prim Care Companion CNS Disord 2026;28(1):25br04095.
Author Affiliations: University of Cincinnati College of Medicine, Cincinnati, Ohio (Xue); Department of Psychiatry and Behavioral Sciences, University of Washington School of Medicine, Seattle, Washington (Blanchard, Chase, Fortney); Department of Psychiatry and Psychology, Division of Integrated Behavioral Health, Mayo Clinic, Rochester, Minnesota (Park, Leasure); Department of Veterans Affairs, HSR Center of Innovation for Veteran-Centered and Value-Driven Care, VA Puget Sound Health Care System, Seattle, Washington (Fortney); Department of Psychiatry and Behavioral Neuroscience, University of Cincinnati College of Medicine, Cincinnati, Ohio (Cerimele).
Corresponding Author: Ivy Xue, BS, University of Cincinnati College of Medicine, 3230 Eden Ave, Cincinnati, OH 45267 ([email protected]).
Financial Disclosure: None.
Funding/Support: Xue was supported in part by the Warren Liang Medical Student Scholars Program Fund. The parent study was funded by the National Institute of Mental Health (R34MH125935) and supported partly by the National Center for Advancing Translational Sciences (KLTR002317).
Role of the Sponsor: The funders of the parent study had no role in the current analysis.
Supplementary Material: Available at Psychiatrist.com.
References (10)

- American Psychological Association, Presidential Task Force on Evidence-Based Practice. Evidence-based practice in psychology. Am Psychol. 2006;61(4):271–285. PubMed CrossRef
- Fortney JC, Unützer J, Wrenn G, et al. A tipping point for measurement-based care. Psychiatr Serv Wash DC. 2017;68(2):179–188. PubMed CrossRef
- de Jong K, Conijn JM, Gallagher RAV, et al. Using progress feedback to improve outcomes and reduce drop-out, treatment duration, and deterioration: a multilevel meta-analysis. Clin Psychol Rev. 2021;85:102002. PubMed CrossRef
- Cerimele JM, Franta G, Blanchard BE, et al. Bipolar disorder symptom monitoring measures: a mixed-methods study of patient preferences. J Acad Consult-Liaison Psychiatry. 2024;65(2):148–156. PubMed CrossRef
- Kroenke K, Spitzer RL, Williams JBW. The PHQ-9. J Gen Intern Med. 2001;16(9):606–613. PubMed CrossRef
- Cerimele JM, Russo J, Bauer AM, et al. The Patient Mania Questionnaire (PMQ-9): a brief scale for assessing and monitoring manic symptoms. J Gen Intern Med. 2022;37(7):1680–1687. PubMed CrossRef
- Park JH, Breitinger SA, Savitz ST, et al. Delays in bipolar depression treatment in primary care vs. integrated behavioral health and specialty care. J Affect Disord. 2025;369:404–410. PubMed CrossRef
- Google Colab. https://colab.research.google.com/. Accessed August 25, 2025.
- Bauer MS, Simon GE, Ludman E, et al. “Bipolarity” in bipolar disorder: distribution of manic and depressive symptoms in a treated population. Br J Psychiatry. 2005;187(1):87–88. PubMed CrossRef
- Hodgkin D, Merrick EL, O’Brien PL, et al. Testing for clinical inertia in medication treatment of bipolar disorder. J Affect Disord. 2016;205:13–19. PubMed
Enjoy this premium PDF as part of your membership benefits!