Lessons Learned at the Interface of Medicine and Psychiatry
The Psychiatric Consultation Service at Massachusetts General Hospital sees medical and surgical inpatients with comorbid psychiatric symptoms and conditions. During their twice-weekly rounds, Dr Stern and other members of the Consultation Service discuss diagnosis and management of hospitalized patients with complex medical or surgical problems who also demonstrate psychiatric symptoms or conditions. These discussions have given rise to rounds reports that will prove useful for clinicians practicing at the interface of medicine and psychiatry.
Prim Care Companion CNS Disord 2026;28(3):25f04133
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Have you ever wondered how you can screen for and diagnose an alcohol use disorder (AUD) in your patients? Have you been reluctant to embark upon such screening for fear of embarrassing your patients with your inquiries, of getting into a domain in which you feel less than competent, or of not knowing which resources would be most readily available and helpful? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Mrs A, a 32-year-old married Hispanic woman, appeared fatigued during a routine pediatric visit for her 3-year-old daughter. She shared that she had been feeling increasingly overwhelmed due to carrying the bulk of parenting and household responsibilities (while also working remotely from home and providing childcare to neighboring families), since her husband works long hours in construction and is often unable to help.
When she was asked about her coping strategies, Mrs A mentioned that she and her husband typically drink 1 or 2 beers together every evening to unwind. After putting her daughter to bed, she may have another drink to “take the edge off.” On weekends when her husband is not working, she frequently consumes 3–4 beers throughout the day. She denied daytime drinking during the workweek or missing any responsibilities, although she admitted to occasionally feeling sluggish in the mornings. She acknowledged that she may be relying on alcohol “more than she should” but had not spoken to any health care provider about it before.
She hesitated before adding that the cost of alcohol had started to strain their already tight household budget. She also expressed concern that the parents of the children she cares for might smell alcohol on her breath, which could jeopardize her livelihood. Supportive comments were provided, and the CAGE (cut down, annoy, guilt, eye-opener) questionnaire was administered. Mrs A reported that she had considered cutting back on her drinking and that she occasionally felt guilty about how much she drank. Given that her visit took place in a family practice setting with her daughter (who was in good health), Mrs A agreed to further screening through the clinic’s screening, brief intervention, and referral to treatment services. She was reassured to learn that the clinic had walk-in behavioral health support, including credentialed alcohol and substance abuse counselors (CASACs). Within 30 minutes, she was seen by a CASAC, who began a supportive conversation about alcohol use, sources of stress, and available resources for moving forward.
DISCUSSION
What Are the Criteria for an AUD?
Historically, alcohol-related conditions have been described using terms like alcoholism, alcohol abuse, and alcohol dependence—terminology that is now considered outdated and stigmatizing. In early editions of the Diagnostic and Statistical Manual of Mental Disorders (DSM), abuse and dependence were treated as distinct diagnoses1; the former often tied to social consequences and the latter to compulsive use. However, by 1994, when the DSM-IV was published, this binary framework was increasingly criticized for its stigmatizing language, lack of nuance, and clinical overlap.1 To address these concerns, the DSM-5 consolidated several categories into a single diagnosis: AUD, which reflected a spectrum of severity (from mild to severe) and embraced more person-centered, nonstigmatizing language.2
AUD is characterized by a pattern of problematic alcohol use that leads to significant distress or impairment in functioning, loss of control over consumption, involvement in risky behaviors, and continued use despite its negative consequences. Individuals may struggle to meet responsibilities, experience interpersonal conflicts related to their drinking, and develop physiological signs (eg, increased tolerance or withdrawal symptoms). AUD is diagnosed when individuals meet at least 2 of the 11 criteria within a 12-month period. The number of criteria present determines the severity: 2–3 symptoms indicate a mild AUD, 4–5 a moderately severe condition, and 6 or more a severe condition. For a more complete description of the diagnostic criteria and for additional resources, readers can refer to the National Institute on Alcohol Abuse and Alcoholism (NIAAA) Healthcare Professional’s Core Resource on Alcohol.3
Which Screening Tools Can Identify a Person at Risk for an AUD?
