See related article by Breitzig et al
Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) mimic the physiological effects of native incretins insofar as they facilitate glucose-stimulated insulin secretion, decrease glucagon synthesis and release, slow gut motility, and reduce appetitive drive.1 Exenatide was FDA-approved for the treatment of adults with type 2 diabetes mellitus (T2DM) in 2005. Since this time there has been an extraordinary increase in the prescribing of GLP-1 RAs in the general population, especially in the last five – seven years. For example, it is estimated that as many as 1 in 6 US adults have been prescribed 1 or more GLP-1 RAs.
The high and increasing demand for GLP-1 RAs in the general population is due to multiple factors including their transformative effects on weight and metabolic abnormalities, media coverage, promotion by social media influencers and the consumer-based approach to their marketing and direct-to-consumer channels of availability. The demand for GLP-1 RAs has strained supply chain and manufacturing capabilities, which has resulted in a contemporaneous rapid increase in online/compounding pharmacy utilization.
Subsequent to the approval of exenatide, additional GLP-1 RAs have been FDA-approved, with differences across agents in indication for use (eg, pediatrics), route and/or intervals of administration, pharmacology, efficacy, and tolerability. In addition to GLP-1 RA monoagonists (eg, semaglutide), dual incretin receptor agonists targeting GLP-1R and glucose-insulinotropic polypeptide receptors (GIP) (eg, tirzepatide) are now available, with anticipated approval of triple agonists (eg, retatrutide; GLP-1 RA-GIP-glucagon [GCG agonist]).2 Also in development are GLP-1 conjugates that combine GLP-1 and GCG agonists (eg, survodutide), GLP-1 and GIP receptor antagonism (eg, MariTide), and GLP-1 RA-amylin receptor agonists (eg, amycretin, cagrilintide-semaglutide).3
The report by Breitzig et al,4 from data obtained from a commercial claims database, indicates that among privately insured persons with mood disorders, there has been an increase in the prescription of GLP-1 RAs (ie, 1.5%–7.2%) during the time period 2018–2023, with primary care and nurse practitioners rather than psychiatrists increasing prescription volume. What was especially notable to me was that the increase in GLP-1 RA prescription could not be fully explained by FDA-approved indications (eg, T2DM) alone. This result suggests that the increasing use of GLP-1 RAs in the mood disorder population appears to be for off-label clinical presentations. I found the study results not only interesting but also very much in accordance with one of the most frequently asked questions to me by health care providers: Whether persons with serious mental illness and/or substance use disorders (SMI-SUD) should be prescribed GLP-1 RAs specifically to treat their mental disorders. The response to this question as I see it can be framed as follows: Which clinical targets are currently evidence-based, and which targets are aspirational?
Currently, GLP-1 RAs are FDA-approved (with differences across the agents) for 6 medical conditions, each of which differentially affects persons with SMI-SUD. For example, obesity, T2DM, metabolic liver disease, obstructive sleep apnea, obesity-related cardiovascular mortality, and progressive kidney disease due to T2DM all occur at a significantly higher rate in persons with mental disorders, with some evidence indicating shared pathophysiology.5–8 Consequently, GLP-1 RAs are currently evidence-based treatments for common conditions that not only differentially affect persons with SMI-SUD but also contribute to the morbidity and mortality of these conditions.
