Succinylcholine is a depolarizing neuromuscular blocker used for rapid sequence intubation and short-term paralysis in surgical and emergency settings.1 Outside such controlled environments, it can cause rapid respiratory arrest, hyperkalemia, and malignant hyperthermia, making its misuse potentially fatal, especially after repeated administration.2–4 Historically, nonmedical use of succinylcholine has been reported almost exclusively in forensic settings, like homicides, suicides, or covert poisonings, where its paralytic effects and postmortem detectability pose diagnostic challenges.5–8 There are no previously published reports, to our knowledge, of succinylcholine being intentionally self-administered for euphoria or more notably for nonsuicidal psychological relief, which is a pattern that has not been documented to date.
Case Report
We present the case of a 29-year old female health care worker with complex posttraumatic stress disorder (PTSD) and polysubstance dependence who engaged in repeated, nonsuicidal self-injection of succinylcholine over 18 months. Her behavior reflects a unique intersection of psychiatric vulnerability, occupational access, and unconventional substance misuse, a pattern that may go unrecognized in conventional clinical or addiction frameworks.
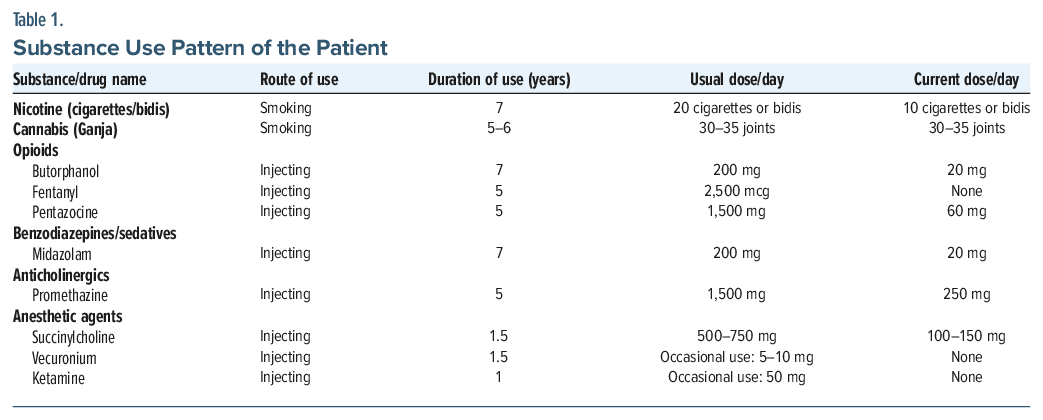
The patient had an 11-year history of polysubstance use beginning in late adolescence, including inhalants, intravenous butorphanol, pharmaceutical opioids, benzodiazepines, and cannabis. Her substance use was driven by persistent sleep disturbance, emotional dysregulation, and trauma. She disclosed a history of early life adversity, prolonged emotional abuse, and repeated nonconsensual sexual intercourse in her first marriage. Following separation and remarriage, she reported an aversion to physical intimacy with her second husband, reflecting persistent relational avoidance. Her sleep was markedly disturbed, characterized by autonomic arousal and frequent nightmares. A comprehensive psychiatric evaluation indicated complex PTSD, characterized by reexperiencing phenomena, emotional numbing, hypervigilance, and pervasive shame. Although she also displayed impulsivity and self-injurious behavior, she lacked core features of borderline personality disorder such as unstable interpersonal relationships or intense fears of abandonment.
The patient was working in an intensive care unit as a charge nurse and was routinely responsible for managing and procuring medication stocks. Her occupational responsibilities, along with established familiarity with local medical shops, allowed her to access opioids and other restricted medications without prescription. She reported primarily injecting pharmaceutical opioids obtained from these shops and only occasionally accessing medications from hospital supply. Approximately 18 months before admission, she mistakenly self-administered succinylcholine, having confused it with another injectable opioid. She recalled a wave of physical stillness, quietness, and emotional detachment within seconds. She described the experience as “deeply calming” and relieving her “constant mental unrest” and unlike any opioid or sedative. This singular episode triggered the beginning of her intentional use of succinylcholine, which she soon began administering daily.
