Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(1):25f04100
Author affiliations are listed at the end of this article.
Have you ever wondered whether you have experienced a psychological or spiritual crisis that resulted from your engagement in clinical care? Have you been uncertain about why your experience was called moral injury rather than anger, confusion, or depression? Have you puzzled over what your best response could have been to mitigate your distress and enhance your resilience? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Dr A, a 50-year-old primary care physician, presented with increasingly severe despair and a loss of professional fulfillment. Over the past several years, she has encountered repeated situations in which systemic and institutional constraints forced her to act against her ethical standards. She described being required to prescribe medications that she believed were unnecessary, to discharge medically fragile patients earlier than she believed was safe, and to not pursue authorizations (because of insurance restrictions) for diagnostic tests that she considered clinically indicated. Although she denied having intrusive recollections or hyperarousal typical of posttraumatic stress disorder (PTSD), she was preoccupied by guilt over these decisions and felt haunted by a persistent sense of moral failure. She withdrew from her colleagues, whom she felt could not understand her situation, and increasingly described herself as “a doctor I don’t respect anymore.” Despite trials of standard treatments for depression, she continued to feel shame, alienation, and the erosion of meaning that had defined her professional life.
DISCUSSION
What Is Moral Injury?
Moral injury is a term that captures manifestations of traumatic distress that are distinct from other trauma-related syndromes (eg, PTSD). Building upon social-cognitive theories of PTSD, the concept of moral injury was introduced in 2009 to recognize the experience of military veterans who did not meet criteria for fear-based criterion A of PTSD yet struggled with negative repercussions of dysregulated mood and thoughts (eg, guilt, shame, and feelings of betrayal). Despite the overlap in criteria for moral injury and PTSD, they rest upon separate constructs.1,2 Moral injury involves a transgression (either perpetrated, witnessed, or experienced in an act of betrayal) that violates deeply held assumptions and beliefs about right, wrong, and personal goodness.3 While moral injury is not a mental disorder, the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR) approved the expansion of the Z-code “Religious, or Spiritual Problem” to include “moral problems,” largely to recognize the role that disruptions to one’s moral identity play in struggles with mental illness.4,5
Moral injury develops when this transgressive experience, or cumulative set of experiences (as in cases of moral distress), results in the disruption of one’s moral identity and leads to a variety of morally laden emotions (eg, shame, feelings of betrayal, and disgust).6–8 Morally unjustified acts committed by an individual, or that an individual did not do but failed to prevent, often result in guilt and shame because of the dissonance between the person’s values and their behavior. Conversely, acts that are witnessed or experienced as a victim (eg, in situations of betrayal) often lead to anger and disgust. Analogous to cognitive dissonance, in which individuals encounter an idea that runs contrary to their previously held beliefs, moral injury is a form of “moral dissonance,” in which a person is confronted by a situation that challenges, transgresses, or contradicts their previously held moral values and expectations.
Moral injury has deep historical roots. The term miasma in ancient Greece referred to a soldier’s experience of “moral defilement or pollution, often resulting from unjust killing, but applicable to any transgression of moral values.”9 In modern times, Shay, a Boston psychiatrist who specialized in the treatment of veterans with PTSD, recognized that PTSD failed to account for the profound guilt, shame, and feelings of betrayal experienced by veterans of the Vietnam War.10 By comparing their experiences with those of Achilles in Homer’s Iliad, Shay helped to elevate these wounds beyond the realm of clinical symptoms and into the realm of tragic, ancient, and deeply human emotions. He argued that moral injury revolves around the shattering of trust, meaning, and moral identity and that healing requires truth-telling, communal recognition, and moral repair—not just medication or cognitive restructuring.
Running parallel to the insights of clinicians who treat treatment-refractory PTSD in Vietnam veterans, health care professionals recognized moral wounds in their own profession, captured as “moral distress,” which arose from engaging in often routine clinical care.11 Jameton12 observed neonatal intensive care unit nurses in medically futile situations as they performed daily and often painful interventions on infants with extremely poor prognoses. In most of those cases, parents and physicians decided to remove supportive care and allow the infant to die. However, when parents who did not fully accept the situation urged physicians to pursue therapy aggressively, nurses were caught in the middle, performing care that went against what they felt was right. Jameton went on to say, “in situations such as these, nurses report feeling distress. Nurses feel frustrated, angry, and guilty. They feel that they have some moral responsibility for the care being provided, but feel powerless to change the course of therapy.”12(p543) Jameton highlighted the role that external constraints play in impeding the perceived best possible care for patients, which leads to moral distress.12
While the concept of moral distress was first described in health care settings and moral injury was described among veterans, these constructs later converged under the constraints of the COVID-19 pandemic. High-stakes ethical situations (eg, the need to decide who would receive life-saving care in resource-limited settings) led to moral distress that labels such as “burnout” failed to capture.13 Moral injury subsequently became recognized as increasingly prevalent and responsible for myriad adverse occupational sequelae, including workplace attrition and suicide. Dean, a psychiatrist and thought leader on moral injury in health care workers, reflected “There are a lot of roads that lead to burnout, but the highway is moral injury.”14
The parallels between moral injury in health care and military settings reveal the ubiquitous nature of these experiences and highlight the role that moral values play in the pursuit of one’s occupation. For example, the military sociocultural context imbues individuals with a warrior ethos and a commitment to serve, while fostering strong interdependent bonds among members.15 This unique context shapes the commitments that are integral to a soldier’s moral identity, which are often transgressed in the pursuit of their occupation. As is seen in military settings, the health care training environment fosters altruism, self-sacrifice, and high levels of occupational dedication; these individuals enter their professions anticipating that they will protect, serve, and administer resources to those under their care. Instead, they may encounter situations in which their values can be challenged or contradicted, such as in the accidental killing of civilians in war, or the administration of limited resources in a way that leads to adverse outcomes, which can result in guilt, shame, feelings of betrayal, and anger.
How Is Moral Injury Recognized in Clinical Settings?
