Abstract
Objective: To evaluate the performance of the New Hampshire Hospital Screening and Referral Algorithm (NHHSRA) and describe the characteristics of inpatients aged 18–65 years, with serious mental illness (SMI) referred for substance use disorder (SUD) interventions.
Methods: Two questions were evaluated: (1) the accuracy and utility of the NHHSRA in identifying patients appropriate for addiction-focused interventions and (2) associations between referral status and patient characteristics. Receiver operating characteristic (ROC) curve analysis evaluated diagnostic performance of the NHHSRA, with sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), precision, and F1 score assessed. Logistic regressions assessed associations between patient characteristics and referral outcomes. The reference standard (“need for SUD intervention”) was defined as the addiction psychiatrist’s clinical assessment following direct patient evaluation. The patients assessed in this study were admitted to New Hampshire Hospital between January 2023 and February 2025.
Results: The cohort (n = 927) was predominantly male (66.7%), with a mean age of 36.5 years. Opioid use disorder (OUD) was the most prevalent primary SUD (37.9%), followed by alcohol (23.9%), cannabis (15.1%), and methamphetamine (13.7%). The NHHSRA demonstrated excellent performance—sensitivity: 96.6%, specificity: 93.6%, PPV: 98.5%, NPV: 86%, and F1 score: 97.5%. ROC analysis yielded an AUC of 0.82, indicating strong discriminative ability. Logistic regressions identified higher odds of a positive NHHSRA screen among patients with OUD and lower odds among those with cannabis use disorder, after adjusting for age, sex, and psychiatric diagnosis.
Conclusions: The NHHSRA is an accurate, objective tool that enhances identification of SUD intervention needs among inpatients with SMI. By addressing limitations of subjective clinical judgment and patient self-report, its implementation may improve access to addiction services and optimize treatment delivery. Patient characteristics associated with referrals inform targeted strategies for integrated care in this population.
Prim Care Companion CNS Disord 2026;28(2):25m04110
Author affiliations are listed at the end of this article.
Individuals with serious mental illness (SMI)—including schizophrenia, bipolar disorder, and severe major depression—experience disproportionately high rates of co-occurring substance use disorders (SUDs), which are often underrecognized in routine clinical care.1,2 Despite global calls for universal SUD screening and early intervention, inpatient psychiatric settings frequently lack standardized tools tailored to this complex population.3 Most existing screening instruments were designed for primary care or individuals with mild psychiatric symptoms and rely heavily on self-report, limiting their utility in SMI populations and in patients in a behavioral crisis requiring psychiatric hospitalization.3
Among patients with SMI, substance use is associated with greater morbidity, prolonged hospitalizations, and higher readmission rates.4 Conversely, timely identification and intervention can reduce costs and improve outcomes, particularly when initiated during psychiatric hospitalization—a critical opportunity for engagement. Yet without systematic approaches, SUD identification remains inconsistent, relying on clinical judgment alone.5
The New Hampshire Hospital Screening and Referral Algorithm (NHHSRA) was developed to address this gap by using objective clinical data to guide referrals for addiction evaluation among inpatients with SMI.6 Initial validation demonstrated 96% sensitivity and specificity in distinguishing patients who require SUD intervention.6
In this study, we assess the real-world performance of the NHHSRA at scale, compared to clinician-driven referrals, and explore demographic and diagnostic characteristics of referred patients. Characterizing this population and identifying significant associations by age, sex, and specific addictive disorder and psychiatric diagnosis support development of data-informed, targeted strategies to improve care delivery and health equity in psychiatric settings.
METHODS
Overview
This study was reviewed and approved by the Dartmouth-Hitchcock Institutional Review Board (Protocol STUDY02001059), which determined that it met criteria for exempt research. Informed consent was waived because all data were de-identified and derived from routine clinical care. This study received no external funding or support.
Setting
This study was conducted at New Hampshire Hospital (NHH), an inpatient psychiatric facility licensed for 202 beds with a maximum capacity to hold 185 patients located in the northeastern United States. The hospital receives patients from urban, suburban, and rural communities statewide, which supports broad generalizability to diverse clinical settings. Patients are admitted to acute-care units with an average length of stay ranging from 7 to 14 days to several years, influenced by clinical acuity, housing and psychosocial needs, and legal status. Insurance type does not affect access to admission or SUD consultation, as NHH is the designated state facility for all involuntary psychiatric admissions regardless of payer source.
