Autoimmune encephalitis (AE) is an immune-mediated disorder caused by autoantibodies to synaptic proteins, manifesting with seizures, cognitive impairment, and psychiatric symptoms. Despite increasing knowledge of the disease, its rarity (roughly 14 cases per 100,000 people) and diverse clinical presentations make early identification of AE challenging.1 We report the case of a patient with probable antibody-negative AE, whose initial workup mimicked a primary psychiatric disorder.
Case Report
A previously healthy 23-year-old woman presented with 2 weeks of recurrent seizure-like episodes and rapidly evolving psychosis (disorganized speech, auditory/visual hallucinations). The neurology team directly observed some seizure-like episodes. Electroencephalogram (EEG) showed background slowing but no epileptiform activity, and magnetic resonance imaging (MRI) of the brain was normal; thus, she was diagnosed with psychogenic nonepileptic seizures. The patient was admitted to inpatient psychiatry care for a presumed primary psychotic condition. Despite multiple psychotropic trials, including aripiprazole, quetiapine, olanzapine, and valproate, the patient continued to deteriorate, with prominent bizarre behaviors such as spending most of the day crawling on the floor.
On hospital day 19, the patient mentioned vision changes, and ophthalmology noted papilledema. Lumbar puncture revealed opening pressure of 32 cm H2O, white blood cell count of 95 cells/µL, lymphocyte predominant, and red blood cell count of 50 cells/µL, with negative herpes simplex virus and cytomegalovirus by polymerase chain reaction. Serology for paraneoplastic antibodies and N-methyl-D-aspartate receptor (NMDA-R) autoantibodies was negative. The cerebrospinal fluid (CSF) autoimmune panel was inconclusive due to insufficient volume.
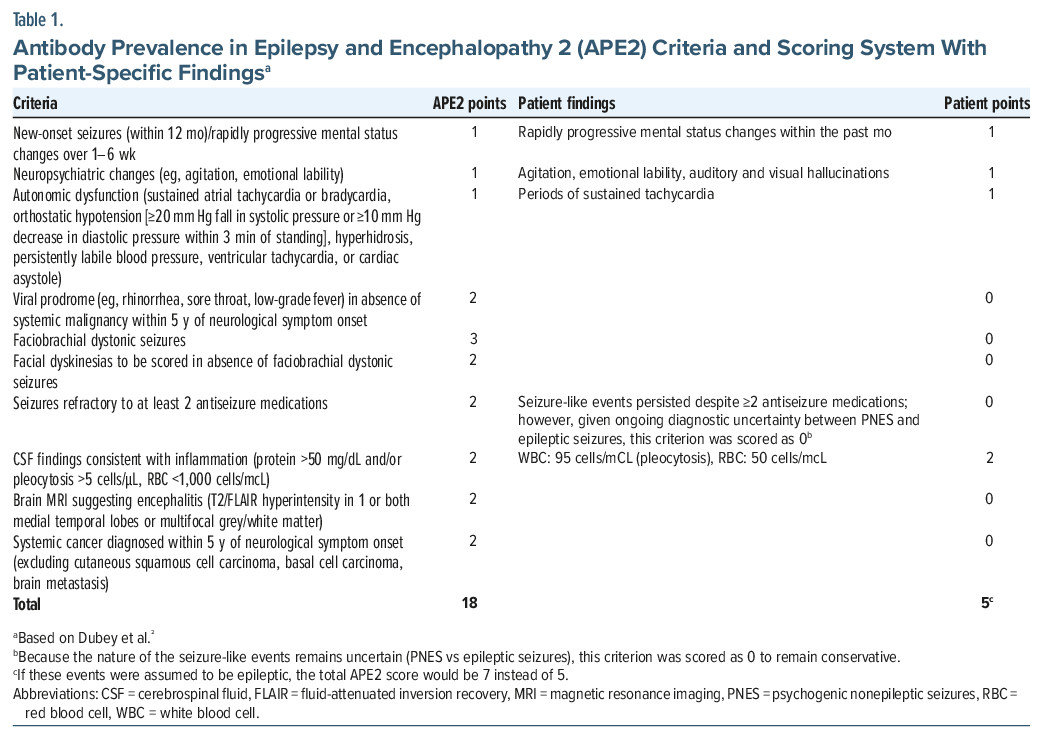
Given the subacute psychiatric symptoms, CSF inflammation, and evidence of increased intracranial pressure, with an infectious cause reasonably excluded, the most likely diagnosis was AE. This diagnosis was supported by an Antibody Prevalence in Epilepsy and Encephalopathy (APE2) score of 5 (Table 1).2 Psychotropic medications were subsequently discontinued, and the patient was treated with intravenous methylprednisolone for 5 days, followed by oral prednisone, with marked improvement in cognitive and mental status by discharge on day 35.