Distinguishing between PTSD and moral injury, or recognizing their co-occurrence, can be challenging. This is largely due to the strong association between specific PTSD symptom clusters and measures of moral injury (eg, guilt/shame, hopelessness, and loss of meaning).16 This overlap of symptoms’ characteristic of moral injury and PTSD is most notable in the affective (cluster D) domain of PTSD symptoms.17 The major difference between them is that PTSD does not necessarily involve guilt and shame, and when guilt and shame are involved in PTSD, they can be due to exaggerated beliefs that go beyond a reasonable interpretation of the events (Table 1).
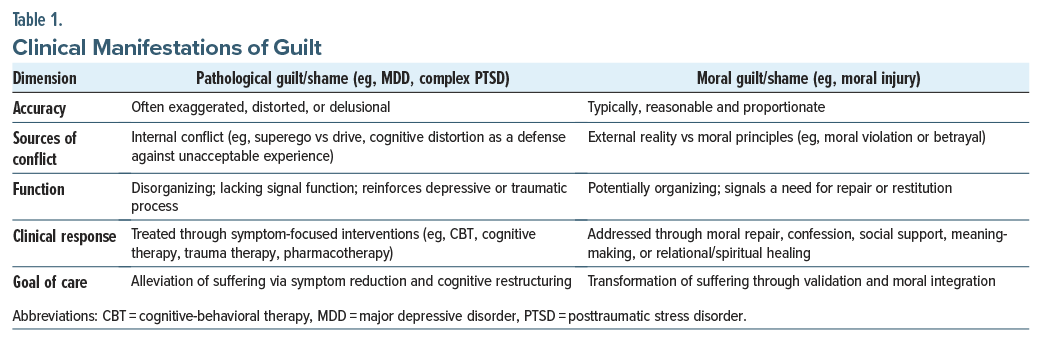
Clinicians must distinguish between pathological guilt and shame, states that are common in several disorders (eg, major depressive disorder [MDD], some cases of PTSD, or neurotic conflict) and morally appropriate guilt, as is seen in some phenomena, such as moral injury. Pathological guilt is often related to excessive, distorted, or globalized beliefs that are driven by cognitive distortions that have been acquired or reinforced during fight, flight, or freeze states. These distorted cognitions sometimes spread into a negative appraisal of the self, which can be manifest as shame.
In contrast to pathological guilt or shame, moral injury is an appropriate and expected response that arises from perceived moral transgressions or betrayals—whether committed, witnessed, or involving the failure to prevent—often under conditions of constraint or duress.18 In these cases, guilt is not a symptom to be reappraised as a cognitive distortion, but a signal that reflects a functioning conscience in the context of a broken or inhumane environment. Shame, when present, is not the result of traumatic conditioning, but a deeply felt sense of a lack of belonging and safety due to moral harms committed by the individual or by trusted others. Treatment should match the emotions’ etiology: cognitive or trauma-based interventions for pathological guilt and relational, narrative, or amend-making approaches for morally grounded guilt.19 The distinction is important for practicing clinicians because using cognitive restructuring techniques that are intended to be used with pathological guilt and shame in individuals with moral injury risks pathologizing and invalidating the moral insight of individuals who can be allies in healing and repair. The same could be said for feelings of anger, betrayal, and disgust, which are relational moral emotions that, in the context of a moral injury, require acknowledgement, validation, and subsequent repair (see Treatments section below).20
Research further demonstrates key distinctions between moral injury and PTSD, which highlight the clinical relevance of addressing both problems in clinical care. One study found that moral injury accounts for an increase in thoughts of, and attempts at, suicide independent of PTSD symptom severity.16 Litz et al21 found that specific types of morally injurious events (eg, perpetration-based) are associated with higher levels of guilt and self-blame compared to traditional life-threatening traumas that classically caused PTSD. Bryan and colleagues17 surveyed National Guard personnel and found that PTSD was uniquely characterized by hyperarousal, memory loss, and self-reported flashbacks, whereas moral injury was characterized by guilt, shame, anhedonia, and social alienation.
Beyond the core emotional and cognitive sequelae of moral injury, additional behavioral and functional sequelae can follow when moral injury is persistent and severe. In a review of 49 studies involving more than 23,000 participants in multiple populations (including active military, veterans, health care workers, refugees, educators, undergraduate students, and other public safety personnel), a variety of associations emerged among moral injury–related constructs and PTSD, depression, anxiety, and self-harm/suicidal behavior.22 The relationship between substance use and moral injury has also been suggested by several studies.23,24 Studies of military personnel have shown positive associations between moral injury and numerous adverse mental health outcomes, including severe PTSD symptoms and the risk of suicide.25 Moreover, in health care workers, moral injury and moral distress are associated with symptoms of burnout (eg, depersonalization and emotional exhaustion) and increased medical errors.26,27
What Are the Implications of Moral Injuries?
Although evidence supporting the proposal for a Z code for moral problems came largely from literature that described moral injury and distress, several clinical scenarios illustrate the relevance of threats to one’s “sense of goodness of the self, others or institutions.”8 Medical mistrust, often marked by a loss of faith in goodness, prompts clinicians to restore trust by conveying integrity and concern as part of a trauma-informed approach, invoking principles of safety, trustworthiness, choice, collaboration, and empowerment.28 In a similar fashion, treatment of the demoralized and suicidal patient often requires caregivers to lend the patient hope in goodness. Frank29 as well as Viederman and Perry30 emphasized the importance of hope in psychotherapy. “Viederman and Perry wrote narrative by its very nature conveys to the patient that he is worth understanding and by implication is therefore worthy.”30(p138) As Shay10 and Alford31 expressed, demoralized individuals may experience existential despair about injustice.