Inpatient SUD interventions available at NHH include initiation or continuation of medications for opioid use disorder (naltrexone, buprenorphine, and methadone), alcohol withdrawal and relapse-prevention pharmacotherapy, other pharmacotherapies with label or off-label evidence for SUD efficacy, and tobacco cessation treatment. Patients also receive motivational interviewing, brief intervention, and referral to outpatient counseling or residential services depending on need.
Sample
The sample included patients with SMI admitted under involuntary status from emergency departments, other inpatient psychiatric units, psychiatric holding facilities, and the community. Patients carry diagnoses of schizophrenia spectrum conditions, bipolar disorders, and severe major depression. On admission, patients undergo psychiatric evaluations and are allocated beds in 1 of 8 units depending on the anticipated length of stay, complexity, and overall treatment needs with patients in each unit managed by either a general psychiatrist or a nurse practitioner. Referrals to addiction services are made according to the clinical assessment of the treating psychiatrist or nurse practitioner. The patients assessed in this study were admitted to NHH between January 2023 and February 2025. Patients older than age 65 were excluded from this study because the NHHSRA was originally developed and validated for individuals aged 18–65 years.
In New Hampshire, involuntary psychiatric admissions follow state statute requiring that patients pose an imminent risk of harm to themselves or others or be unable to care for basic needs due to mental illness. Initial involuntary holds are time-limited (up to 10 days prior to court hearing), which still allows sufficient time for screening, SUD assessment, and initiation of short-term interventions.
Importantly, involuntary admission status does not permit involuntary treatment for SUD. Decisions about medications for withdrawal or relapse prevention remain voluntary unless the patient lacks decision-making capacity, in which case standard medical consent pathways apply.
Some patients experience readmissions, a known phenomenon common in state psychiatric systems. While readmissions were present in this sample, they represented a minority of cases and did not necessitate separate analytic handling because the NHHSRA is applied independently at each admission.
Instrument
The NHHSRA is a clinician-facing tool developed to identify psychiatric inpatients with SMI who may benefit from SUD interventions. Unlike traditional screening instruments that rely on self-report and were developed for general or primary care populations, the NHHSRA addresses the unique needs of inpatient SMI settings.
The NHHSRA utilizes 5 objective data points readily available at the time of admission, including recent positive urine toxicology results, history of SUD diagnoses, legal mandates for treatment, and current pharmacologic SUD treatment regimens. It identifies patients who would benefit from SUD interventions while in the inpatient setting, thereby prompting referral to addiction psychiatry services.
The tool was initially validated in a study of over 300 psychiatric inpatients, demonstrating a sensitivity of 94% and an overall accuracy of 96% in identifying patients appropriate for SUD intervention, when compared against the current gold standard clinician judgment.6 The NHHSRA provides a standardized, reproducible, and scalable method to enhance identification and accurate referral practices for SUD within SMI psychiatric settings. The instrument follows a decision tree structure, where each item represents a yes/no assessment of objective clinical criteria. The algorithm proceeds sequentially: a “yes” at one step may trigger a subsequent assessment or prompt referral, while a “no” may continue the patient along the next branch of the algorithm. This stepwise approach continues until the patient reaches a terminal classification of either “needs SUD intervention” (1) or “does not need intervention” (0). Completion of the NHHSRA can be performed by trained clinical staff at admission; however, for the purpose of this study, it was the addiction psychiatrist who applied it.
Data
As part of routine care at NHH, patients were referred to addiction services by their treating psychiatrist or nurse practitioner if substance use intervention was deemed potentially beneficial. Every referred patient was evaluated directly by a board-certified addiction psychiatrist, who served as the “gold standard” for determining whether a patient required a pharmacologic relapse prevention intervention or whether motivational or relapse prevention psychotherapies with a SUD counselor would be clinically meaningful. The formal consult included clinical interview, electronic health record (EHR) and toxicology review, Prescription Drug Monitoring Program data, and collateral input (eg, information from family). Thus, “need for SUD intervention” was operationalized as 1 = addiction psychiatrist determined an intervention was appropriate and 0 = no intervention recommended. SUD counselors conducted additional therapeutic assessments when clinically indicated, but all final determinations were made by the addiction psychiatrist.
In parallel, the NHHSRA was applied to referred patients to assess its ability to identify those in need of intervention. Data collected included whether the NHHSRA would have flagged the patient, demographic information (age, sex), and psychiatric and SUD diagnosis. While these data capture the most relevant clinical and operational factors, certain variables (such as detailed SUD severity scores, socioeconomic status, and prior outpatient SUD treatment) were not formally included, as they were not part of the NHHSRA or not available in structured, codable fields. Comparisons were then made between clinician-driven referrals and those who would have been identified through the NHHSRA.
