Depression is predicted to be the most common cause of disability in the coming decade. Self-inflicted hammer blow to the cranium is a rare phenomenon seen in patients with a history of attempted suicide. The resulting comminuted depressed skull fracture of the midline vertex is life threatening. Rapid interdisciplinary communication and intervention are essential to reduce morbidity and mortality. We present a case of self-inflicted hammer blows to the head, review the relevant literature on this topic, and discuss neurosurgical and psychiatric implications.
Self-Inflicted Hammer Blows to the Cranial Vault:
An Interdisciplinary Challenge
ABSTRACT
Depression is predicted to be the most common cause of disability in the coming decade. Self-inflicted hammer blow to the cranium is a rare phenomenon seen in patients with a history of attempted suicide. The resulting comminuted depressed skull fracture of the midline vertex is life threatening. Rapid interdisciplinary communication and intervention are essential to reduce morbidity and mortality. We present a case of self-inflicted hammer blows to the head, review the relevant literature on this topic, and discuss neurosurgical and psychiatric implications.
Prim Care Companion CNS Disord 2016;18(3):doi:10.4088/PCC.15br01927
© Copyright 2016 Physicians Postgraduate Press, Inc.
aDepartment of Neurosurgery, Justus Liebig University Giessen, Germany
bDepartment of Psychiatry and Psychotherapy, Friedberg Hospital, Friedberg, Germany
*Corresponding author: Kartik G. Krishnan, MD, PhD, Department of Neurosurgery, Justus Liebig University Giessen, Klinikstrasse 33, 35392 Giessen, Germany
([email protected]).
Depression is ranked among the most common, disabling disorders and is one of the major health threats of the 21st century.1 In a report from October 2012, the World Health Organization2 estimated that 350 million people worldwide suffer from depression and that depression is predicted to be the most common cause of disability by the year 2020. Beyond its burden on society, depression is associated with worse global outcomes for the affected individual, which include (1) reduced social functioning, (2) reduced quality of life with regard to general health, (3) inability to return to work and sustain oneself, and (4) attempts at suicide.3–5
The Global Burden of Disease study6 also reported that suicide was the 13th leading cause of death globally and was more prevalent in regions with advanced health care systems. Suicide accounted for 5% of female and 6% of male deaths in persons aged 15–49 years old and 884,000 deaths across all ages.6
There are numerous methods of suicide. Self-inflicted blows to the cranium with a hammer are a very rare phenomenon and life threatening, due to the risk of laceration of the superior sagittal sinus and resulting rapid exsanguination. This article reports a rare case of self-inflicted hammer blow to the cranial vault, reviews the relevant literature, and discusses the neurosurgical and psychiatric implications.
CASE REPORT
Mr A, a 54-year-old right-handed white man who grew up as an only child, has suffered from agitation, anxiety, and depressive phases since his early youth. Since the age of 17 years, he has consumed alcohol on a daily basis (mainly beer up to 10 bottles per day, sometimes brandy, and wine on rare occasions). The patient denied the use of illegal drugs. Tranquillizers prescribed for his restlessness and anxiety in the past failed to improve his symptoms. Mr A attempted suicide for the first time in 2001 at the age of 41 years by cutting across his left wrist. Since that time, he has undergone continuous psychotherapy and a long-term medical rehabilitation program. He had a total of 4 recorded inpatient hospitalizations since 2002, mainly due to alcohol withdrawal syndrome and acute psychiatric crises, which seem to have been caused by feeling overburdened or being left alone.
Mr A’s first hospital stay resulted from a feeling of abandonment and associated anxiety when his girlfriend had to be hospitalized for a prolonged, however predictable, time for an elective surgical procedure. The second hospitalization was 18 months later with similar symptoms of being abandoned when his girlfriend seemed to have left him for no specific reasons after their wedding date was already arranged. After a crisis intervention, Mr A was stabilized quickly and was discharged for outpatient treatment on a daily basis.
For the next 10 years, he continued to receive predominantly outpatient treatment. Under such care, Mr A was increasingly able to manage his states of anxiety and avoid suicidal crises. Although he consistently exhibited a behavior of hitting his head against a wall in situations of increased angst, he was usually able to return to a state of a “clear head” without causing serious injury to himself. The one distinct symptom Mr A repeatedly mentioned to have experienced during each phase of agitation was an increase in pressure within his head.