Depression may unearth or provoke struggles with one’s moral identity. Negative moral emotions (eg, guilt, shame, contempt/disgust, and regret) are common in depression, and DSM-5 core symptoms of MDD include feelings of worthlessness or excessive or inappropriate guilt nearly every day. On the other hand, realistic or “true” guilt can also lead to depressed mood, for example, as a contributing factor to suicide risk following incarceration. In the context of trauma, individuals who have been subjected to coercion and abuse may internalize shame and guilt in ways that increase their vulnerability to depression. Relatedly, complex PTSD can contribute to depression. In a study of 240 psychiatric inpatients, Bekes and coworkers32 found that the impact of childhood trauma on present borderline personality disorder, PTSD, and disturbances in self-organization was mediated by moral injury and shame. At the same time, depression can be an occasion for moral reassessment, improved insight, and growth.33
Personality disorders marked by narcissism and psychopathy differ from other moral problems in that they typically cause others more distress, reflecting stunted conceptions of goodness and a lack of empathy and compassion among other prosocial virtues. Finally, literature on moral dilemmas in various settings documents associations among anxiety, depression, and burnout. Patients may present for treatment with distressing indecision about questions that have a prominent moral component, eg, whether it is right to divorce, whether one should sacrifice for an aging parent, or whether one should forgive a childhood abuser.
Who Is at Risk for Moral Injury (and Why)?
Veterans, health care workers, and other civilian populations such as refugees and displaced persons are among those most at risk for moral injury. Among veterans who have been deployed, moral injury can result from a mismatch between the warriors’ expectations and experiences of engagement. Some warriors go to war expecting they will assist the people in the country they occupy. However, they may have been confronted with militants who used women and children as shields and may have had to shoot at targets knowing there were innocent (noncombatant) women and children there. Or, they may have had to kill children who were shooting at their unit. They may feel betrayed when Iraqi or Afghani collaborators, whom they trusted, detonated an improvised explosive device that injured them or other warriors. Alternatively, they may feel guilty when local collaborators, such as interpreters, were imprisoned or killed despite their promise to protect them. Experiences such as these can create moral dissonance between warriors’ expectations and their experience. This moral dissonance can become palpable when the warrior returns home and engages in civilian life with its clear moral code (eg, do not harm innocent civilians, women, and children). The warrior has difficulty integrating his experience and sense of self at war and in civilian life. This disconnect makes it difficult for warriors to share their experience with civilians—such as family members, a spouse, or their children—and to maintain a bond with other veterans. Sometimes, warriors feel “different,” “bad,” or “evil” and deny that part of their self that was there during the war. Frequently, veterans take responsibility for their actions but have difficulty understanding the factors that influence their behavior in the broader context of politics, war, and circumstances of their unit.
Moral injury among veterans who had been deployed can be associated with the severity of emotional distress, recent mental health service use, pain, disordered sleep, fear of death, use of alcohol/drugs to cope postdeployment, and poor unit support/morale during deployment. Deployed veterans with moral injury are more likely to have current mental health disorders and other psychological problems, even years after their deployment.34 Conversely, more severe levels of trauma and the presence of moral injury may lead to higher posttraumatic growth. Thus, the presence of each of the following factors (adverse childhood events, traumatic events during military service, moral injury, and PTSD) contributed to greater self-reported posttraumatic growth in a survey of 5,245 post-9/11 veterans.35 Medical-surgical personnel deployed in war zones frequently experience moral injury related to witnessing horrific injuries; treating pregnant women, children, and US soldiers; having limited capabilities and resources; being inexperienced in performing specialty surgical procedures; second-guessing decisions; and communicating with those in command. These moral injuries result in postdeployment manifestations, eg, disordered sleep, impaired medical practice, and disrupted interpersonal relationships.36
Military sexual trauma (MST) is another cause of moral injury. The Veterans Health Administration uses the term MST to refer to experiences of sexual assault and/or sexual harassment that occurs during military service.37 Specifically, 38 U.S. Code §1720D defines MST as “physical assault of a sexual nature, battery of a sexual nature, or sexual harassment (unsolicited verbal or physical contact of a sexual nature which is threatening in character) that occurred while the former member of the Armed Forces was serving on duty, regardless of duty status or line of duty determination.”38 MST is estimated to occur in approximately 1 in 3 female and 1 in 50 male veterans.37 However, its prevalence is likely higher due to underreporting.39,40 MST is associated with significant, and frequently chronic, mental health consequences, such as PTSD, depression, substance use, insomnia, suicidal ideation and suicide attempts,41–44 and eating disorders.45,46 However, MST is traumatizing beyond the presence of clinical symptoms. Because it occurs within the highly organized, formal, and patriarchal structure of the military, MST shatters the victim’s sense of trust in their unit and sometimes the military and can lead to the loss of their professional and personal identity.47,48 Witnesses of MST may be incentivized not to report what they observed, and their sense of morality may also be injured.
Although moral injury was recognized by health care professionals as a source of occupational distress before the advent of the COVID-19 pandemic, moral injury’s prominence expanded exponentially given COVID-19’s global impact.49 The COVID-19 pandemic intensified mental health challenges for patients, families, communities, and health care workers, particularly among intensive care unit staff (eg, nurses, physicians, respiratory therapists, and environmental service workers). Health care professionals faced severe physical and emotional burdens due to often overwhelming numbers of patients, staffing shortages, limited resources (eg, personal protective equipment and ventilators), visitor restrictions, contact precautions, and high mortality rates. Nearly half of all health care workers lost trust in their leadership during the pandemic, describing a deep sense of betrayal that reflected moral injury.50 The pandemic exacerbated the vulnerabilities of health care systems that resulted in burnout, moral injury, grief, depression, and PTSD as health care workers were tasked with providing care for patients who were isolated from family support and then perished. Their moral injury stemmed from their perceived inability to provide adequate care and to prevent death, despite their best efforts.