Research Aims
- Aim 1: Assess NHHSRA performance (accuracy identifying patients to refer for substance use services, compared to gold standard, clinician-driven referrals).
- Aim 2: Examine associations between substance use intervention referral and patient characteristics (eg, age, sex, psychiatric and SUD diagnosis).
Statistical Analysis
The analytical sample was initially comprised of 1,045 individuals referred to addiction services. After excluding 38 patients for age >65 years and 80 patients with non-SUD classifications (such as gambling) or pain management classification, the final sample size was 927.
Demographic variables included age (categories of 18–19, 20–29, 30–39, 40–49, 50–59, 60–65; Patients aged >65 years were excluded due to potentially nonlinear associations between age and the outcomes of interest) and sex (0 = female, 1 = male). Primary SUD was grouped into 6 exclusive categories: opioids, alcohol, methamphetamine, cocaine, cannabis, and “other” (eg, benzodiazepines, kratom, tobacco, hallucinogens). The first 5 accounted for 93% of the sample.
Principal psychiatric diagnoses, based on Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition criteria, were categorized into the following categories: bipolar disorder, major depressive disorder, schizophrenia spectrum disorders, and borderline personality disorder. These together accounted for 84% of the sample. Less prevalent diagnoses (eg, antisocial personality disorder, posttraumatic stress disorder, attention-deficit/hyperactivity disorder) were combined into an “other” category.
Appropriateness of a substance use intervention referral was determined by the addiction team’s assessment (1 = intervention appropriate vs 0 = no intervention). The addiction team consisted of a board-certified addiction psychiatrist and 2 licensed substance use counselors. All consultations were conducted in person by the appropriate team member, depending on whether therapeutic or pharmacologic input was requested. The NHHSRA was also coded as a binary variable indicating that the individual would algorithmically be classified as needing SUD intervention (1 = NHHSRA identification vs 0 = NHHSRA would not have identified the patient).
All statistical analyses were performed with RStudio 4.5.0 using packages ggplot2, dplyr, and pROC. Descriptive statistics characterized the study sample. Means and SDs were reported for continuous variables, while frequencies and percentages were presented for categorical variables. Independent samples t-tests assessed differences in mean age across primary substances and psychiatric diagnosis. Chi-square and Fisher exact tests were used to examine associations between sex and both primary substance and psychiatric diagnosis. A significance threshold of P <.05 was used throughout.
To assess the predictive accuracy of the NHHSRA in identifying patients in need of SUD interventions, we performed ROC curve analysis. The AUC with 95% CI was reported to evaluate discriminative ability. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), precision, and F1 score were calculated using binary classification metrics, comparing between clinician-driven referral determination (as the gold standard determination of need for SUD intervention) and the NHHSRA determination of need for SUD intervention.7,8
Finally, to examine relationships between patient characteristics and referral for SUD intervention, 2 multiple logistic regression models were used to test associations between all predictor variables (patient age, sex, primary SUD, and psychiatric diagnosis) and the 2 binary outcomes of interest: (1) referral for substance use intervention (yes/no, as determined by the addiction team’s patient assessment process) and (2) screening positive on the NHHSRA (yes/no). Adjusted odds ratios (aORs) and 95% CIs were calculated using the Wald method.