For example, mortality studies have reported that among persons with SMI-SUD, cardiovascular causes account for the largest number of excess and premature deaths, suggesting that GLP-1 RAs hold promise to be transformative in this vulnerable population by reducing the ignominious mortality gap that exists between persons with SMI-SUD and the general population.9,10 Along with the aforementioned currently approved and evidence-based FDA indications, other disorders that may possibly receive FDA approval include heart failure with preserved ejection fraction, peripheral artery disease, arthritis, and polyendocrine metabolic ovarian syndrome (PMOS). It is not without interest that these potential additional indications, wherein determinations as to whether the evidence for GLP-1 RAs is definitive, also differentially affect SMI-SUD.11,12
The prescription of GLP-1 RAs to mitigate weight gain and/or metabolic disruption associated with psychotropic drugs (eg, clozapine) is evidence-based, supported by replicated results from rigorous short- and intermediate-term randomized controlled studies.13–15 The benefits on anthropometrics and metabolic measures in this context far exceed effect size estimates for metformin.16,17 Whether GLP-1 RAs protect against lithium-induced nephrotoxicity is unknown, but it’s not without interest that nephroprotective mechanisms implicated with GLP-1 RAs in the treatment of T2DM-related kidney disease and tacrolimus-induced nephrotoxicity overlap with pathoetiologic mechanisms implicated with lithium-induced nephrotoxicity.18,19
In addition to being a peripheral incretin, GLP-1 is a central neuropeptide which is a cleavage product of the pre-proglucagon neurons produced in the nucleus tractus solitarius. In addition, G protein-coupled excitatory GLP-1 receptors are located in central regions subserving disparate brain functions (eg, ventral tegmental area, nucleus accumbens, hippocampus, lateral septum, hypothalamus). For example, preclinical and translational research findings indicate that GLP-1 signaling modulates reward salience, response, and learning as well as aversion and general cognitive functions. It is tempting to speculate that these aforementioned phenomenological effects reflect the molecular and cellular effects of GLP-1 RAs on neuronal plasticity, differentiation, apoptosis, neuroprotection, and autophagy.20,21
The aforementioned observations have provided the rationale for repurposing and developing GLP-1 RAs as psychiatric drugs. Results from observational, target trial emulation, Mendelian randomization, and preliminary controlled studies have reported benefits with GLP-1 RAs across multiple clinical targets including alcohol-,substance- and tobacco-use disorders, mood and psychotic disorders, binge-eating disorder, and major neurocognitive disorders. For example, preliminary controlled evidence indicates that semaglutide significantly reduces alcohol cravings, heavy drinking days, and number of drinks per drinking day in persons with alcohol-use disorder.22–25
As much of the evidence base reporting benefits across domains of psychopathology is comprised of persons whose primary diagnosis is either obesity and/or T2DM, the question arises as to whether the psychiatric benefit can be parsimoniously explained as pseudo-specific and a consequence of improvement in anthropometrics and metabolism.26–31 Although metabolic-related factors may be moderational in some persons and select conditions, they do not fully explain the improvements reported in psychopathology.21,32,33
Notwithstanding the promising preliminary data in the treatment, prevention, and/or disease modification of SMI-SUD, the evidentiary standard for efficacy has not yet been met, and mixed results have been reported in studies wherein the trial population was enrolled on the basis of having a psychiatric diagnosis. For example, controlled trials evaluating GLP-1 RAs in major neurocognitive disorders (early Alzheimer disease, Parkinson’s disease) have been mixed wherein the primary outcome has been reducing cognitive deterioration and motoric symptom intensification, respectively.34–36
Although target trial emulation and other methodologic approaches (eg, Mendelian randomization) are valid and highly suggestive of efficacy, they do not represent the foundational constructs necessary before definitive efficacy can be concluded. Currently, multiple phase 3 programs evaluating disparate GLP-1 RAs (eg, semaglutide, brenipatide [GLP-GIP agonists]) are ongoing, with results expected to appear over the next 1 to 3 years (NCT07219953, NCT07286175, NCT07412756, NCT07410507).23 Phase 3 studies are evaluating multiple mental disorders including, but not limited to, major depressive disorder, bipolar disorder, schizophrenia, alcohol-use disorder, opioid-use disorder, and binge-eating disorder.