She subsequently developed a pattern of injecting 1–2 mL (50 mg/mL) succinylcholine diluted in 50–100 mL normal saline, infused over 10–15 minutes, 5–7 times, amounting to 500–750 mg/d within 2–3 months of initiating the use, which was approximately 4 to 5 times the clinical dose. She reported that the “calming” effect of succinylcholine progressively shortened over time, prompting escalation in both dose and frequency. This pattern did not reflect classical craving or pharmacologic tolerance, but rather an overpowering, negative reinforcement–driven urge to reproduce the brief attenuation of her chronic internal unrest. She did not exhibit a physiological withdrawal syndrome, aside from a resurgence of psychological agitation when she attempted to stop. Nevertheless, several dependence-like features were evident, including persistent use despite repeated medical harm, occupational impairment, and preoccupation with obtaining the substance through inappropriate means. Despite experiencing 2 episodes of respiratory depression requiring assisted ventilation at her workplace, she continued use until a third near-fatal event that prompted the hospital to inform her husband, who then accompanied her to seek medical attention. At hospital admission, she presented with generalized weakness, giddiness, and multiple inflamed injection sites across the trunk and gluteal region. She was diagnosed with multiple substance dependence, harmful pattern of nonpsychoactive substances, and complex PTSD per International Classification of Diseases, Eleventh Revision criteria. Table 1 provides an overview of the patient’s substance use pattern.
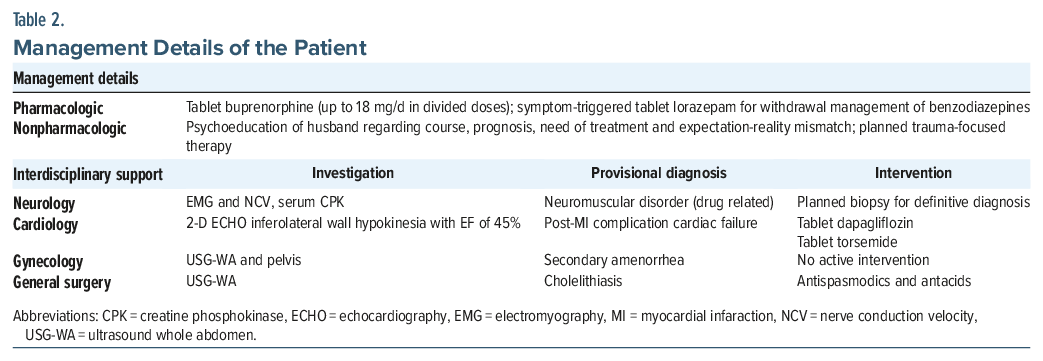
Treatment included inpatient opioid agonist therapy with buprenorphine, wound care, trauma-informed psychotherapy, and multidisciplinary support (Table 2). Although sertraline was planned for managing her complex PTSD, initiation was deferred due to her acute medical instability related to succinylcholine misuse and a prior episode of cardiac arrest. She requested discharge before pharmacotherapy could be started and subsequently showed inconsistent engagement with follow-up services. She remained abstinent from opioids and succinylcholine for several months postdischarge, though a possible relapse was later reported by her husband.
Discussion
This case is noteworthy for several reasons. It is the first documented report of nonsuicidal, intentional misuse of succinylcholine, a high-risk neuromuscular blocker not known for psychoactive properties. The drug-seeking behavior in this case was not euphoria but perceived psychological calmness likely tied to transient hypoxia and hypercarbia from respiratory muscle paralysis.9 The very short duration of succinylcholine action, combined with slow infusion, may have offered some protection against fatal respiratory arrest in this case. This case underscores the clinical blind spot in recognizing misuse of nonpsychoactive substances, especially in trauma-exposed individuals with complex psychiatric comorbidities and illustrates how occupational access to restricted medications can facilitate high-risk experimentation among health care personnel.