Mr A’s symptoms worsened in September 2014, as the entire responsibility of taking care of his parents fell on his shoulders soon after the untimely death of a supporting family member. Both of his parents suffer from dementia, and his mother is also blind and diabetic. The strain of caring for his parents all by himself had triggered a state of angst and anxiety. After spending a restless night yelling at his parents, Mr A had attempted suicide by strangling himself with a rope. This suicide attempt led to his next inpatient treatment stay at the psychiatric ward. Additional psychotherapy and psychopharmacologic therapy were administered on an inpatient basis. After his symptoms disappeared and he was deemed to have become more reflective and accepting of his present responsibilities, he was discharged home.
The incident reported here occurred on the same night after his discharge from inpatient care: being home alone with his severely disabled parents had triggered fear and panic attacks. As Mr A described the incident later, he again felt an internal pressure mounting inside his head and had to immediately “release” the internal pressure. In this state, he grabbed a metal hammer and repeatedly hit himself on the head in the presence of his mother. After severe bleeding, he lost consciousness. The police as well as the emergency team were notified. Mr A was intubated at the scene of the incident and brought to our Accidents and Emergency Department for further diagnosis and treatment.
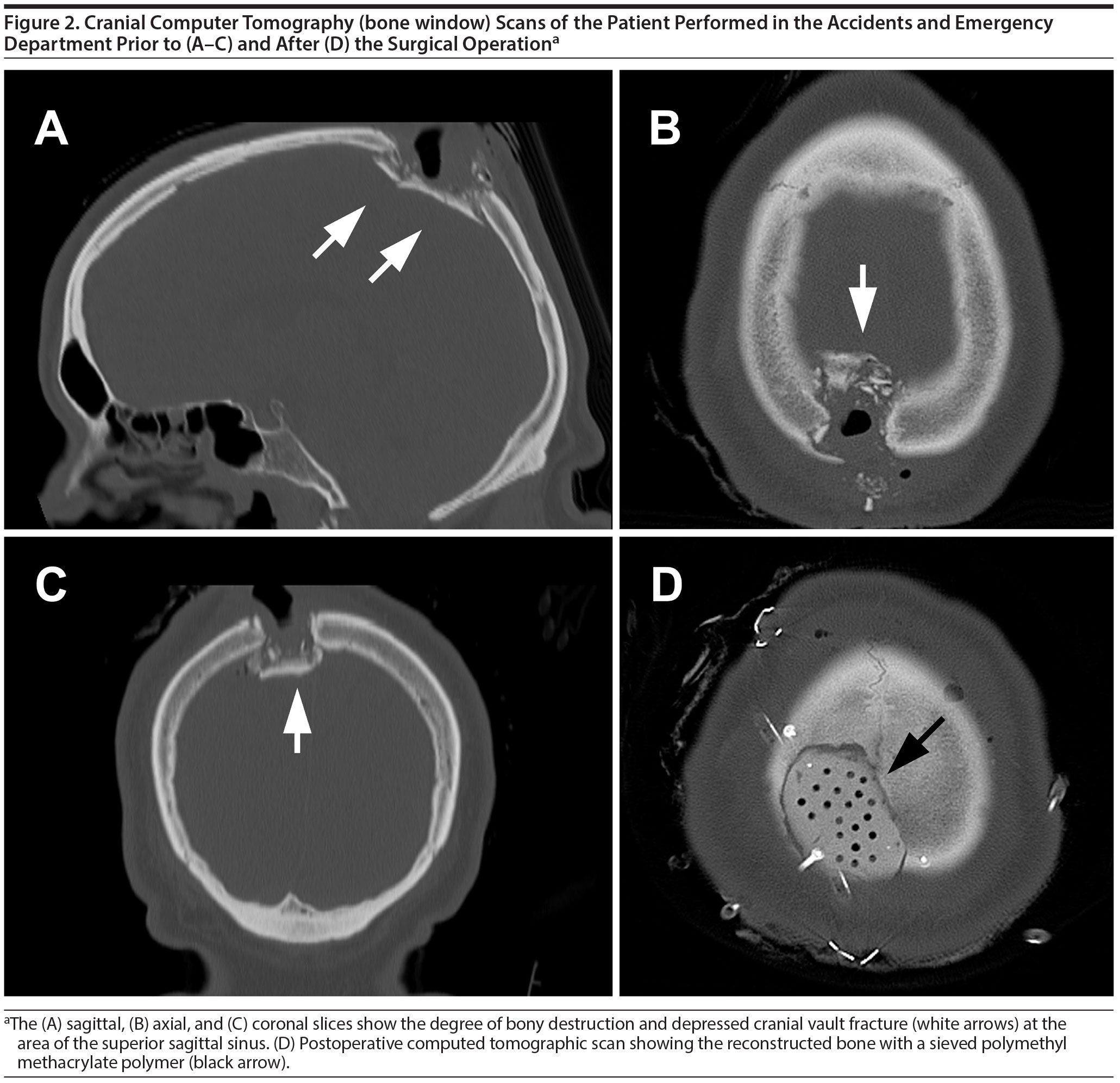
Mr A had a severely lacerated and actively bleeding wound on the vertex (Figure 1). Several free-floating bone fragments were palpable. Computed tomography of the neurocranium showed a comminuted depressed fracture of the parietal cranial vault directly on top of the superior sagittal sinus (Figure 2A–C; Figure 2D shows postoperative computed tomography). After stabilizing his hemodynamic condition, the patient underwent an emergency surgical operation. Exploration showed that the superior sagittal sinus was marginally lacerated and the bleeding had arrested itself with a large clot (Figure 3A and B). The bone fragments were removed. The superior sagittal sinus was sealed using Tisseel fibrin glue (Baxter International Inc, Deerfield, Illinois) and Spongostan gelatin wafer (Ferrosan Medical Devices, Søborg, Denmark) (Figure 3C); the bony defect was reconstructed using extempore-prepared, self-hardening polymethyl methacrylate paste (Figure 3D). The integumentary defect from the multiple lacerations was reconstructed by rotational advancement scalp flaps (Figure 3E and F).


