Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(2):25f04076
Author affiliations are listed at the end of this article.
Have you ever been frustrated by listening to case presentations that lacked structure or seemed to miss key elements? Have you ever been led astray by a consultee’s confidence in their analysis of the case? Have you wondered whether there was a better way to distill and convey the essence of a case to facilitate training and interdisciplinary communication? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Three presentations of the same patient will be offered to illustrate the notion that case presentations often drive the creation of differential diagnoses by what is said (and not said) and by whether the information given is the “lead” or merely added as an extra (potentially interesting) tidbit.
Presentation 1: Ms A, a 71-year-old recently widowed woman, was seen by her primary care provider (PCP) at the request of Ms A’s daughter, who was concerned that her mother’s depression, poor self-care, and lack of energy reflected a recurrence of major depressive disorder (MDD). Ms A’s daughter wondered whether her mother should restart the antidepressant (sertraline) that she had used for the treatment of prior depressive episodes.
Presentation 2: Ms A, a 71-year-old woman, was seen by her PCP at the request of Ms A’s daughter, who was concerned by her mother’s impaired attention, concentration, and self-care. She feared that her mother was developing Alzheimer disease, and she wanted to know how long she would be able to function on her own.
Presentation 3: Ms A, a 71-year-old recently widowed woman with depression, poor self-care, impaired attention, and word-finding difficulty, was seen by her PCP at the request of her daughter because Ms A’s impaired attention and word-finding difficulty were not characteristic of her prior episodes of depression. Ms A’s daughter wondered what could be responsible for her mother’s symptoms.
DISCUSSION
What Information Should Be Included in Case Presentations?
Starting in the first year of medical school, trainees learn how to build a patient database comprised of the chief concern (or complaint), the history of the present illness, the past medical and psychiatric history, social history, family history, medication list, allergies, mental status examination, and findings from laboratory testing and the physical examination. When trainees present cases to their supervisors, they often struggle to decide how much detail should be included and how long the presentation should be. These decisions are typically influenced by several factors, such as the number of cases that need to be presented, the urgency of clinical interventions, and the supervisor’s level of confidence in the trainee’s clinical judgment, which often prompts abbreviated presentations that are focused on the information needed to formulate and initiate an action plan. Nonetheless, some trainees provide lengthy presentations, which frequently reflects difficulty in synthesizing the salient features of the patient’s history or formulating a coherent diagnostic impression or treatment plan. Others, perhaps guided by overconfidence, offer presentations that are overly concise, with telegraphic summaries of the most readily apparent pieces of clinical data (eg, “A 52-year-old man experienced crushing substernal chest pain; his ECG demonstrated ST elevations and Q waves, and troponin levels were elevated. He was diagnosed with a myocardial infarction and admitted to the cardiac care unit.”) Many supervisors encourage trainees to formulate cases efficiently and to recognize characteristic patterns of illness, whereas others emphasize a more deliberate approach that prioritizes minimizing diagnostic errors by considering a broad differential rather than focusing solely on the most probable or most serious condition. Listeners to case presentations are often influenced by the presenter’s framing of the case and may be drawn toward the same diagnostic conclusion. In such instances, potentially critical details—such as recent transoceanic travel, calf pain, or dehydration—may be omitted. Conversely, some presenters offer an abundance of information, including a family history of coronary artery disease and comorbid conditions (such as MDD, diabetes mellitus, hypertension, and hypercholesterolemia and even recent intranasal cocaine use to counteract travel-related fatigue prior to the onset of chest pain).
In our 3 ultrabrief vignettes, each presenter offered only selected aspects of the case, directing listeners toward particular domains—disordered mood, impaired cognition, and the complex interplay among affective symptoms, medical conditions, and their treatments. Consequently, listeners may have difficulty constructing a comprehensive differential diagnosis, as critical information remains unknown or unarticulated. Supervising clinicians must remain vigilant to avoid coming to premature closure based solely on information presented by trainees, as these vignettes illustrate how even small deviations in case presentation can lead to markedly different diagnostic formulations.
How (and Why) Should Case Formulations Be Structured?