RESULTS
Sample Characteristics
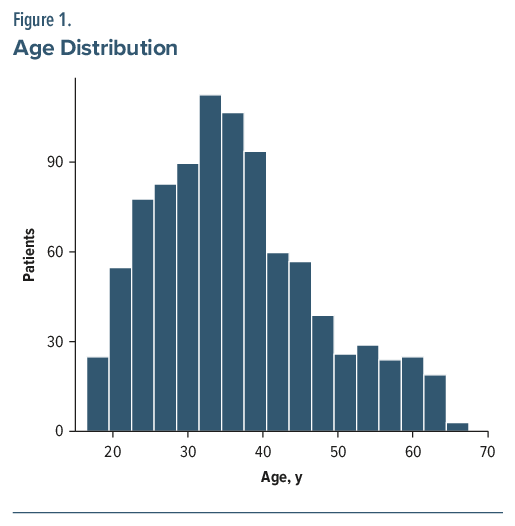
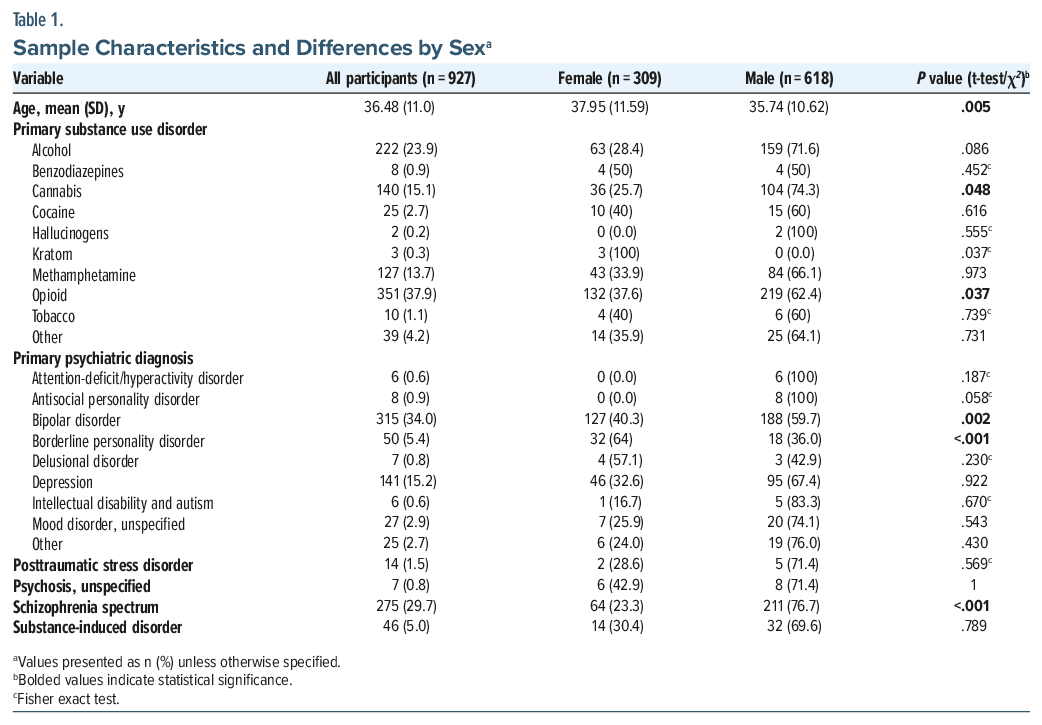
Of 927 patients, one-third were female (33.3%), and the mean age was 36.48 (SD = 11.0) years, with most (66.9%) younger than 40 years (Figure 1.). The most frequently reported primary SUDs comprised opioids (37.9%), alcohol (23.9%), cannabis (15.1%), methamphetamine (13.7%), and cocaine (2.7%) use disorders. The most frequent primary psychiatric diagnoses were bipolar disorder (34.0%), schizophrenia spectrum disorders (29.7%), and major depressive disorder (15.2%), with less frequent diagnoses including borderline personality disorder, unspecified mood disorder, and posttraumatic stress disorder (Table 1.).
Sex and Age Comparisons
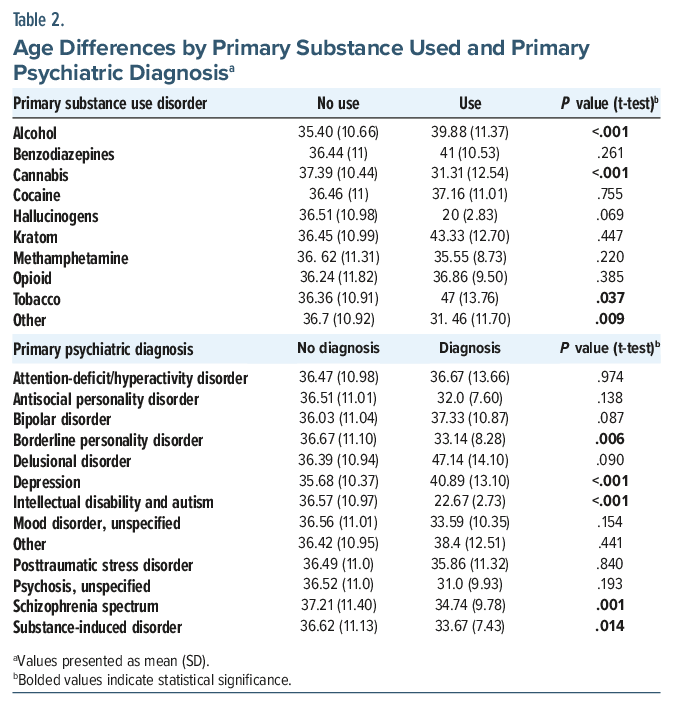
Females were slightly older (P =.005) (Table 1), and fewer had cannabis (25.7% vs 74.3%, P=.048) or opioids (37.6% vs 62.4%, P=.037) as primary SUD. Females also more often had borderline personality disorder (64.0% vs 36%, P <.001), while males had higher rates of bipolar disorder (59.7% vs 40.3%, P=.002) and schizophrenia spectrum disorders (76.7% vs 23.3%, P <.001). Patients with cannabis use disorder were younger on average (mean = 31.3, SD=12.5 vs mean=37.4, SD=10.4; P <.001) (Table 2). Patients with depression were older on average (mean=40.89, SD=13.10 vs mean=35.68, SD=10.37), and those with schizophrenia spectrum disorders were younger (mean=34.74, SD=9.78 vs mean=37.21, SD=11.40) (Table 2).