The psychological toll on health care workers during the pandemic revealed dramatically elevated rates of burnout, anxiety, depression, and moral distress. More than 60% of health care workers reported symptoms of burnout during the pandemic, with nurses being disproportionately affected due to the intense emotional and physical demands required to provide patient care.51 Public health service officers and other frontline first responders, who often operated outside of traditional clinical and hospital environments, were also exposed to suffering, complex ethical dilemmas, and death, which contributed to moral injuries during the COVID-19 pandemic.52
While health care workers may experience moral injury in the context of resource scarcity, triage dilemmas, or perceived institutional betrayals, they are not unique in facing vulnerability. Moral injury is no longer limited to military service members and veterans; it now encompasses health care workers and a wide range of civilians, including those who have been forcibly displaced. Displaced persons (in areas affected by conflict, mass violence, natural disasters, and humanitarian crises) often face repeated exposure to events that challenge or violate deeply held moral beliefs.53 Addressing moral injuries in these populations requires moving beyond providing trauma-informed care to include interventions that recognize moral distress, pain, isolation, and betrayal.53
Across all populations, a unique factor relevant to those at risk for moral injury is spirituality and religiosity. Research suggests that individuals who are religious/spiritual and those who are not both have moral injury, although to various degrees and in different languages aligning with their respective worldviews.54 Regarding treatment for those who identify as religious or spiritual, spiritually oriented cognitive processing therapy has been applied in the treatment of moral injury.55 Evidence is lacking regarding the contributions of differing religious traditions (although major faith traditions all contain both moral expectations and resources for dealing with moral failure).56 With regard to the spirituality of the clinician, while unrelated to moral injury, spiritually integrated cognitive-behavioral therapy (CBT) was found to be as effective delivered by nonreligious as by religious therapists, suggesting that therapeutic mechanisms may be effective regardless of the clinician’s specific worldview.57
How Should Clinicians Respond When Patients Disclose Moral Injury?
When patients describe symptoms that are consistent with moral injury, psychoeducation helps to frame the next steps of healing. Rather than avoiding discussion of, or focusing on, the emotional sequelae of an experience, clinicians can validate a patient’s moral concerns. Herman,58 in Truth and Repair, highlighted the need of trauma survivors to have their concerns acknowledged and vindicated. Validation of a patient’s distress involves providing a language for the experience, recognizing its distinction from other psychiatric conditions, eg, PTSD and depression, as well as recognizing the perpetration-related and relational-violation-related subtypes of moral injury (although these may be comorbid). This allows for exploration with the patient of the nature of their suffering so that it can be addressed. While evidence-based treatments for moral injury are lacking, several individual and group therapy approaches may be useful. There is likely utility in clinicians being an initial change agent even in early patient-clinician encounters, allowing for interpersonal and moral reconnection that forms from establishing a safe connection.
Clinicians can also address the psychological and moral dimensions of a patient’s experience. For example, Barr and associates1 advocated for a “dual approach” that addressed the dysregulation of the fear and memory systems, as well as disturbances in value and character, eg, “through reflection, self-forgiveness, repentance, and restoration.”1 Similarly, Litz20 argued for a “Yes, . . . and” rather than a “Yes, . . . but” approach, that goes beyond traditional behavioral approaches, eg, CBT, which assumes a normally operating conscience and addresses distorted beliefs that are associated with guilt and shame.
In addition, clinicians can help patients access resources for dealing with moral failure or demoralization, eg, by engaging the patient’s core values, the spiritual basis of their ideals, the virtues upheld by their traditions, and prosocial experiences and attachments (eg, mindfulness and other spiritual practices).59 Clinicians can also help individuals who struggle with guilt to explore options for forgiveness, by themselves and others, but without serving as moral arbiters or secular priests. For example, most proposed treatments of moral injury suggest that moral emotions, such as guilt related to actions a soldier perpetrated during deployment, can serve as a signal of an underlying value that was lost or transgressed. In helping patients move forward, clinicians can help to clarify the values that were lost and to orient the patient toward a life of meaning in accordance with those values. The guilt may signal an underlying value to protect the vulnerable; the clinician can help to clarify this through nonjudgmental exploration, allowing the patient to choose to live according to that value in a newly integrated way going forward.
What Are the Treatments for Moral Injury?
Several psychotherapeutic treatments adapt or incorporate CBT approaches. Spiritually Integrated Cognitive Processing Therapy (SICPT), developed by Pearce and colleagues,60 has been shown effective in reducing symptoms of moral injury and PTSD, particularly when spiritual distress is prominent. Acceptance and Commitment Therapy for Moral Injury (ACT-MI), described by Borges and colleagues,61 targets avoidance and control behaviors that can perpetuate moral injury–related suffering, pursuing valued action despite ongoing moral pain. Value-based CBT integrates elements of ACT, spiritual care, and adaptive disclosure, while targeting shame-based maladaptive coping behaviors in military populations, by emphasizing self-compassion, forgiveness, and reconnection with personal values and social networks.62 The modified Adaptive Disclosure-Enhance (AD-E) therapy recognizes that personalized treatment plans are needed for different types of trauma. AD-E includes letter-writing, compassion training, and homework that promotes recovery or reinforcement of social networks.63 Narrative-based therapies, such as the 6-Fold Path to Self-Forgiveness (6-FPSF), have also shown promise.64
As far as course of illness and subsequent treatment targets when MI and PTSD co-occur, there are no empirical longitudinal studies, to our knowledge, that demonstrate how they coevolve. While there are theoretical models, which we cite,1 as well as anecdotal clinical evidence suggesting that moral injury is more durable and remains after fear-based mechanisms are extinguished through prolonged exposure or cognitive processing therapy, the empirical evidence for this is lacking. For treatment, sequence is likely best personalized based on the severity of presenting symptoms. Fear-based sequelae of PTSD may be a barrier to processing guilt/shame from moral injury; however, guilt/shame may also prevent engagement in appropriate care for PTSD in other cases.