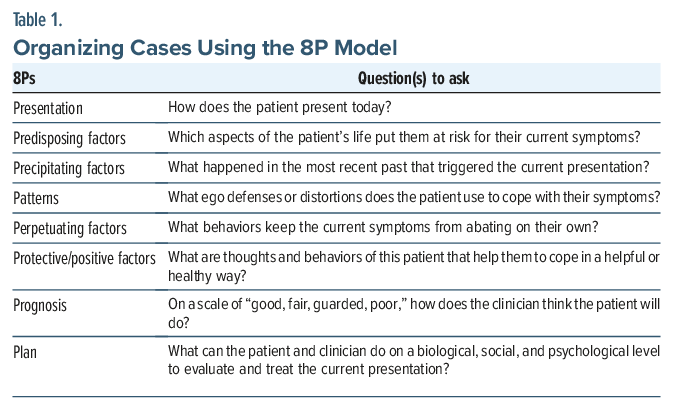
As case formulation plays a critical role in how cases might be approached, using a framework that ensures a structured approach can be useful. Case formulations can frame a patient’s history with the biopsychosocial model using the 8P model, which builds on the Bolton 4P model1 that involves predisposing, precipitating, perpetuating, and positive factors. The 8P model organizes case formulations with presentation, predisposing factors, precipitating factors, patterns, perpetuating factors, protective/positive factors, prognosis, and plans (Table 1).
Once the history has been obtained from the patient and other sources, it is reasonable to consider what clinicians aspire to do with that information. Organizing and integrating the information (using the 8P model) can lead to a deeper understanding of the symptoms and the person who has those symptoms. If the intricacies of why patients see clinicians are not unearthed, it becomes more likely that symptoms will be targeted rather than directing attention to the underlying problem.
How Can Training and Clinical Care Be Enhanced by Creating Thoughtful and Structured Presentations and Case Formulations?
Metacognition (the practice of thinking about one’s thinking) is essential to training and clinical practice. The act of organizing a vast amount of information about patients into a coherent narrative can lead clinicians to reflect on all aspects of the presentation and thus the plan. Creating formulations in training (as well as later in clinical practice) trains clinicians to think and reflect on how (and why) the patient is presenting for medical care. Reflection brings learning, development of therapeutic relationships, and development in professional practice.2
What Might Get Missed During Case Formulation?
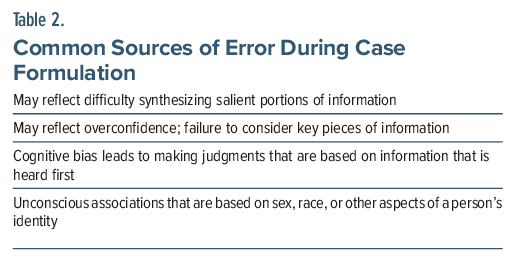
Stigma, bias, and premature anchoring each interfere with diagnostic accuracy and the doctor-patient interaction. Equally as important as formulating complex cases in a structured fashion is ensuring that our formulations are accurate and complete. In addition to common pitfalls (such as being overinclusive or overly concise in one’s formulation), it is important to consider thought processes and biases that may lead to erroneous case formulations (Table 2). The dual process model has described how individuals solve problems and make decisions, with approaches to thinking that include pattern-based, intuitive thinking and logical reasoning and analysis.3 Given the time constraints placed on the practitioners of medicine and the reactions associated with being human, physicians often rely on the first mode to make diagnostic decisions. While this often works well for simple presentations of common problems, more complex and uncommon presentations are apt to reveal cognitive biases when this framework is relied upon.3 A recent study of premature anchoring (ie, a source of cognitive bias that leads to making judgments based on information that is heard first) showed that veterans with congestive heart failure (CHF) were less likely to be tested or diagnosed with a pulmonary embolism if their chief complaint indicated that they had a history of CHF.4
More broadly, implicit bias (the phenomenon of making unconscious associations) can also lead to erroneous case formulations. Implicit bias facilitates the making of associations that are based on sex, race, or other aspects of a person’s identity.5,6 Since clinicians are unaware of these associations, they fall into cognitive traps because of them. With thoughtful reflection, biases can be brought into consciousness and corrected.
How Important Is Nonverbal Communication That Is Provided by Patients to Their Health Care Providers?
In addition to under-recognition of bias, nonverbal cues can also be a rich source of information that, when missed, can lead to errors in case formulation. Charles Darwin, in his 1882 book, The Expression of the Emotions in Man and Animals, argued that bodily movements (eg, facial expressions) represent internal emotional states that are universal to our species and serve an evolutionary purpose.7 Comparing nonverbal communication with verbal communication (ie, congruent vs. incongruent) often yields clinical information that distinguishes truth from deception, accesses more details than are verbally volunteered, and assists with diagnostic clarity.8 Nonverbal communication by presenters of cases can also affect the diagnostic assessment of clinical preceptors.