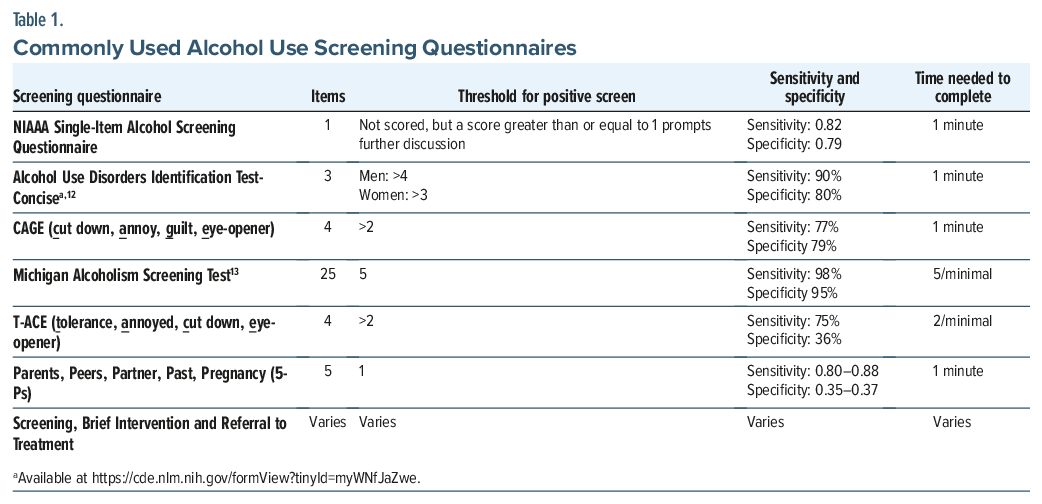
Given variability in clinical settings, visit length, and patient readiness, alcohol screening can be flexibly conducted using a stepped approach, beginning with brief prescreening questions and progressing to validated instruments as indicated. An initial prescreening question such as “How often have you had a drink containing alcohol in the past year?” may be used to open a brief clinical conversation. The NIAAA Single Alcohol Screening Question, “How many times in the past year have you had 4 or more (for women) or 5 or more (for men) drinks in a day?” can then be easily integrated into a routine clinical interview.4
Other validated screening tools for the detection of AUDs include the Alcohol Use Disorders Identification Test-Concise (AUDIT-C) and the CAGE Questionnaire. The AUDIT-C consists of 3 questions assessing frequency and quantity of alcohol use (eg, “How often do you have a drink containing alcohol?”) and is freely available through the National Library of Medicine National Institutes of Health Common Data Elements Repository,5 whereas the CAGE questionnaire comprises 4 lifetime questions focused on problematic use (eg, Have you ever felt you should cut down on drinking?”), with even a single positive response considered a positive screen.6 Both the AUDIT-C and the CAGE rapidly and effectively screen for AUDs with a high degree of accuracy and predictability.6
Additional screeners tailored to specific populations include the Tolerance, Annoyed, Cut down, Eye-opener (T-ACE), which adds an assessment for tolerance.7 Both the T-ACE and the Parents, Peers, Partner, Past, Pregnancy (5-Ps) focus on the diagnosis of AUDs in pregnant women.7,8 For ease of clinical implementation, Table 1 summarizes commonly used AUD screening tools and provides primary citations and direct weblinks to freely available versions, allowing clinicians to readily access full instruments and scoring guidance.5,7,9–13 Additional validated screening instruments, implementation guidance, and tools that require licensing or fees are available through NIDAMED Clinical Resources.14
Who Is at Risk for AUD?
The risk of developing AUD is cumulative and multifactorial, involving a combination of genetic, environmental, and psychological factors.
Sex
AUD has a higher prevalence in men; however, the number of AUD diagnoses in women is increasing. Women tend to progress more quickly to severe stages of AUD. Additionally, women are more susceptible to medical complications related to alcohol use, such as breast cancer, cardiac complications, and alcohol-related liver disease.15
Genetic Risk Factors
A family history of AUD is a significant risk factor for the development of the disorder. Studies show that approximately 50% of the risk for developing AUD is genetic.16 Large-scale genome-wide association studies have identified key genetic loci associated with alcohol metabolism, including the ADH1B*2 variant (alcohol dehydrogenase) and the ALDH2*2 variant (acetaldehyde dehydrogenase).17 These genetic variations are commonly present in East Asian populations and lead to aversive reactions to alcohol, serving as protective factors against the development of AUD.
Additionally, genetic variants in neurotransmission loci, such as γ-aminobutyric acid receptor subunit α-2, have been linked to an increased risk for AUD, while opioid receptor μ 1 is associated with alcohol-induced euphoria and may influence susceptibility to AUD. Stress-related loci such as corticotropin-releasing hormone receptor 1, which are involved in stress and emotional regulation, have also been identified as risk loci for AUD.18–20 Studies suggest that the highest risk for AUD arises from a combination of genetic vulnerability, family history, and cumulative alcohol exposure.21
Social Determinants of Health
Social determinants of health play a major role in the morbidity and mortality of alcohol use, with lower socioeconomic groups bearing the most burden. The risks are primarily due to higher stress levels, including a higher prevalence of childhood trauma—which is a major risk factor for the development of AUD, as discussed below—and less access to health care.22
Childhood Adversity
Early-life adversity, including trauma, neglect, and resource scarcity, is a well-established risk factor for the development of addiction later in life. Chronic hypothalamic-pituitary axis upregulation alters the response to stress and increases the risks of AUD. Evidence from both human and rodent models suggests that childhood adversity alters stress and reward circuits, increasing susceptibility to addiction-related behaviors.23
Onset of Alcohol Consumption
The early initiation of alcohol use, particularly during adolescence when the brain is still developing, significantly increases the risk of AUD.24 The developing brain is more vulnerable to alcohol’s neurotoxic effects, which can alter reward pathways and impulse control, increasing the likelihood of long-term alcohol dependence.