Beyond psychotherapeutic approaches, evidence is steadily accumulating for psychedelic-assisted treatments—that is, the clinical administration of psychedelics within a short course of psychotherapeutic support—to treat a range of conditions that are adjacent to, or frequently comorbid with, moral injury. These include PTSD,65 anxiety,66 depression,67 grief,68 alcohol use,69 and demoralization in the setting of chronic medical illness.70 Importantly, preliminary work has also examined psychedelic use in populations at high risk for moral injury, such as frontline health care workers suffering from pandemic-related depression and veterans and first responders.71–73 While the US Food and Drug Administration declined to approve the first new drug application for a psychedelic drug in 2024, several late-phase clinical trials are currently underway.74
Psychedelic therapies have shown promise in addressing several psychological and emotional states central to MI, including painful emotions that are difficult to approach directly, such as shame and guilt as well as existential distress.75,76 MDMA, for example, is known for enhancing feelings of empathy and trust that allows patients to revisit, process, and integrate difficult feelings with openness and honesty. Classic psychedelics, such as psilocybin, have been linked to greater self-compassion, acceptance, and shifts in negative narratives, all of which are relevant for recovery in MI.76 Mechanistically, moral injury and neural targets of psychedelics share overlaps; MI has been associated with alterations in brain networks associated with self-referential processing, such as the default mode network, that is also implicated in the therapeutic actions of psychedelics.77,78 One recent study of MI found pathological activity in key regions of the default mode network, with this activity also correlated with rumination—the clinical correlate of aberrant self-referential processing.79 Psychedelics are known to disrupt the default mode network, thereby altering self-referential processing and shifting previously deeply held belief patterns via interfering with high-level priors.80 Together, these mechanisms suggest psychedelics hold promise in targeting key psychological and neurobiological signatures of MI.
How Should Clinicians Respond to Their Own Moral Distress/Injuries in the Context of Providing Clinical Care?
While most studies of moral injury have been conducted in military personnel, several feasibility trials have focused on health care clinicians in the context of the COVID-19 pandemic.64,81 The same general approach can be applied to a clinician’s response to their own, or to a colleague’s, experience of moral injury, while distinguishing it from moral frustration and moral distress.59 This involves acknowledging its reality, working with its existential frame, appreciating spiritual and psychological dimensions, and engaging much-needed resources, which may include formal or informal discussion of the issues with coworkers. What is needed varies to some degree on whether their experience comes from being a victim, a witness, or the person responsible for the injury. SICPT and ACT-MI may be helpful depending on the individual and the circumstances of injury; 6-FPSF was developed specifically for health care clinicians.
Moral injury that is characterized more by loss of trust than guilt can arise when the injury occurs as a function of institutional policies, programs, or resource limitations that are outside the purview or control of the individual clinician at the bedside. In this context, an institutional response may be required as part of the process to re-establish trust. As institutions create spaces of vulnerability, clinicians will feel empowered to seek help themselves. This may take the form of support from a colleague or from initiating in regular therapy to process the unique moral strains of working in health care.
Trauma-informed principles (including transparency, collaboration, empowerment, and peer support) may help frame the discussion. Psychological safety can be modeled and promoted by supervisors, departmental leadership, case conferences, risk management teams, and peers. Each of these workplace elements can serve as a forum for disclosing, learning, processing, reinforcing broader skills and competencies; identifying avenues for advocacy as a change-agent; retaining a sense of belonging and self-compassion; and generating and implementing a response plan, when indicated.
What Happened to Dr A?
Dr A’s presentation was correctly diagnosed as moral injury, critically distinguished from either depression or PTSD. Her treatment focused on supportive psychotherapy and efforts to re-establish meaning in her professional life. While she achieved some relief, she eventually left her decades-long medical primary care practice in the face of ongoing, systemic pressures co-occurring with her hospital’s merger. She now works in a concierge practice with improved symptoms but continues to struggle with some guilt over her decision, as she misses caring for the underserved patients that she had originally entered medical school to treat. Her case illustrates the limitations of current approaches and underscores the need for innovative therapies that can target the shame, guilt, and self-alienation at the heart of moral injury.
CONCLUSION
Moral injury was introduced into the literature to recognize the experience of military veterans who did not meet criteria for fear-based criterion A for PTSD yet struggled with negative repercussions of dysregulated mood and thoughts (eg, guilt, shame, and feelings of betrayal). Moreover, moral injury is a form of “moral dissonance,” in which a person is confronted by a situation that challenges, transgresses, or contradicts their previously held moral values and expectations. The parallels between moral injury in health care and military settings reveal the ubiquitous nature of these experiences and highlights the role that moral values play in the pursuit of one’s occupation. Moral injury is an appropriate and expected response that arises from perceived moral transgressions or betrayals—whether committed, witnessed, or involved the failure to prevent—often under conditions of constraint or duress. MST is another source of moral injury; it is associated with significant, and frequently chronic, mental health consequences (eg, PTSD, depression, substance use, suicide attempts). Medical-surgical personnel deployed in war zones frequently experience moral injury related to witnessing horrific injuries. These moral injuries result in postdeployment manifestations (eg, disordered sleep, impaired medical practices, and disrupted interpersonal relationships). Rather than avoiding discussion of, or focusing on, the emotional sequelae of an experience, clinicians can validate a patient’s moral concerns.
Article Information
Published Online: February 26, 2026. https://doi.org/10.4088/PCC.25f04100
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 3, 2025; accepted November 25, 2025.
To Cite: Mattson SA, King F, Tanev KS, et al. Moral injury: appreciating its impact and managing its sequelae. Prim Care Companion CNS Disord 2026;28(1):25f04100.
Author Affiliations: Department of Psychiatry, Massachusetts General/McLean Hospital, Boston, Massachusetts (Mattson, Matta, Stern); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (King, Tanev, Matta, Levy-Carrick, Peteet, Stern); Center for Neuroscience of Psychedelics, Massachusetts General Hospital, Boston, Massachusetts (King); The Home Base Program, Boston, Massachusetts (Tanev); MGH TBI Clinical and Research Program, Massachusetts General Hospital, Boston, Massachusetts (Tanev); Department of Psychiatry, Mass General Brigham AMC, Boston, Massachusetts (Levy-Carrick); Psychosocial Oncology Fellowship Site Director, Dana-Farber Cancer Institute and Brigham and Women’s Hospital, Boston, Massachusetts (Peteet).
Mattson, King, Tanev, Matta, and Levy-Carrick are co-first authors; Peteet and Stern are co-senior authors.
Corresponding Author: Seth A. Mattson, MD, Department of Psychiatry, Massachusetts General/McLean Hospital, Boston, Massachusetts ([email protected]).