Aim 1: NHHSRA Performance
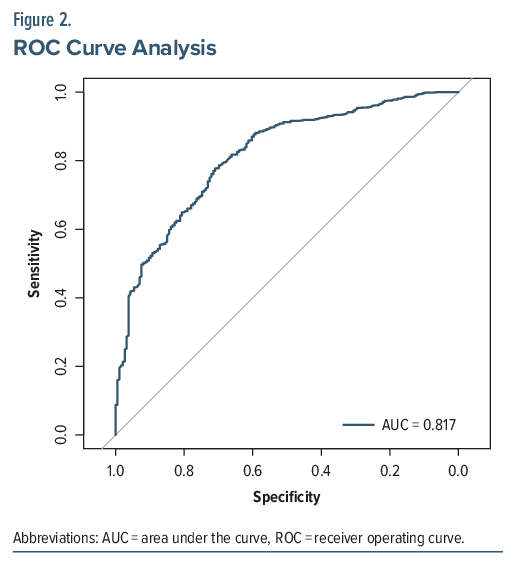
The NHHSRA demonstrated excellent performance in identifying patients in need of SUD intervention when compared to clinical-based referral. Of the total 927 patients, 730 “true positives” (patients identified as needing an SUD intervention per both the NHHSRA and the clinician evaluation) and 160 “true negatives” (patients identified as not needing an SUD intervention per both the NHHSRA and clinician evaluation) were identified. In turn, 11 “false positives” (patients flagged by the NHHSRA for intervention but not identified as needing SUD intervention based on clinician evaluation) and 26 “false negatives” (patients not flagged by the NHHSRA for intervention who were identified as needing SUD intervention based on clinician evaluation) were identified. Sensitivity was 96.6%, specificity 93.6%, PPV 98.5%, and NPV 86%. The overall model accuracy was 95.5%, and the F1 score was 97.5%, indicating strong overall test performance. ROC analysis showed an AUC of 0.82 (95% CI, 0.78–0.85), indicating good discriminative ability (Figure 2.).