Mr A received postoperative care in the neurosurgical intensive care unit. He was weaned off anesthesia quickly and extubated. He had no gross neurologic deficits after awakening from induced coma. The wound healing was uneventful. After a few days of neurosurgical intensive care, Mr A was transferred back to the psychiatric ward.
LITERATURE REVIEW
Patients with a combined personality, panic, psychological, and behavioral disorder usually initially present with simple alcohol addiction. Overall, our patient’s disorder was kept under control (largely dormant), with the exception of a few impulsive breakdowns in the last 14 years. Thus, Mr A could take more responsibility for himself with psychiatric and psychopharmacologic support on an outpatient basis alone. However, the untimely loss of a relative who supported Mr A in the care of his parents had triggered the feeling of abandonment anew. Feeling pressure within one’s head and wanting to release it by opening one’s own skull is an extremely rare phenomenon. A thorough review of the literature showed 1 case8 of hammering nails through the skull into the brain and 4 cases7,9,10 of attempted suicide by hammer blows. Two patients were reported to have survived,8,10 and in 3 cases of hammer blows to the vertex,7,9 the patients died of bleeding from the superior sagittal sinus. Park et al7 recently published 2 cases of self-inflicted suicidal hammer blows strikingly similar to the one we describe here and derived forensic implications from them.
Fracture of the cranial vault in the anatomic neighborhood of the superior sagittal sinus is life threatening, since laceration of the sinus can lead to exsanguination. Dural involvement and contusion of the brain parenchyma are further complications of head injury. In our case, the comminuted fracture of the cranial vault, despite being directly on top of the parietal superior sagittal sinus, had only partially lacerated the superior sagittal sinus and had not lacerated the dura mater. These findings correlate with those of the autopsies reported by Park et al.7 Had our patient continued further with the repetitive blows he had been inflicting on himself, he would have died.