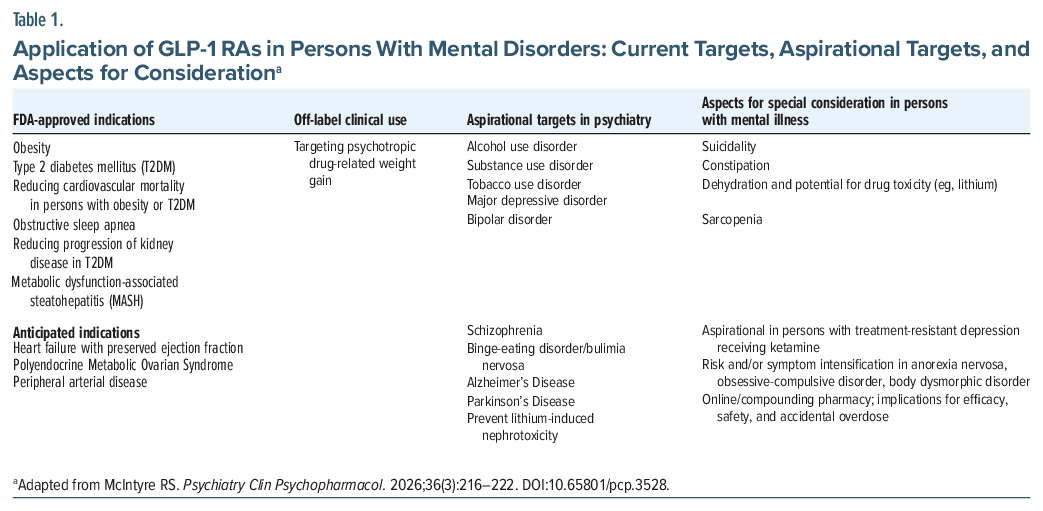
The prescription of GLP-1 RAs in persons with SMI-SUD needs to be informed by the reported safety and tolerability profiles of these agents, with some aspects of relevance to persons with SMI-SUD (Table 1). Concerns with respect to GLP-1 RAs causing suicidality have been interpreted by the FDA and other regulators (eg, European Medicines Agency) as best explained by association rather than causality.30,31,37 Notwithstanding, practitioners should continue to be vigilant for the worsening of suicidality for any persons prescribed and self-administering GLP-1 RAs.
It is well established that GLP-1 RAs slow gastric emptying, which could interact with the constipating effects of many psychotropic drugs (eg, clozapine, cogentin). In addition, GLP-1 RA–associated dehydration, which is sometimes reported, could introduce the need for more vigilant monitoring, patient education, and preventative measures in persons receiving lithium.38 Approximately 30%–40% of the weight loss in persons receiving GLP-1 RAs is due to muscle loss, which, if accompanied by impaired function, could exacerbate the risk for sarcopenia, which also occurs at a higher rate in the SMI-SUD population.39
Also, GLP-1 RAs can increase the risk for aspiration in persons receiving anesthetics, which should be considered in any individual who is receiving ketamine for difficult-to-treat psychiatric disorders, notably treatment-resistant depression.38,40,41 Persons with SMI-SUD more often are financially precarious and have inequitable access to GLP-1 RAs, which could increase the likelihood that they will seek out these agents via online pharmacies/compounding use. It is established that using online pharmacies/compounders not only introduces questionable product quality but also increases the risk for dosing errors and accidental overdose.42 An additional concern specific to the psychiatric population, notably persons with established eating disorders, is the possibility of exacerbating symptoms of anorexia nervosa as well as obsessive-compulsive behavior.25
In summary, GLP-1 RAs are evidence-based treatments for many medical conditions frequently encountered in the SMI-SUD population. Evidence also supports the prescription of GLP-1 RAs in the treatment and prevention of metabolic and weight-related alterations caused by psychotropic drugs. Although anecdotally practitioners often report a significant reduction in craving and use of alcohol, substances, and tobacco with the prescription of GLP-1 RAs, it remains aspirational as to whether these agents are definitively effective in the treatment or prevention of any psychiatric disorder.
The next 1 to 3 years will see readouts of phase 3 studies designed to address whether GLP-1 RAs are psychiatric drugs. Other priority research questions to be addressed relevant to repurposing GLP-1 RAs as psychiatric drugs include target engagement studies, CNS penetration, drug-drug interaction studies with concomitant drugs, dose-finding studies, and health systems research that endeavors to determine optimal integrated care pathways. In the interim, evidence-based prescription of GLP-1 RAs in persons with SMI-SUD holds promise to improve their health and well-being and possibly reduce the excess mortality, which is a strategic imperative in psychiatry.43,44
Article Information
Published Online: June 1, 2026. https://doi.org/10.4088/JCP.26com16484
© 2026 Physicians Postgraduate Press, Inc.