George B. Murray, MD, while serving as a consultation psychiatrist at Massachusetts General Hospital, developed the concept of limbic music, described as “a term that denotes the existential, clinical raw feel emanating from the patient. It is a truer rendering of the patient’s clinical state than is articulate speech.”9(p22) The neocortex (which includes the Broca area) is the foundation for the words of what one thinks and feels. However, most actions performed daily are created within the limbic system before neocortical (ie, nonsensory structures) intellectualization (ie, suppression of affect or so-called “neocortical squelch” can be produced).9(p22) Thus, this concept of limbic music can be used to interpret interactions and refine assessments of psychiatric presentations.10 Murray wrote, “limbic music never lies”9(p22) (ie, the “music” of communication is more meaningful than the lyrics/words).
How Might Artificial Intelligence Be Used to Fill Gaps in the Case Formulation?
Artificial intelligence (AI) is a potentially novel approach to information gathering and case formulation. AI is increasingly used in health care settings to record patient histories with greater efficiency, to streamline the evaluation process, to refine the diagnosis, and to plan treatment. AI can gather and classify content within the electronic medical record (eg, numerical values, dates, ages, and images).11 Moreover, recent advances have enabled AI to analyze complex data utilizing natural language processing (NLP) algorithms to generate clinical impressions.11,12 Beyond making diagnoses, AI shows tremendous potential in identifying and classifying the level of risk associated with complex conditions.13,14
NLP also plays a key role in automating history taking using chatbots and transcription tools that enable patient interviews to be conducted (or recorded) in real time. Systems (eg, Chat GPT-4) can be used to transcribe the content of physician-patient interactions, although shortcomings can flow from failing to recognize nonverbal cues.15–17
In addition, AI supports clinicians in the creation of differential diagnoses through offering probabilistic assessments derived from a broad spectrum of patient data.17–19 Studies have also assessed the efficiency of AI in the creation of evidence-based treatment recommendations, while other applications facilitate remote patient monitoring, track medication adherence, and alert providers to treatment nonadherence.20
The accelerating integration of AI into clinical practice raises questions about how clinicians process and synthesize case information. Just as supervising clinicians must remain vigilant against coming to premature diagnostic closure based solely on trainee presentations—where small omissions or framing bias can yield markedly different diagnostic impressions—clinicians must also exercise caution when interpreting AI-generated data. AI may streamline the information gathering process, but it cannot replace sound clinical judgment in patient care.
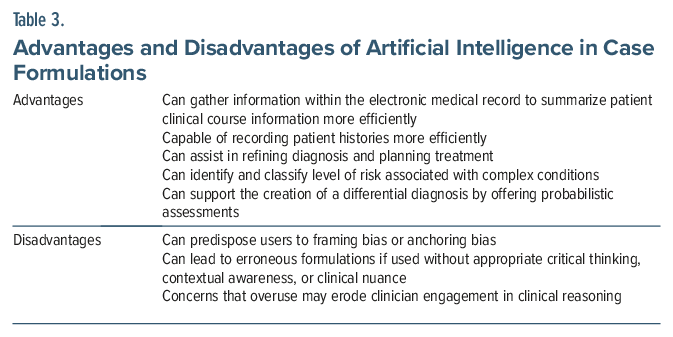
AI in medicine represents a double-edged sword (Table 3): It holds immense promise for enhancing diagnostic accuracy, efficiency, and patient care, while simultaneously raising concerns regarding data security, safety, and the erosion of human engagement in clinical reasoning.17,21
What Information Is Needed by Consultees, Covering Physicians, and Supervisors?
To ensure comprehensive patient care, clinical information should be passed on to consultees and covering physicians who participate in the care of patients. Communication failures during handoffs are common, and they are associated with medical errors and adverse events,22 in part due to the data that are, or are not, presented to colleagues.
Well-maintained medical records can provide documentation that facilitates communication among colleagues. Timely, accurate, and accessible medical records also are important in many aspects of clinical care, including prevention of medication errors, avoiding drug-drug interactions, risk stratification and mitigation, and avoiding withdrawal syndromes. Furthermore, documenting a patient’s history and clinical course in the medical record provides an opportunity to create a cohesive narrative that helps to frame a differential diagnosis, to guide a medical workup, and to establish a treatment plan.
Several instruments and strategies can enhance how information from the medical record is conveyed during handoffs (eg, workshops and educational units,23,24 and a simplified Situation-Background-Assessment-Recommendation [SBAR] tool).25 I-PASS (a verbal and written mnemonic for Illness severity, Patient summary, Action list, Situational awareness with contingency planning, Synthesis by the receiver) is another tool that can reduce adverse events. In a prospective intervention study of 10,740 patients, it was determined that the flexible I-PASS system that employed a structured patient handoff can be individualized to improve communication and reduce preventable adverse events.26 However, relatively little work has been done to adapt I-PASS for psychiatric use (eg, management of problematic behaviors, enhancing pharmacotherapy).27
WHAT HAPPENED TO MS A?