Immediate surgical management is warranted in acute conditions involving depressed fractures of the cranial vault, especially with a possible involvement of the sinuses. Repeated blunt hammer blows to the vertex result in typical lacerations of the skin and multiple depressed and comminuted fractures of the cranial vault with or without the involvement of the venous sinuses and the dura mater. Thus, surgical management is quite challenging from several points of view: surgical management should be quick or the sinus bleeding will lead to exsanguination and the reconstruction has to be performed in several layers (sinus and dura mater, bone, and the lacerated integumentary coverage). For cranioplasty, various materials have been described and are commercially available.11,12 All of the materials follow the same decisive principles: biomechanical strength and stability, apt fit into the defect, resistance to infections, biocompatibility, osteoconductivity, and osteoinductivity.11,12 Autologous rib grafts have been shown to be effective for cranioplasty.13–15 However, they are quite cumbersome, require a donor site operation, and have associated risks and a donor site defect. Synthetic materials include celluloid, polymethyl methacrylate, polyethylene, silicon, and ceramic and metal or metallic alloys (aluminum, gold, silver, titanium).16 Polymethyl methacrylate is known for its favorable properties when used in cranioplasty: it is light and formable; once hardened, it does not radiate heat; it is radiopaque—at the same time it does not produce artifacts like metallic alloys—it is visible in all forms of radiologic diagnoses just like the bone; it is relatively inexpensive; and, above all, it is inert and biocompatible. Polymethyl methacrylate is one of the most widely used materials in bone reconstruction.17,18
The typical laceration pattern of the skin resulting from repeated hammer blows to the vertex also poses a reconstructive surgical challenge, as leaving an open skin defect directly on the cranium leads to sequestration, infection, and marmorisation of the underlying bone. The diploё of the cranial bone is ideally suited as a reservoir for invading bacteria, which when untreated eventually leads to meningitis and associated grave complications. Thus, albeit appearing a little trivial (during the emergency phase) in comparison to brain damage, sinus laceration, and exsanguination, the immediate reconstruction of the integumentary defect of the cranial vault is indeed of vital importance and not the least inconsequential. Integumentary coverage of defects on the head is achieved by several means: skin grafting alone, rotational and advancement skin flaps in combination with or without skin grafting, and free tissue transfer.19 In order to graft skin on a bony surface, it is necessary to have a well-perfused periosteal or fascial layer. Skin grafting directly on a bony surface leads to parched skin graft and rejection. Thus, mobilization of 1 skin flap or more from the anatomic neighborhood to cover such a defect is mandated. The skin flaps are raised in such a manner that a layer of galea periosteum is left attached to the bone. After mobilization and rotation of the flaps to the recipient area, the resulting donor defect is skin grafted. Very large and complex defects are better treated using free vascularized tissue transfer options.19
The lifetime management of patients with depression is challenging because of the dynamic, chronic, and fluctuating nature of this disease. It is incumbent on health care professionals to reduce the burden of depression. The relationship between depression, anxiety disorders, and suicide attempts has been a subject of debate.20,21 Family dysfunction, as in the case of Mr A, is considered a critical factor for suicidal behavior among individuals in western societies.22,23
Problems within families or groups of individuals form a common, but unique, category of adjustment difficulty and serve as a critical factor for the development of depression and suicidal behavior among the western societies.22,23 Our case showed several of these factors leading to poor communication and self-discipline problems, separation, bereavement, and burden, which aggravated depressive episodes, caused angst, and led to suicide attempts.
Submitted: December 24, 2015; accepted
January 26, 2016.
Published online: June 30, 2016.
Potential conflicts of interest: None.
Funding/support: None.
REFERENCES
1. Liu CY, Wang SJ, Teng EL, et al. Depressive disorders among older residents in a Chinese rural community. Psychol Med. 1997;27(4):943–949. doi:10.1017/S0033291797005230 PubMed
2. Depression: a global public health concern. WHO Dep Ment Heal Subst Abus. 2012;1–8. WHO Web site. http://www.who.int/mental_health/management/depression/who_paper_depression_wfmh_2012.pdf?ua=1. Accessed February 9, 2016.