Financial Disclosure: Dr King holds personal stock in Cybin and Compass, serves as a scientific advisor to Apex Labs, and receives research support from Tryp Therapeutics, the Tiny Blue Dot Foundation, and the David Borsook Project. Dr Stern has received royalties from Elsevier for editing textbooks on psychiatry. Drs Mattson, Matta, Tanev, Levy-Carrick, and Peteet have no disclosures or conflicts of interest.
Funding/Support: None.
Clinical Points
- Moral injury involves a transgression (either perpetrated, witnessed, or experienced in an act of betrayal) that violates deeply held assumptions and beliefs about right, wrong, and personal goodness.
- The major difference between moral injury and posttraumatic stress disorder (PTSD) is that PTSD does not necessarily involve guilt and shame; when guilt and shame are involved in PTSD, they can be due to exaggerated beliefs that go beyond a reasonable interpretation of the events.
- Healing of moral injuries requires truth-telling, communal recognition, and moral repair—not just medication or cognitive restructuring.
- Trauma-informed principles (including transparency, collaboration, empowerment, and peer support) help to frame discussions, while psychological safety can be modeled and promoted by supervisors, departmental leadership, case conferences, risk management teams, and peers.
References (81)

- Barr N, Atuel H, Saba S, et al. Toward a dual process model of moral injury and traumatic illness. Front Psychiatry. 2022;13:883338. PubMed CrossRef
- Griffin BJ, Purcell N, Burkman K, et al. Moral injury: an integrative review. J Traumatic Stress. 2019;32(3):350–362. PubMed CrossRef
- Litz BT, Stein N, Delaney E, et al. Moral injury and moral repair in war veterans: a preliminary model and intervention strategy. Clin Psychol Rev. 2009;29(8):695–706. PubMed CrossRef
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision (DSM-5-TR). American Psychiatric Association Publishing; 2022.
- American Psychiatric Association. Supplement to Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision. American Psychiatric Association Publishing; 2025. Accessed May 9, 2025. https://www.psychiatry.org/getmedia/b68a5776-f88c-45c7-9535-fd219d7aa5cb/APA-DSM5TR-Update-September-2025.pdf
- Farnsworth JK, Drescher KD, Nieuwsma JA, et al. The role of moral emotions in military trauma: implications for the study and treatment of moral injury. Rev Gen Psychol. 2014;18(4):249–262. CrossRef
- Vanderweele TJ, Wortham JS, Carey LB, et al. Moral trauma, moral distress, moral injury, and moral injury disorder: definitions and assessments. Front Psychol. 2025;16:1422441. PubMed CrossRef
- Mattson S, VanderWeele TJ, Lu F, et al. Moral, religious, or spiritual problem: an expanded Z code diagnostic category in the DSM-5-TR. J Nerv Ment Dis. 2025;213(11):297–304.
- Koenig HG, Al Zaben F. Moral injury: an increasingly recognized and widespread syndrome. J Religion Health. 2021;60(5):2989–3011. CrossRef
- Shay J. A. In: Achilles in Vietnam: Combat Trauma and the Undoing of Character. Athanaeum Books; 1994.
- Jameton A. Nursing Practice: The Ethical Issues. Prentice-Hall Inc; 1984.
- Jameton A. Dilemmas of moral distress: moral responsibility and nursing practice. AWHONN’s Clin Issues Perinat Women’s Health Nurs. 1993;4(4):542–551. PubMed
- Dean W, Talbot S, Dean A. Reframing clinician distress: moral injury not burnout. Fed Pract Health Care Prof VA, DoD, PHS. 2019;36(9):400–402. PubMed
- Dean W. Why Developing Individual Resilience Isn’t Enough to Heal Moral Injury. Institute for Healthcare Improvement; 2025. https://www.ihi.org/library/blog/why-developing-individual-resilience-isnt-enough-heal-moral-injury
- Nash WP, Marino Carper TL, Mills MA, et al. Psychometric evaluation of the moral injury events scale. Mil Med. 2013;178(6):646–652. PubMed CrossRef
- Koenig HG, Youssef NA, Ames D, et al. Examining the overlap between moral injury and PTSD in US veterans and active duty military. J Nerv Ment Dis. 2020;208(1):7–12. PubMed CrossRef
- Bryan CJ, Bryan AO, Roberge E, et al. Moral injury, posttraumatic stress disorder, and suicidal behavior among National Guard personnel. Psychol Trauma. 2018;10(1):36–45. PubMed CrossRef
- Kurth C. Moral anxiety and moral agency. Oxf Stud Normative Ethics. 2015;5:171–195.
- Kinghorn W. Challenging the hegemony of the symptom: reclaiming context in PTSD and moral injury. J Med Philos. 2020;45(6):644–662. PubMed CrossRef
- Litz BT. The future of moral injury and its treatment. J Military, Veteran, Fam Health. 2023;9(2):1–5. CrossRef
- Litz BT, Contractor AA, Rhodes C, et al. Distinct trauma types in military service members seeking treatment for posttraumatic stress disorder. J Traumatic Stress. 2018;31(2):286–295. PubMed CrossRef
- Hall NA, Everson AT, Billingsley MR, et al. Moral injury, mental health and behavioural health outcomes: a systematic review of the literature. Clin Psychol Psychother. 2022;29(1):92–110. PubMed CrossRef
- Maguen S, Nichter B, Norman SB, et al. Moral injury and substance use disorders among US combat veterans: results from the 2019-2020 National Health and Resilience in Veterans Study. Psychol Med. 2023;53(4):1364–1370. PubMed CrossRef
- Williamson V, Stevelink SAM, Greenberg N. Occupational moral injury and mental health: systematic review and meta-analysis. Br J Psychiatry. 2018;212(6):339–346. PubMed CrossRef
- Griffin BJ, Maguen S, McCue ML, et al. Moral injury is independently associated with suicidal ideation and suicide attempt in high-stress, service-oriented occupations. NPJ Ment Health Res. 2025;4(1):32. PubMed CrossRef
- American Psychiatric Association. Moral Injury During the COVID-19 Pandemic. 2020. https://www.psychiatry.org/file%20library/psychiatrists/apa-guidance-covid-19-moral-injury.Pdf
- Lennon RP, Parascando J, Talbot SG, et al. Prevalence of moral injury, burnout, anxiety, and depression in healthcare workers 2 years in to the COVID-19 pandemic. J Nerv Ment Dis. 2023;211(12):981–984. PubMed CrossRef
- Wilson C, Pence DM, Conradi L. Trauma-informed care. In: Encyclopedia of Social Work; 2013.