J Clin Psychiatry 2026;87(3):26com16484
Submitted: April 17, 2026; accepted April 23, 2026.
To Cite: McIntyre RS. Prescribing GLP-1 receptor agonists for persons with mental disorders: evidence-based and aspirational targets. J Clin Psychiatry 2026;87(3):26com16484.
Author Affiliations: Department of Psychiatry, University of Toronto, Toronto, Ontario, Canada; Department of Pharmacology and Toxicology, University of Toronto, Ontario, Canada.
Corresponding Author: Roger S. McIntyre, MD, FRCPC, 77 Bloor Street West, Toronto, ON Canada M5S 1M2 ([email protected]).
Relevant Financial Relationships: Dr McIntyre has received research grant support from CIHR/GACD/National Natural Science Foundation of China (NSFC) and the Milken Institute and speaker/consultation fees from Lundbeck, Janssen, Alkermes, Neumora Therapeutics, Boehringer Ingelheim, Sage, Biogen, Mitsubishi Tanabe, Purdue, Pfizer, Otsuka, Takeda, Neurocrine, Neurawell, Sunovion, Bausch Health, Axsome, Novo Nordisk, Kris, Sanofi, Eisai, Intra-Cellular, NewBridge Pharmaceuticals, Viatris, Abbvie, Bristol Myers Squibb (BMS) Teva, Adhere Tech, GH Research, Autobahn Therapeutics, and Atai Life Sciences.
Funding/Support: None.
References (44)

- Wong S, Le GH, Teopiz K, et al. Investigating the functional connectivity between central glucagon-like peptide-1 (GLP-1) and glutamatergic signaling: a systematic review. CNS Spectr. 2026;31(1):e4. CrossRef
- Drucker DJ. Efficacy and safety of GLP-1 medicines for type 2 diabetes and obesity. Diabetes Care. 2024;47(11):1873–1888. CrossRef
- Gonzalez-Rellan MJ, Drucker DJ. New molecules and indications for GLP-1 medicines. JAMA. 2025;334(14):1231–1234. CrossRef
- Breitzig MT, Trippetti TR, Kong L, et al. Prevalence of GLP-1 receptor agonist use among privately insured individuals with mood disorders. J Clin Psychiatry. 2026;87(3):26br16352.
- Jawad MY, Meshkat S, Tabassum A, et al. The bidirectional association of nonalcoholic fatty liver disease with depression, bipolar disorder, and schizophrenia. CNS Spectr. 2023;28(5):541–560. PubMed CrossRef
- McIntyre RS, Le GH. Practitioners providing care for persons with severe mental disorders should routinely screen for metabolic dysfunction-associated steatotic liver disease. J Clin Psychiatry. 2025;86(4). doi:10.4088/JCP.25com16021. CrossRef
- Liu YK, Ling S, Lui LMW, et al. Prevalence of type 2 diabetes mellitus, impaired fasting glucose, general obesity, and abdominal obesity in patients with bipolar disorder:a systematic review and meta-analysis. J Affect Disord. 2022;300:449–461. CrossRef
- Stubbs B, Vancampfort D, Veronese N, et al. The prevalence and predictors of obstructive sleep apnea in major depressive disorder, bipolar disorder and schizophrenia: a systematic review and meta-analysis. J Affect Disord. 2016;197:259–267. PubMed CrossRef
- McIntyre RS, Berk M, Brietzke E, et al. Bipolar disorders. Lancet. 2020;396(10265):1841–1856. PubMed CrossRef
- Herrman H, Patel V, Kieling C, et al. Time for united action on depression: a Lancet-World Psychiatric Association Commission. Lancet. 2022;399(10328):957–1022. PubMed CrossRef
- Forslund M, Wändell P, Forsberg L, et al. GLP-1 receptor agonist treatment in women with polycystic ovary syndrome-a systematic review and meta-analysis. Eur J Endocrinol. 2026;194(3):25–39. CrossRef
- Wong S, Le GH, Lo HKY, et al. Suicide risk in persons with polycystic ovarian syndrome: a systematic review. Ann Gen Psychiatry. 2025;24(1):38. CrossRef
- McIntyre RS, Kwan ATH, Rosenblat JD, et al. Psychotropic drug-related weight gain and its treatment. Am J Psychiatry. 2024;181(1):26–38. CrossRef
- Ganeshalingam AA, Uhrenholt N, Arnfred S, et al. Semaglutide effects on insulin sensitivity and β-cell function in patients with schizophrenia, prediabetes, and obesity treated with second-generation antipsychotics: findings from the HISTORI trial, a 30-week randomized, placebo-controlled trial with semaglutide 1.0 mg weekly. Diabetes Care. 2026:dc252041.