Our first vignette focused on depressive features and a prior response to an antidepressant, while the second vignette highlighted Ms A’s cognitive impairment, and the third vignette introduced the concept of whether Ms A’s symptoms presented differently from prior episodes of dysfunction. Each vignette reported information accurately, but inadequately. Each vignette reflected the biases introduced by Ms A’s daughter or by the treating clinician. Fortunately, given the prominent cognitive features of Ms A’s presentation and the subacute onset of these symptoms, further investigation was done (including brain magnetic resonance imaging [MRI]). The MRI revealed a glioblastoma that required radiation therapy, tumor resection, and steroids to reduce central nervous system edema.
CONCLUSION
Each clinical presentation conveys large amounts of information. This makes it challenging to strike a balance when attempting to consider a comprehensive yet parsimonious presentation. Presentations can be too brief (ie, lacking essential information), overly inclusive (ie, obfuscating key pieces of information), or misguided. However, precise structuring of clinical information can facilitate training and interdisciplinary communication. Moreover, recognition of cognitive biases (eg, premature anchoring or implicit biases) can enhance diagnostic accuracy and patient-physician relationships, while ensuring that key elements of information are not omitted.
Clinical tools can assist with case formulations. Despite AI’s inherent dangers, it has great potential to assist with case formulations, while the 8P model provides a comprehensive framework to help clinicians gain a deeper understanding of each patient that goes far beyond their symptoms and illnesses. Methods (such as SBAR or I-PASS) can help to standardize clinical presentations and handoffs. Finally, when considering a case presentation, clinicians should be wary about premature anchoring to the elements presented, as this can lead to erroneous conclusions.
Article Information
Published Online: April 9, 2026. https://doi.org/10.4088/PCC.25f04076
© 2026 Physicians Postgraduate Press, Inc.
Submitted: September 8, 2025; accepted January 7, 2026.
To Cite: Chang AK, Ho PA, Rustad JK, et al. Strategies to formulate, present, and document complex cases and avoid critical omissions. Prim Care Companion CNS Disord 2026;28(2):25f04076.
Author Affiliations: Ohio State University, Columbus, Ohio (Chang); Te Toka Tumai/Auckland City Hospital, Auckland, New Zealand (Chang); Geisel School of Medicine at Dartmouth, Lebanon, New Hampshire (Ho, Rustad, McGarry, Fox); Larner College of Medicine at University of Vermont (Rustad); White River Junction VA Medical Center, White River Junction, Vermont (Rustad); Burlington Lakeside VA Community Based Outpatient Clinic, Burlington, Vermont (Rustad); Dartmouth-Hitchcock Medical Center, Lebanon, New Hampshire (Ho, McGarry, Fox); Massachusetts General Hospital/Harvard Medical School, Boston, Massachusetts (Stern).
Chang, Ho, Rustad, McGarry, and Fox are co-first authors; Stern is senior author.
Corresponding Author: Patrick A. Ho, MD, MPH, Geisel School of Medicine at Dartmouth, Lebanon, New Hampshire ([email protected]).
Financial Disclosure: Dr Rustad is employed by the United States Department of Veterans Affairs, but the opinions expressed in this article do not reflect those of the Department of Veterans Affairs. Dr Stern has received royalties from Elsevier for editing textbooks on psychiatry. Drs Chang, Ho, McGarry, and Fox have nothing to disclose.
Funding/Support: None.
Clinical Points
- Case presentations often drive the creation of the differential diagnosis by what is said (and not said) and by whether the information given is the “lead” or merely added as a (potentially interesting) tidbit.
- While it is important to trust those with whom one works, clinicians should be wary of coming to premature closure and being anchored to the presenter’s hypothesis by their words or body language.
- Case formulations can frame a patient’s history using the biopsychosocial model using the 8P model, which builds on the Bolton 4P model that involves predisposing, precipitating, perpetuating, and positive factors.
- Recognition of cognitive biases (eg, premature anchoring or implicit biases) can enhance diagnostic accuracy and patient-physician relationships.
References (27)

- Bolton JW. Case formulation after Engel: the 4P model. Philos Psychiatry Psychol. 2014;21(3):179–189. CrossRef
- Sandars J. The use of reflection in medical education: AMEE Guide No. 44. Med Teach. 2009;31(8):685–695. PubMed CrossRef
- Royce CS, Hayes MM, Schwartzstein RM. Teaching critical thinking: a case for instruction in cognitive biases to reduce diagnostic errors and improve patient safety. Acad Med. 2019;94(2):187–194. PubMed CrossRef
- Ly DP, Shekelle PG, Song Z. Evidence of anchoring bias during physician decision-making. JAMA Intern Med. 2023;193(8):818–823.