- Frank JD. Persuasion and Healing: A Comparative Study of Healing. Johns Hopkins Press; 1961.
- Viederman M, Perry SW 3rd. Use of a psychodynamic life narrative in the treatment of depression in the physically ill. Gen Hosp Psychiatry. 1980;2(3):177–185. PubMed CrossRef
- Alford CF. Trauma, Culture and PTSD. Springer; 2016.
- Bekes VB, Szabo D, Levay EE, et al. Moral injury and shame mediate the relationship between childhood trauma and borderline personality disorder, PTSD, and complex PTSD symptoms in psychiatric inpatients. J Personal Disord. 2023; 37.
- Martin MW. Depression: illness, insight and identity. Philosophy, Psychiatry Psychol. 1999;6(4):271–286.
- Boscarino JA, Adams RE, Wingate TJ, et al. Impact and risk of moral injury among deployed veterans: implications for veterans and mental health. Front Psychiatry. 2022;13:899084. PubMed CrossRef
- Aronson KR, Morgan NR, Doucette CE, et al. Associations among combat exposure, adverse childhood experiences, moral injury, and posttraumatic growth in a large cohort of post-9/11 veterans. Psychol Trauma. 2025;17(3):639–647. PubMed CrossRef
- Ryu MY, Martin MJ, Jin AH, et al. Characterizing moral injury and distress in US Military Surgeons deployed to far-forward combat Environments in Afghanistan and Iraq. JAMA Netw Open. 2023;6(2):e230484. PubMed CrossRef
- Department of Veterans Affairs. Military Sexual Trauma. 2021. https://www.mentalhealth.va.gov/docs/mst_general_factsheet.pdf
- U.S. Government. Veterans’ benefits: Counseling and treatment for sexual trauma, 38 USC §1720D. 2014. https://www.gpo.gov/fdsys/pkg/USCODE-2014-title38/pdf/USCODE-2014-title38-partII-chap17-subchapII-sec1720D.pdf
- Lutwak N, Dill C. Military sexual trauma increases risk of post-traumatic stress disorder and depression thereby amplifying the possibility of suicidal ideation and cardiovascular disease. Mil Med. 2013;178(4):359–361. PubMed CrossRef
- Wilson LC. The prevalence of military sexual trauma: a meta-analysis. Trauma, Violence & Abuse. 2018;19(5):584–597. PubMed CrossRef
- Bartlett BA, Iverson KM, Mitchell KS. Intimate partner violence and disordered eating among male and female veterans. Psychiatry Res. 2018;260:98–104. PubMed CrossRef
- Goldstein LA, Dinh J, Donalson R, et al. Impact of military trauma exposures on posttraumatic stress and depression in female veterans. Psychiatry Res. 2017;249:281–285. PubMed CrossRef
- Jenkins MM, Colvonen PJ, Norman SB, et al. Prevalence and mental health correlates of insomnia in first-encounter veterans with and without military sexual trauma. Sleep. 2015;38(10):1547–1554. PubMed CrossRef
- Kimerling R, Street AE, Pavao J, et al. Military-related sexual trauma among Veterans Health Administration patients returning from Afghanistan and Iraq. Am J Public Health. 2010;100(8):1409–1412. PubMed CrossRef
- Blais RK, Brignone E, Maguen S, et al. Military sexual trauma is associated with post-deployment eating disorders among Afghanistan and Iraq veterans. Int J Eat Disord. 2017;50(7):808–816. PubMed CrossRef
- Maguen S, Cohen B, Ren L, et al. Gender differences in military sexual trauma and mental health diagnoses among Iraq and Afghanistan veterans with posttraumatic stress disorder. Womens Health Issues. 2012;22(1):e61–e66. PubMed CrossRef
- Brown LS. Cultural competence in trauma therapy: beyond the flashback. Am Psychol Assoc. 2008. https://doi.org/10.1037/11752-000
- Herman J. Trauma and recovery: The Aftermath of Violence—From Domestic Abuse to Political Terror. Basic Books; 2015.
- Dean W, Morris D, Manzur MK, et al. Moral injury in health care: a unified definition and its relationship to burnout. Fed Pract. 2024;41(4):104–107. PubMed CrossRef
- Dean W. Moral injury and preserving our profession. Mo Med. 2023;120(6):423–425. PubMed
- Kirzinger A, Kearney A, Hamel L, et al. Frontline Health Care Survey. Agency for Healthcare Research and Quality; 2021. Accessed September 16, 2025. https://www.ahrq.gov/nursing-home/resources/frontline-workers-survey.html
- Ritter M, Vance M, Iskander J. Moral injury among US Public Health Service first responders during the COVID-19 pandemic. Public Health Rep. 2023;138(5):732–735. PubMed CrossRef
- Donovan N, Lukic G, Mason O. A scoping review of moral injury in refugees. Eur J Psychotraumatol. 2025;16(1):2501369. PubMed CrossRef
- Currier JM, Foster JD, Isaak SL. Moral injury and spiritual struggles in military veterans: a latent profile analysis. J Trauma Stress. 2019;32(3):393–404. PubMed CrossRef
- O’Garo K-GN, Koenig HG. Spiritually integrated cognitive processing therapy for moral injury in the setting of PTSD: initial evidence of therapeutic efficacy. J Nerv Ment Dis. 2023;211(9):656–663. PubMed
- Pyne JM, Currier J, Hinkson KD, et al. Addressing religious and spiritual diversity in moral injury care: five perspectives. Curr Treat Options Psychiatry. 2023;10(4):446–462. CrossRef
- Propst LR, Ostrom R, Watkins P, et al. Comparative efficacy of religious and nonreligious cognitive-behavioral therapy for the treatment of clinical depression in religious individuals. J Consult Clin Psychol. 1992;60(1):94–103. PubMed CrossRef
- Herman JL. Truth and Repair: How Trauma Survivors Envision Justice. Basic Books; 2023.