- Sass MR, Klausen MK, Schwarz CR, et al. Semaglutide and early-stage metabolic abnormalities in individuals with schizophrenia spectrum disorders: a randomized clinical trial. JAMA Psychiatry. 2026;83(2):128–138. CrossRef
- Mansour MEM, Alsaadany KR, Mustafa MMM, et al. Efficacy and safety of pharmacological and non-pharmacological interventions for antipsychotic-induced weight gain in individuals with schizophrenia: a systematic review and network meta-analysis of 55 clinical trials. J Psychopharmacol. 2025(02698811251399544):2698811251399544.
- Daggolu J, Chen H. Effect of concurrent metformin on adherence to and persistence of treatment with second-generation antipsychotics in nondiabetic patients. J Clin Psychiatry. 2025;87(1). doi:10.4088/JCP.25m15808. PubMed CrossRef
- Abdelhady R, Arab HH, Fakhr Eldeen RR, et al. Unveiling the therapeutic potential of dulaglutide in mitigating tacrolimus-induced nephrotoxicity through targeting the miR-22/HMGB-1/TLR4/MyD88/NF-κB trajectory. Arch Pharm Weinh. 2025;358(4):e3127. PubMed CrossRef
- McIntyre RS, Kwan ATH. Potential protective role of GLP-1 receptor agonists for lithium-induced nephrotoxicity: a population-based observational study. CNS Spectr. 2025;31(1):e5. CrossRef
- Sioufi MC, Heroiu I, Wong S, et al. The effect of GLP-1 receptor agonists on autophagy: insights gathered from research evaluating neurodegenerative disorders with these agents. Acta Neuropsychiatr. 2026:1–36. Published online February 13.
- McIntyre RS, Rasgon N, Goldberg JF, et al. The effect of glucagon-like peptide-1 and glucose dependent insulinotropic polypeptide receptor agonists on neurogenesis, differentiation and plasticity: potential mechanistically-informed therapeutics in the treatment and prevention of mental disorders. CNS Spectr. 2025;18:1–25. Published online February.
- Wang W, Volkow ND, Berger NA, et al. Association of semaglutide with reduced incidence and relapse of cannabis use disorder in real-world populations: a retrospective cohort study. Mol Psychiatry. 2024;29(8):2587–2598. CrossRef
- Hendershot CS, Bremmer MP, Paladino MB, et al. Once-weekly semaglutide in adults with alcohol use disorder: a randomized clinical trial. JAMA Psychiatry. 2025;82(4):395–405. CrossRef
- Yammine L, Green CE, Kosten TR, et al. Exenatide adjunct to nicotine patch facilitates smoking cessation and may reduce post-cessation weight gain: a pilot randomized controlled trial. Nicotine Tob Res. 2021;23(10):1682–1690. CrossRef
- Zhang L, Chen X, Xu Y, et al. Exploring glucagon-like peptide-1 receptor agonists as potential disease-modifying agent in psychiatric and neurodevelopmental conditions: evidence from a drug target Mendelian randomization. BMC Psychiatry. 2025;25(1):484. CrossRef
- Li S, Sabbah SG, Kwan ATH, et al. Repurposing glucagon-like peptide-1 (GLP-1) receptor agonists for the treatment of depression: a systematic review of preclinical, observational and clinical investigations. Eur Neuropsychopharmacol. 2025;99:56–67. CrossRef
- Zheng X, Wang H, Liu P, et al. Investigating the association between GLP-1 receptor agonists and mood disorders: a study integrating real-world data and Mendelian randomization. Eur Psychiatry. 2025;69(1):e6. CrossRef
- Kerem L, Stokar J. Risk of suicidal ideation or attempts in adolescents with obesity treated with GLP1 receptor agonists. JAMA Pediatr. 2024;178(12):1307–1315. CrossRef
- Yi YT, Zheng YJ, Bargiota SI, et al. The effect of GLP-1 receptor agonists on anxiety: a systematic review. Psychoneuroendocrinology. 2026;188:107844. CrossRef
- Au HCT, Zheng YJ, Le GH, et al Association of glucagon-like peptide-1 receptor agonists and suicidality: a systematic review. Obes Rev. 2026:e70120.