- Fitzgerald C, Hurst S. Implicit bias in healthcare professionals: a systematic review. BMC Med Ethics. 2017;18(1):19. PubMed CrossRef
- Hall WJ, Chapman MV, Lee KM, et al. Implicit racial/ethnic bias among health care professionals and its influence on health care outcomes: a systematic review. Am J Public Health. 2015;105(12):e60–e76. PubMed CrossRef
- Chahal K. The utility of assessing nonverbal communication in the psychiatric evaluation. Am J Psychiatry Residents’ J. 2017:3–5. CrossRef
- Darwin C. The Expression of the Emotions in Man and Animals. London: Penguin Group; 2009. CrossRef
- Murray GB. Limbic music. Psychosomatics. 1992;33(1):16–23. PubMed CrossRef
- Kontos N. Limbic music. In: Stern TA, Beach SR, Smith FA, et al, eds. Massachusetts General Hospital Handbook of General Hospital Psychiatry. Eighth edition. Philadelphia, PA: Elsevier; 2025:46–55.
- Lee S, Kim HS. Prospect of artificial intelligence based on electronic medical record. J Lipid Atheroscler. 2021;10(3):282–290. PubMed CrossRef
- Somnay YR, Craven M, McCoy KL, et al. Improving diagnostic recognition of primary hyperparathyroidism with machine learning. Surgery. 2017;161(4):1113–1121. PubMed CrossRef
- Kawaler E, Cobian A, Peissig P, et al. Learning to predict post-hospitalization VTE risk from EHR data. AMIA Annu Symp Proc. 2012;2012:436-445. PubMed
- Campanella G, Hanna MG, Geneslaw L, et al. Clinical-grade computational pathology using weakly supervised deep learning on whole slide images. Nat Med. 2019;25(8):1301–1309. PubMed CrossRef
- Nadarzynski T, Miles O, Cowie A, et al. Acceptability of artificial intelligence (AI)-led chatbot services in healthcare: a mixed-methods study. Digit Health. 2019;5:2055207619871808. PubMed CrossRef
- Haug CJ, Drazen JM. Artificial intelligence and machine learning in clinical medicine. N Engl J Med. 2023;388(13):1201–1208. PubMed CrossRef
- Krishnan G, Singh S, Pathania M, et al. Artificial intelligence in clinical medicine: catalyzing a sustainable global healthcare paradigm. Front Artif Intell. 2023;6:1227091. PubMed CrossRef
- Probability Density Function. DeepAI. 2019. Accessed July 25, 2025. https://deepai.org/machine-learning-glossary-and-terms/probability-density-function
- Muhammad W, Hart GR, Nartowt B, et al. Pancreatic cancer prediction through an artificial neural network. Front Artif Intell. 2019;2:2. PubMed CrossRef
- Babel A, Taneja R, Mondello Malvestiti F, et al. Artificial intelligence solutions to increase medication adherence in patients with non-communicable diseases. Front Digit Health. 2021;3:669869. PubMed CrossRef
- Kashoub M, Al Abdali M, Al Shibli E, et al. Artificial intelligence in medicine: a double-edged sword or a Pandora’s Box? Oman Med J. 2023;38(5):e542. PubMed CrossRef
- Joint Commission on Accreditation of Healthcare Organizations. Sentinel event statistics released for 2015. Jt Comm Perspect. 2016;36:10.
- Frank A, Berlin R, Adelsky S, et al. Transitions in care: a workshop to help residents and fellows provide safe, effective handoffs for acute psychiatry patients. MedEdPORTAL. 2020;16:10951. PubMed CrossRef
- Ying J, Zhang MW, Tan GM, et al. Initiative to improve handover notes in a tertiary psychiatric hospital. BMJ Open Qual. 2024;13:e 002601. CrossRef
- Vallabhaneni K, Hazan J, Donaldson L, et al. Improving the handover process in a psychiatry liaison setting. BMJ Open Qual. 2022;11(1):e001627. PubMed CrossRef
- Starmer AJ, Spector ND, Srivastava R, et al. I-PASS Study Group. Changes in medical errors after implementation of a handoff program. N Engl J Med. 2014;371(19):1803–1812. PubMed CrossRef
- Bowes MR, Santiago PN, Hepps JH, et al. Using I-PSS in psychiatry residency transitions of care. Acad Psychiatry. 2018;42(4):534–537. PubMed CrossRef
Enjoy this premium PDF as part of your membership benefits!