Aim 2: Association Between SUD Intervention Referral and Patient Characteristics
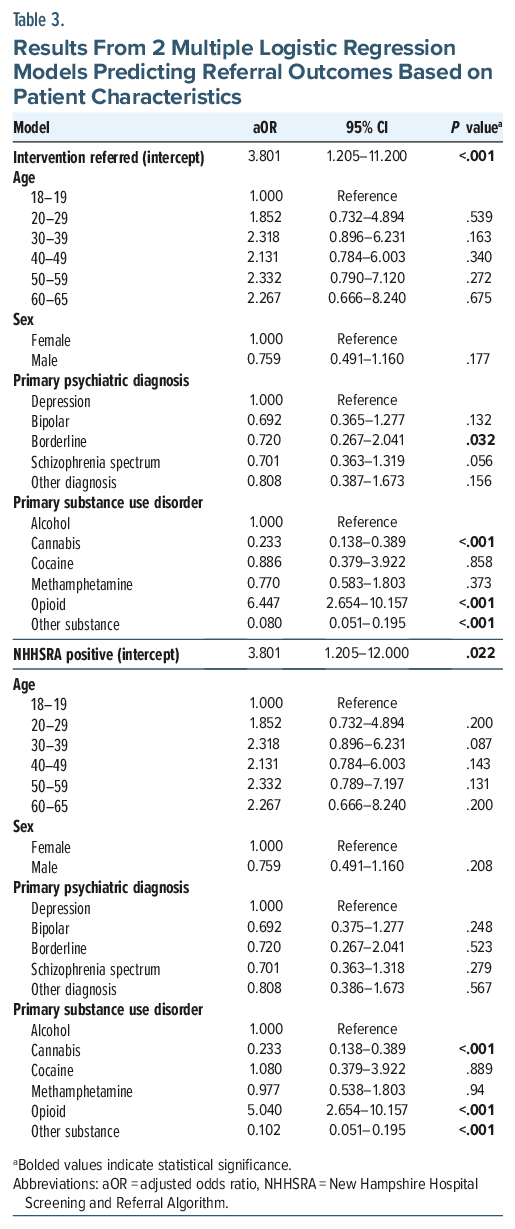
In the multiple logistic regression model predicting whether an SUD intervention was recommended by the addiction team members, cannabis use disorder (aOR=0.23; CI, 0.14–0.39; P <.001) and “other substance” use disorder (aOR=0.08; CI, 0.04–0.15; P <.001) were each associated with lower adjusted odds of receiving a recommendation for SUD intervention, relative to alcohol use disorder; in contrast, opioid use disorder was associated with higher adjusted odds (aOR=6.45; CI, 3.11–14.71; P <.001). Patients with borderline personality disorder had lower adjusted odds of receiving a recommendation for SUD intervention (aOR=0.36; CI, 0.13–0.99; P=.045) compared to those with depression.
In the multiple logistic regression model predicting the NHHSRA screening determination, patients with cannabis use disorder (aOR = 0.22; 95% CI, 0.13–0.37; P < .001) as well as “other substance” use disorder (aOR = 0.10; 95% CI, 0.05–1.82; P < .001) had significantly lower adjusted odds of screening positive compared to those with alcohol use disorder. Conversely, opioid use disorder was strongly associated with increased adjusted odds of screening positive on the NHHSRA (aOR = 5.21; 95% CI, 2.75–10.48; P < .001) (Table 3).
DISCUSSION
This study supports the NHHSRA’s high accuracy and robust predictive validity, with sensitivity exceeding 96% and specificity over 93% when compared against the current gold standard of clinician judgment. The gold standard assessment incorporated not only patient-level clinical factors, such as substance use severity and psychiatric comorbidities, but also unit-level considerations including staffing, resource availability, prior treatment history, and anticipated feasibility of intervention. These findings align with the initial validation study of the NHHSRA, which demonstrated similarly high sensitivity and accuracy, underscoring the algorithm’s reliability and reproducibility in clinical practice.6 This supports prior calls in the literature emphasizing the need for objective, standardized tools specifically tailored for SMI populations to overcome limitations inherent in traditional self-report–based screening instruments.9,10
The decision to exclude adults aged >65 years reflects both methodological and clinical considerations. The NHHSRA was originally validated in patients aged 18–65 years and, applying it outside that range without prior adaptation could introduce misclassification. Additionally, the clinical needs and intervention feasibility of adults aged >65 years often differ from younger patients, further supporting the exclusion.
The demographic and clinical characteristics of patients referred for SUD interventions reveal important patterns consistent with existing research. Opioid use disorder emerged as a significant predictor for both positive NHHSRA screening and receipt of intervention, reflecting the widespread opioid epidemic documented extensively in psychiatric populations worldwide.11 Studies have highlighted opioids as a predominant substance linked with increased morbidity among patients with SMI, and our findings corroborate these concerns. Conversely, cannabis and “other” SUDs were associated with lower odds of identification and intervention. It should be noted that the “other” category included only a small number of patients, limiting specific intervention data for substances such as kratom, long-term benzodiazepine tapering, or other novel substances of abuse, but these patients were still considered for SUD intervention as appropriate. This observation is consistent with prior literature suggesting underdetection and undertreatment of cannabis use disorder, potentially due to clinician biases, stigma, or variable clinical emphasis on certain substances.12 The association of younger age with cannabis use disorder and older age and male sex with alcohol use disorder further reflects known demographic trends reported in epidemiological studies.13
Psychiatric diagnosis significantly influenced intervention referral likelihood, consistent with prior clinical and epidemiological research.13 Notably, the lower likelihood of SUD intervention from clinician-driven referral among patients with borderline personality disorder, despite its known association with substance misuse, raises important questions about clinical recognition and service engagement barriers, an area previously identified as underexplored in the literature.11 In contrast to clinician-driven referrals, the adjusted odds of screening positive on the NHHSRA were not significantly different for patients with borderline personality disorder.