Discussion
This case highlights 3 diagnostic pitfalls. First, AE seizures may be subtle; for example, faciobrachial dystonic seizures—a pathognomonic manifestation of antileucine-rich glioma inactivated 1 encephalitis—present as brief tonic contractions and are easily misclassified.3 Second, negative structural brain findings or seizures on MRI and EEG do not exclude AE. Fluorodeoxyglucose positron emission tomography scan is more sensitive for diagnosing AE, although it is less available.4,5 The third pitfall is that negative serology early in the course does not preclude AE—diagnosis remains primarily clinical, guided by CSF inflammation and exclusion of alternatives.
Objective tools can help with the diagnosis of AE. APE2 criteria were found to have as high as 99% sensitivity and 93% specificity for AE.2 Our patient meets the criteria of ≥4 points based on rapid mental status change/neuropsychiatric features, autonomic dysfunction, and CSF pleocytosis (with minimal red blood cell contamination), crossing the threshold associated with neural-specific antibody positivity and supporting early immunotherapy when infections are excluded.
Early treatment is linked to better outcomes in AE (eg, anti-NMDA-R), and some patients require second-line or prolonged therapy.6,7 Best practices emphasize starting immunotherapy once AE is highly suspected and infectious etiologies are excluded based on CSF results.8 While our patient had a low likelihood of an infectious cause based on history and initial screenings, confirmation with lumbar puncture was delayed until hospital day 20. Given AE’s neuroinflammatory nature, timely corticosteroid administration could have been considered even without confirmed antibodies. However, response alone should not be viewed as diagnostic, given that some patients also may not respond to immunotherapy or need intensive or prolonged treatment.8 Overall, this case highlights that a higher level of suspicion for AE is warranted when the patient presents with atypical neuropsychiatric symptomatology.
Article Information
Published Online: March 19, 2026. https://doi.org/10.4088/PCC.25cr04083
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04083
Submitted: September 12, 2025; accepted November 26, 2025.
To Cite: Luu S, Kong Y, Sokolic M, et al. An atypical presentation of autoimmune encephalitis. Prim Care Companion CNS Disord 2026;28(2):25cr04083.
Author Affiliations: Department of Psychiatry, Rutgers New Jersey Medical School, Newark, New Jersey (Luu, Kong, Chern, Ali, Rutkowski); Department of Psychiatry, Rutgers Robert Wood Johnson, Piscataway, New Jersey (Sokolic).
Corresponding Author: Skylar Luu, Department of Psychiatry, Rutgers New Jersey Medical School, 185 S Orange Avenue, Newark, NJ 07103 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and information has been de-identified to protect patient anonymity.
References (8)

- Dubey D, Pittock SJ, Kelly CR, et al. Autoimmune encephalitis epidemiology and a comparison to infectious encephalitis. Ann Neurol. 2018;83(1):166–177. PubMed CrossRef
- Dubey D, Kothapalli N, McKeon A, et al. Predictors of neural-specific autoantibodies and immunotherapy response in patients with cognitive dysfunction. J Neuroimmunol. 2018;323:62–72. PubMed CrossRef
- Irani SR, Michell AW, Lang B, et al. Faciobrachial dystonic seizures precede Lgi1 antibody limbic encephalitis. Ann Neurol. 2011;69(5):892–900. PubMed CrossRef
- Probasco JC, Solnes L, Nalluri A, et al. Abnormal brain metabolism on FDG-PET/CT is a common early finding in autoimmune encephalitis. Neurol Neuroimmunol Neuroinflamm. 2017;4(4):e352. PubMed CrossRef
- Probasco JC, Solnes L, Nalluri A, et al. Decreased occipital lobe metabolism by FDG-PET/CT: an anti-NMDA receptor encephalitis biomarker. Neurol Neuroimmunol Neuroinflamm. 2018;5(1):e413. PubMed CrossRef
- Du Y, Zhao C, Liu J, et al. Simplified regimen of combined low-dose rituximab for autoimmune encephalitis with neuronal surface antibodies. J Neuroinflammation. 2022;19(1):259. PubMed CrossRef
- Titulaer MJ, McCracken L, Gabilondo I, et al. Treatment and prognostic factors for long-term outcome in patients with anti-NMDA receptor encephalitis: an observational cohort study. Lancet Neurol. 2013;12(2):157–165. PubMed CrossRef
- Abboud H, Probasco JC, Irani S, et al. Autoimmune encephalitis: proposed best practice recommendations for diagnosis and acute management. J Neurol Neurosurg Psychiatry. 2021;92(7):757–768. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!