- McIntyre RS. Glucagon-like peptide-1 receptor agonists and suicidality: association versus causation and the need for ongoing surveillance. Am J Psychiatry. 2025;182(12):1038–1046. CrossRef
- van Bruggen FH, McIntyre RS. Neuroinflammation and insulin resistance in major depression and bipolar disorder: implications for clinical trials evaluating immunometabolic targeted therapies. Brain Behav Immun Health. 2026;51:101166. PubMed CrossRef
- Volkow ND, Xu R. GLP-1 receptor agonists in psychiatry: a pharmacoepidemiological scoping review. Biol Psychiatry. 2026. doi:10.1016/j.biopsych.2026.03.1002. CrossRef
- Cummings JL, Atri A, Sano M, et al. Efficacy and safety of oral semaglutide 14 mg (flexible dose) in early-stage symptomatic Alzheimer’s disease (evoke and evoke+): two phase 3, randomised, placebo-controlled trials. Lancet. 2026. doi:10.1016/S0140-6736(26)00459-9. CrossRef
- Vijiaratnam N, Girges C, Auld G, et al. Exenatide once a week versus placebo as a potential disease-modifying treatment for people with Parkinson’s disease in the UK: a phase 3, multicentre, double blind, parallel-group, randomised, placebo-controlled trial. Lancet. 2025;405(10479):627–636. CrossRef
- Edison P, Femminella GD, Ritchie C, et al. Liraglutide in mild to moderate Alzheimer’s disease: a phase 2b clinical trial. Nat Med. 2026;32(1):353–361. CrossRef
- Taipale H, Taylor M, Lähteenvuo M, et al. Association between GLP-1 receptor agonist use and worsening mental illness in people with depression and anxiety in Sweden: a national cohort study. Lancet Psychiatry. 2026;13(4):327–335. PubMed CrossRef
- Nagamine T. Challenges of constipation in people suffering from schizophrenia: a narrative review. Clin Pract. 2025;15(2):33. CrossRef
- Kwan ATH, Lakhani M, McIntyre RS. Muscle atrophy associated with glucagon-like peptide-1 receptor agonists: a population-based observational study. Clin Nutr. 2026;60(106620):106620. PubMed CrossRef
- Bulbul F, Tamam L, Demirkol ME, et al. The prevalence of sarcopenia in patients with schizophrenia. Psyc Clin Psychopharmacol. 2021;31(1):60–66. CrossRef
- Davila Diaz R, Campos Barrera E, Diaz Fosado LA, et al. Glucagon-like peptide-1 receptor agonists in plastic surgery: perioperative considerations and safety protocols. Cureus. 2025;17(12):e99865.
- Mattingly TJ 2nd, Conti RM. Marketing and safety concerns for compounded GLP-1 receptor agonists. JAMA Health Forum. 2025;6(1):e245015. CrossRef
- Wagner E, Højlund M, Fiedorowicz JG, et al. Disparities in diabetes treatment and monitoring for people with and without mental disorders: a systematic review and meta-analysis. Lancet Psychiatry. 2026;13(2):112–124. CrossRef
- McIntyre RS. Glucagon-like peptide-1 receptor agonists (GLP-1 RAs) have potential to transform health outcomes for persons with bipolar disorder, schizophrenia, major depressive disorder and other serious mental illnesses by lengthening healthspan and reducing excess and premature mortality. Expert Opin Pharmacother. 2026;27(1):1–3. CrossRef
This PDF is free for all visitors!