By leveraging objective clinical data such as urine toxicology, SUD diagnoses, and pharmacologic regimens, as well as treatment mandates, the NHHSRA addresses a critical gap in SUD screening for SMI populations. This approach aligns with recommendations from health authorities advocating for systematic, evidence-based screening strategies to improve diagnostic accuracy and intervention timeliness.12 Moreover, it addresses a structural gap in psychiatric hospital services, which traditionally consider SUD a problem not to intervene substantially upon while in the hospital and to refer to outpatient services after the crisis is stabilized, rather than a problem to integrate into a patient’s treatment plan. The NHHSRA’s standardized framework overcomes the challenge of limited subjective information from acutely decompensated patients with SMI upon admission and minimizes variability caused by individual clinical judgment, thereby fostering more equitable access to addiction services—an issue increasingly highlighted in recent health disparities research.11 While other hospitals may have differing lengths of stay, staffing ratios, and available interventions, the NHHSRA can be adapted to complement local clinical judgment, supporting broader generalizability.
The findings should be interpreted in the context of several limitations. First, collapsing categories with small cell counts into broader groups may have masked important distinctions among less prevalent psychiatric diagnoses or substance use types. Second, the NHHSRA’s performance and the gold standard assessment may be influenced by resource availability, staff expertise, and patient history, factors that might vary in other settings. Third, measures related to other relevant patient characteristics (eg, severity of SUD, SUD history, socioeconomic status, among others) were outside of the study scope. Fourth, the use of mutually exclusive categories for primary substance and psychiatric diagnosis does not fully reflect the high prevalence of comorbidity and polysubstance use in this population.
Future research should focus on prospective, multisite validation of the NHHSRA across diverse inpatient settings and patient populations. Integration of the algorithm into EHR systems and clinical workflows may enhance scalability and real-time clinical decision support, an implementation strategy supported by recent advances in health informatics literature.14 Future work may also examine potential refinements to the algorithm, such as weighting steps based on resource availability, staff experience, and substance-specific considerations. Additionally, assessing the impact of standardized screening on patient outcomes, treatment engagement, initiating or continuing evidence-based interventions for SUD, and health equity is critical to advancing addiction care for individuals with SMI. Tailoring interventions based on substance-specific and diagnosis-specific risk profiles, as suggested by our findings and prior work, could further refine care strategies.
Importantly, the NHHSRA has been piloted at NHH and is being considered for global integration into clinical workflows, providing decision support to clinicians without significant time burden. Its standardized format allows for efficient application while still permitting clinician discretion, ensuring that individual patient needs and context are considered.
In summary, the NHHSRA represents a significant advancement in addressing the persistent challenge of systematic SUD identification among SMI inpatients. Its demonstrated accuracy and utility support its broader adoption to improve consistency, equity, and effectiveness of addiction services within psychiatric care, ultimately fostering better health outcomes for this vulnerable population.
CONCLUSION
This study demonstrates the NHHSRA’s high accuracy in identifying psychiatric inpatients with SMI who are in need of SUD interventions, showing excellent sensitivity (96.6%) and specificity (93.6%). The algorithm’s performance supports its potential as a scalable, objective tool to complement clinician judgment and address gaps in SUD identification within this vulnerable population. Our analysis further reveals important demographic and diagnostic trends: opioid use disorder was strongly associated with higher odds of both screening positive and receiving intervention, while cannabis and “other” SUD were associated with decreased odds compared to alcohol use disorder. Age and sex differences also emerged, with younger SMI patients more likely to have cannabis use disorder and older SMI patients more likely to have alcohol use disorder.
These findings highlight the imperative to integrate standardized, data-driven screening methods like the NHHSRA into inpatient psychiatric workflows to improve identification and referral for SUD care. Doing so may reduce morbidity, shorten hospital stays, and decrease readmission rates.
Article Information
Published Online: March 31, 2026. https://doi.org/10.4088/PCC.25m04110
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 15, 2025; accepted December 16, 2025.
To Cite: Stanciu CN, Timmons P, Fetter JC, et al. Substance use referrals among inpatients with serious mental illness: clinical characteristics and real-world evaluation of the New Hampshire Hospital Screening and Referral Algorithm. Prim Care Companion CNS Disord 2026;28(2):25m04110.