3. Dikmen SS, Bombardier CH, Machamer JE, et al. Natural history of depression in traumatic brain injury. Arch Phys Med Rehabil. 2004;85(9):1457–1464. doi:10.1016/j.apmr.2003.12.041 PubMed
4. Holsinger T, Steffens DC, Phillips C, et al. Head injury in early adulthood and the lifetime risk of depression. Arch Gen Psychiatry. 2002;59(1):17–22. doi:10.1001/archpsyc.59.1.17 PubMed
5. Hesdorffer DC, Rauch SL, Tamminga CA. Long-term psychiatric outcomes following traumatic brain injury: a review of the literature. J Head Trauma Rehabil. 2009;24(6):452–459. doi:10.1097/HTR.0b013e3181c133fd PubMed
6. Lozano R, Naghavi M, Foreman K, et al. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012;380(9859):2095–2128. doi:10.1016/S0140-6736(12)61728-0 PubMed
7. Park H, Lee B, Yoon C. Suicide by blunt head trauma: two cases with striking similarities. Forensic Sci Int. 2015;255:102–105. doi:10.1016/j.forsciint.2015.08.002 PubMed
8. Spiers AS. Attempted suicide or hitting the nail on the head. Case report. J Fla Med Assoc. 1994;81(12):822–823. PubMed
9. Portigliatti-Barbos M. Suicide by hammer blows. Minerva Medicoleg. 1952;72(3):79–81. PubMed
10. Borghesi R. On unusual methods of suicide: apropos of a case of attempted suicide by self-inflicted hammer blow on the head. Rass Studi Psichiatr. 1965;54(2):157–164. PubMed
11. Chang V, Hartzfeld P, Langlois M, et al. Outcomes of cranial repair after craniectomy. J Neurosurg. 2010;112(5):1120–1124. doi:10.3171/2009.6.JNS09133 PubMed
12. Dujovny M, Aviles A, Agner C, et al. Cranioplasty: cosmetic or therapeutic? Surg Neurol. 1997;47(3):238–241. doi:10.1016/S0090-3019(96)00013-4 PubMed
13. Yadla S, Campbell PG, Chitale R, et al. Effect of early surgery, material, and method of flap preservation on cranioplasty infections: a systematic review. Neurosurgery. 2011;68(4):1124–1129, discussion 1130. PubMed
14. Rogers GF, Greene AK. Autogenous bone graft: basic science and clinical implications. J Craniofac Surg. 2012;23(1):323–327. doi:10.1097/SCS.0b013e318241dcba PubMed
15. Huang Y-H, Yang T-M, Lee T-C, et al. Acute autologous bone flap infection after cranioplasty for postinjury decompressive craniectomy. Injury. 2013;44(1):44–47. doi:10.1016/j.injury.2011.11.005 PubMed
16. Piitulainen JM, Kauko T, Aitasalo KMJ, et al. Outcomes of cranioplasty with synthetic materials and autologous bone grafts. World Neurosurg. 2015;83(5):708–714. doi:10.1016/j.wneu.2015.01.014 PubMed
17. Drosos GI, Babourda E, Magnissalis EA, et al. Mechanical characterization of bone graft substitute ceramic cements. Injury. 2012;43(3):266–271. doi:10.1016/j.injury.2011.02.004 PubMed
18. Gladstone HB, McDermott MW, Cooke DD. Implants for cranioplasty. Otolaryngol Clin North Am. 1995;28(2):381–400. PubMed
19. Krishnan KG, Müller A, Hong B, et al. Complex wound-healing problems in neurosurgical patients: risk factors, grading and treatment strategy. Acta Neurochir (Wien). 2012;154(3):541–554. doi:10.1007/s00701-011-1221-0 PubMed
20. Vickers K, McNally RJ. Panic disorder and suicide attempt in the National Comorbidity Survey. J Abnorm Psychol. 2004;113(4):582–591. doi:10.1037/0021-843X.113.4.582 PubMed
21. Hornig CD, McNally RJ. Panic disorder and suicide attempt. A reanalysis of data from the Epidemiologic Catchment Area study. Br J Psychiatry. 1995;167(1):76–79. doi:10.1192/bjp.167.1.76 PubMed
22. McDermut W, Miller IW, Solomon D, et al. Family functioning and suicidality in depressed adults. Compr Psychiatry. 2001;42(2):96–104. doi:10.1053/comp.2001.21220 PubMed
23. Prinstein MJ, Boergers J, Spirito A, et al. Peer functioning, family dysfunction, and psychological symptoms in a risk factor model for adolescent inpatients’ suicidal ideation severity. J Clin Child Psychol. 2000;29(3):392–405. doi:10.1207/S15374424JCCP2903_10 PubMed
Enjoy this premium PDF as part of your membership benefits!