Clinicians must maintain a high index of suspicion for unconventional misuse patterns in individuals with trauma and occupational access. At a systems level, the case highlights the need for secure medication storage protocols and monitoring of high-risk drug inventories in health care environments. Forensic surveillance data from China have reported succinylcholine in animal poisonings and syringe dart attacks, further validating the need for regulation beyond clinical use.10
In conclusion, we present the first reported case of intentional nonsuicidal succinylcholine misuse for psychological relief in a health care professional with complex PTSD. This unusual and dangerous pattern of misuse expands our clinical understanding of how trauma and occupational access intersect to produce novel substance use behaviors.
Article Information
Published Online: April 7, 2026. https://doi.org/10.4088/PCC.25cr04075
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04075
Submitted: September 8, 2025; accepted November 26, 2025.
To Cite: Patel V, Kaur G, Mandal P, et al. Intentional nonsuicidal succinylcholine use in a health care worker with complex posttraumatic stress disorder. Prim Care Companion CNS Disord 2026;28(2):25cr04075.
Author Affiliations: National Drug Dependence Treatment Centre, All India Institute of Medical Sciences, New Delhi, India (Patel, Kaur, Mandal, Agrawal, Dayal, Ambekar); Department of Psychiatry, All India Institute of Medical Sciences, Tatibandh, Raipur, India (Patel); Department of Anesthesia, All India Institute of Medical Sciences, New Delhi, India (Baidya); Department of Anesthesia, All India Institute of Medical Sciences, Guwahati, Assam, India (Baidya).
Corresponding Author: Piyali Mandal, MD, National Drug Dependence Treatment Centre, 4th Floor, Teaching block, Ansari Nagar, New Delhi, India, Pin 110029 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Informed consent was obtained from the patient to publish this case report, and information has been de-identified to protect anonymity.
Acknowledgments: The authors acknowledge the contributions of the hospital clinical team in managing the patient and facilitating multidisciplinary care.
References (10)

- Cass NM, Brace GR. Repeated doses of suxamethonium. Anaesth Intensive Care. 1980;8(3):345–348. PubMed CrossRef
- Barrons RW, Nguyen LT. Succinylcholine-Induced rhabdomyolysis in adults: case report and review of the literature. J Pharm Pract. 2020;33(1):102–107. PubMed CrossRef
- Chekol B, Zurbachew N, Mekete G, et al. Prevalence and associated factors of postoperative suxamethonium-induced myalgia in surgical patients at Debre Tabor Comprehensive Specialized Hospital Ethiopia: a cross-sectional study. Sci Rep. 2024;14(1):16552. PubMed CrossRef
- Hager HH, Patel P, Burns B. Succinylcholine chloride. In: StatPearls. StatPearls Publishing; 2025. Accessed April 28, 2025. http://www.ncbi.nlm.nih.gov/books/ NBK499984/
- Furbee RB. Criminal poisoning: medical murderers. Clin Lab Med. 2006;26(1):255–273. PubMed CrossRef
- Johnstone RE, Katz RL, Stanley TH. Homicides using muscle relaxants, opioids, and anesthetic drugs: anesthesiologist assistance in their investigation and prosecution. Anesthesiology. 2011;114(3):713–716. PubMed CrossRef
- Zhao YF, Zhao BQ, Ma KJ, et al. Forensic analysis for 54 cases of suxamethonium chloride poisoning. Fa Yi Xue Za Zhi. 2017;33(4):374–375. PubMed CrossRef
- Kunhahamed MO, Thomas VK, Abraham SV, et al. Survival following intentional succinylcholine injection for self-harm. Turk J Emerg Med. 2020;20(4):193–195. PubMed CrossRef
- Drechsler M, Morris J. Carbon dioxide narcosis. In: StatPearls. StatPearls Publishing; 2025. Accessed April 30, 2025. http://www.ncbi.nlm.nih.gov/books/ NBK551620/
- Wang X, Xiang P, Zhang S, et al. Retrospective analysis of forensic toxicology data from 2021 to identify patterns of various forensic cases. Forensic Sci Int. 2023;347:111683. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