Author Affiliations: Dartmouth Geisel School of Medicine, Hanover, New Hampshire (Stanciu, Fetter); New Hampshire Hospital, Concord, New Hampshire (Stanciu, Fetter); Arizona State University, College of Health Solutions, Phoenix, Arizona (Timmons); Arizona State University, School of Social Work, Phoenix, Arizona (Cano).
Corresponding Author: Patricia Timmons, MSN, RN, 550 N 3rd St Ste 501, Phoenix, AZ 85004 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
ORCID: Cornel N. Stanciu: https://orcid.org/0000-0002-5978-1492; Patricia Timmons: https://orcid.org/0000-0002-7583-5825
Clinical Points
- The New Hampshire Hospital Screening and Referral Algorithm showed high accuracy in identifying psychiatric inpatients with serious mental illness (SMI) in need of substance use disorder (SUD) interventions, with excellent sensitivity (96.6%) and specificity (93.6%).
- Opioid use disorder was strongly associated, with higher odds of both screening positive and receiving intervention, while cannabis and “other” SUD were associated with decreased odds compared to alcohol use disorder.
- Age and sex differences were found, with younger SMI patients more likely to have cannabis use disorder and older SMI patients more likely to have alcohol use disorder.
References (14)

- Common Comorbidities with Substance Use Disorders Research Report. Bethesda (MD): National Institutes on Drug Abuse (US); 2020. Available from: https://www.ncbi.nlm.nih.gov/books/NBK571451
- Woodward D, Wilens TE, Glantz M, et al. A systematic review of substance use screening in outpatient behavioral health settings. Addict Sci Clin Pract. 2023;18(1):18. PubMed CrossRef
- Sweetman J, Raistrick D, Mdege ND, et al. A systematic review of substance misuse assessment packages. Drug Alcohol Rev. 2013;32(4):347–355. PubMed CrossRef
- Carey KB, Correia CJ. Severe mental illness and addictions: assessment considerations. Addict Behav. 1998;23(6):735–748. PubMed CrossRef
- Substance Use Disorder Treatment for People With Co-occurring Disorders: Updated 2020 [Internet]. Rockville (MD): Substance Abuse and Mental Health Services Administration (US); 2020. (Treatment Improvement Protocol (TIP) Series, No. 42.) Chapter 3—Screening and Assessment of Co-occurring Disorders. https://www.ncbi.nlm.nih.gov/books/NBK571017
- Stanciu CN, Healey CJ, Emeny RT, et al. The New Hampshire Hospital Screening and Referral Algorithm (NHHSRA) for substance use in people with serious mental illness. Prim Care Companion CNS Disord. 2023;25(3):22m03410. PubMed CrossRef
- Zou KH, O’Malley AJ, Mauri L. Receiver-operating characteristic analysis for evaluating diagnostic tests and predictive models. Circulation. 2007;115(5):654–657. PubMed
- Li J. Area under the ROC curve has the most consistent evaluation for binary classification. PloS One. 2024;19(12):e0316019. PubMed CrossRef
- Reilly J, Meurk C, Heffernan E, et al. Substance use disorder screening and brief intervention in routine clinical practice in specialist adult mental health services: a systematic review. Aust N Z J Psychiatry. 2023;57(6):793–810. PubMed CrossRef
- Large MM, Smith G, Sara G, et al. Meta-analysis of self-reported substance use compared with laboratory substance assay in general adult mental health settings. Int J Methods Psychiatr Res. 2012;21(2):134–148. PubMed CrossRef
- Bahji A. Navigating the complex Intersection of substance use and psychiatric disorders: a comprehensive review. J Clin Med. 2024;13(4):999. PubMed CrossRef
- European Monitoring Centre for Drugs and Drug Addiction. Comorbidity of Substance Use and Mental Health Disorders in Europe (Perspectives on Drugs). Publications Office of the European Union; 2016. https://www.euda.europa.eu/publications/pods/comorbidity-substance-use-mental-health_en
- Ringeisen H, Edlund MJ, Guyer H, et al. Mental and Substance Use Disorders Prevalence Study: Findings Report. RTI International; 2023.
- UNC School of Public Health. Integrating Substance Use Disorder Screening into Behavioral Health Services: Implementation Strategies. UNC School of Public Health; 2022.
Enjoy this premium PDF as part of your membership benefits!