- Litz BT, Walker HE. Moral injury: an overview of conceptual, definitional, assessment, and treatment issues. Annu Rev Clin Psychol. 2025;21(1):251–277. PubMed CrossRef
- Pearce M, Haynes K, Rivera NR, et al. Spiritually integrated cognitive processing therapy: a new treatment for post-traumatic stress disorder that targets moral injury. Glob Adv Health Med. 2018;7:2164956118759939. PubMed CrossRef
- Borges LM, Barnes SM, Farnsworth JK, et al. Case conceptualizing in Acceptance and Commitment Therapy for Moral Injury: an active and ongoing approach to understanding and intervening on moral injury. Front Psychiatry. 2022;13:910414. PubMed CrossRef
- Diekmann C, Issels L, Alliger-Horn C, et al. Traumatized German soldiers with moral injury - value-based cognitive-behavioral group therapy to treat war-related shame. Front Psychiatry. 2023;14:1173466. PubMed CrossRef
- Litz BT, Yeterian J, Berke D, et al. A controlled trial of adaptive disclosure-enhanced to improve functioning and treat posttraumatic stress disorder. J Consulting Clin Psychol. 2024;92(3):150–164. PubMed CrossRef
- DeMarco MJ. 6-Fold path to self-forgiveness: an interdisciplinary model for the treatment of moral injury with intervention strategies for clinicians. Front Psychol. 2024;15:1437070. PubMed CrossRef
- Mitchell JM, Ot’alora MG, van der Kolk B, et al. MDMA-assisted therapy for moderate to severe PTSD: a randomized, placebo-controlled phase 3 trial. Nat Med. 2023;29(10):2473–2480. PubMed
- Robison R, Barrow R, Conant C, et al. Single treatment with MM120 (lysergide) in generalized anxiety disorder: a randomized clinical trial. JAMA. 2025;334(15):1358–1372. PubMed CrossRef
- Raison CL, Sanacora G, Woolley J, et al. Single-dose psilocybin treatment for major depressive disorder: a randomized clinical trial. JAMA. 2023;330(9):843–853. PubMed CrossRef
- Beesley VL, Kennedy TJ, Maccallum F, et al. Psilocybin-assisted supportive psychotherapy in the treatment of prolonged grief (PARTING) trial: protocol for an open-label pilot trial for cancer-related bereavement. BMJ Open. 2025;15(4):e095992. PubMed CrossRef
- Bogenschutz MP, Ross S, Bhatt S, et al. Percentage of heavy drinking days following psilocybin-assisted psychotherapy vs placebo in the treatment of adult patients with alcohol use disorder: a randomized clinical trial. JAMA Psychiatry. 2022;79(10):953–962. PubMed CrossRef
- Anderson BT, Danforth A, Daroff R, et al. Psilocybin-assisted group therapy for demoralized older long-term AIDS survivor men: an open-label safety and feasibility pilot study. eClinicalMedicine. 2020;27:100538. PubMed CrossRef
- Back AL, Freeman-Young TK, Morgan L, et al. Psilocybin therapy for clinicians with symptoms of depression from frontline care during the COVID-19 pandemic: a randomized clinical trial. JAMA Netw Open. 2024;7(12):e2449026. PubMed CrossRef
- Ellis S, Bostian C, Feng W, et al. Single-dose psilocybin for U.S. military veterans with severe treatment-resistant depression: a first-in-kind open-label pilot study. J Affective Disord. 2025;369:381–389. PubMed CrossRef
- Mithoefer MC, Mithoefer AT, Feduccia AA, et al. 3,4-methylenedioxymethamphetamine (MDMA)-assisted psychotherapy for post-traumatic stress disorder in military veterans, firefighters, and police officers: a randomised, double-blind, dose-response, phase 2 clinical trial. Lancet Psychiatry. 2018;5(6):486–497. PubMed CrossRef
- Schenberg EE, Hauskeller C, Schwarz CG, et al. Psychedelic therapies: healing for the wrong reasons?. Nat Ment Health. 2024;2:1265–1267. CrossRef
- Agin-Liebes G, Nielson EM, Zingman M, et al. Reports of self-compassion and affect regulation in psilocybin-assisted therapy for alcohol use disorder: an interpretive phenomenological analysis. Psychol Addict Behav. 2024;38(1):101–113. PubMed CrossRef
- Agin-Liebes GI, Malone T, Yalch MM, et al. Long-term follow-up of psilocybin-assisted psychotherapy for psychiatric and existential distress in patients with life-threatening cancer. J Psychopharmacol. 2020;34(2):155–166. PubMed CrossRef
- Barnes HA, Hurley RA, Taber KH. Moral injury and PTSD: often co-occurring yet mechanistically different. J Neuropsychiatry Clin Neurosci. 2019;31(2):A4–A103. PubMed CrossRef
- Fulton TM, Guelfo A, Elbasheir A, et al. Resting-state neural signatures of moral injury: associations with rumination. Biol Psychiatry Cogn Neurosci Neuroimaging. 2025.
- Terpou BA, Lloyd CS, Densmore M, et al. Moral wounds run deep: exaggerated midbrain functional network connectivity across the default mode network in posttraumatic stress disorder. J Psychiatry Neurosci. 2022;47(1):E56–E66. PubMed CrossRef
- Carhart-Harris RL, Friston KJ. REBUS and the anarchic brain: toward a unified model of the brain action of psychedelics. Pharmacol Rev. 2019;71(3):316–344. PubMed CrossRef
- Smith-MacDonald L, Lusk J, Lee-Baggley D, et al. Companions in the abyss: a Feasibility and acceptability study of an online therapy group for healthcare providers working during the COVID-19 pandemic. Front Psychiatry. 2022;12:801680. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!