Social vs Isolation
Societal trends, the glamorization of alcohol consumption on social media and TV, along with peer pressure and the desire to fit in, may predispose individuals to increased alcohol consumption. Moreover, Creswell25 highlighted the importance of the context in which drinking occurs, noting that social drinking is often linked to positive emotions, whereas drinking alone is more commonly associated with coping with negative emotions. The association of improved mood and social experiences with alcohol consumption carries an additional risk for developing AUD, while solitary drinking is primarily driven by the desire to mitigate negative affective states. A study conducted during the COVID-19 pandemic found that consuming alcohol in isolation was associated with an increased risk of progressing to AUD.26
Co-occurring Psychiatric Conditions
Another critical risk factor for AUD is the presence of co-occurring psychiatric disorders. Many psychiatric conditions co-occur with AUD, particularly those involving dysregulation of stress and fear-related neural circuits, reward system dysfunction, and impulsivity. Deficits in cognitive control, especially in individuals with heightened impulsivity and emotional dysregulation (eg, post-traumatic stress disorder, attention-deficit/hyperactivity disorder [ADHD], unipolar and bipolar depressive disorders, and anxiety disorders), further increase the risk of developing AUD.27
Among these, anxiety disorders are one of the most common comorbidities of AUD, reflecting shared neurobiological disruptions in inhibitory (GABAergic), excitatory (glutamatergic), and stress-regulation systems.28,29 Chronic alcohol exposure transiently enhances GABAergic inhibition and suppresses glutamatergic signaling; however, repeated withdrawal produces a rebound state marked by glutamatergic hyperexcitability and activation of brain stress systems including corticotropin-releasing factor and noradrenergic pathways.29 This neuroadaptation results in heightened anxiety and hyperarousal and provides a mechanistic rational for pharmacologic strategies that target hyperexcitability, impaired inhibitory control, and stress responsivity in AUD.29 Self-medicating anxiety with alcohol may provide temporary relief but ultimately reinforces this negative affect state and anxiety symptoms, perpetuating a pathophysiological loop through dysregulation of stress and fear circuitry.
Studies have shown that patients with major depressive disorder (MDD) and comorbid AUD often present with more severe symptoms, including suicidal ideation, personality disorders, and higher rates of smoking.30 Additionally, Cluster B personality disorders (eg, borderline and antisocial personality disorders) have been linked to higher rates of AUD. However, there is a shift away from assuming that personality traits are a direct cause of AUD, as such associations can perpetuate stigma and shift blame for a condition influenced by multiple biological and environmental factors.
Psychiatric disorders (such as schizophrenia, MDD, and personality disorders) frequently co-occur with AUD (eg, schizophrenia at 33.7%, MDD at 28%, and personality disorders at 50%–70%).31 The cognitive dysfunction and impulsivity seen in conditions like ADHD make these individuals more vulnerable to AUD, with up to 43% of individuals with ADHD developing AUD. Screening for ADHD in AUD patients is recommended, as ADHD symptoms such as impulsivity and a maladaptive reward system heighten the risk of alcohol misuse. Routine screening and early intervention are crucial for better treatment outcomes.32
How Can You Facilitate a Patient’s Acceptance for Help in Cutting Down or Stopping Alcohol Use?
Given the widespread stigma and associated shame, one of the most important aspects of engaging a patient with AUD is creating a sense of safety and comfort that allows the patient to accept help. Using a nonjudgmental approach and building therapeutic rapport are crucial, as evidence shows that these factors improve outcomes. Avoiding stigmatizing terminology and instead using person-first, nonstigmatizing language—such as “a patient with AUD” rather than terms such as alcoholic or drunk, or return to drinking rather than relapsing—is essential and helps to reduce stigma within the health care system.33 Framing questions in neutral, collaborative terms (eg, “Can you tell me about how alcohol fits into your life right now?”) further reinforces trust and openness.33
The concept of active listening, being attentive and fully present with the patient, using open-ended questions, reflecting, summarizing, and seeking to understand, plays a key role in this process.34,35 One of the tools with the strongest evidence for helping patients is motivational interviewing, a standardized behavioral intervention that explores a patient’s personal motivation for change.36,37 Exploring goals and values is a key part of this process. Motivational interviewing is based on the understanding that a patient’s goals and values may not always align with those of the clinician. By exploring ambivalence regarding alcohol use, motivational interviewing helps patients identify internal reasons for change.
Understanding ambivalence and the stages of change—precontemplation, contemplation, preparation, action, and maintenance—is an important part of the process.38 Using curiosity and a nonjudgmental stance, clinicians are invited to understand the reasons for and against change from the patient’s perspective and to leverage the patient’s strengths. Another important aspect of engaging patients in care is referral to peer support specialists—individuals who share personal experience with recovery and can provide understanding, encouragement, and hope.39
What Complications Are Associated With Acute Alcohol Intoxication, and How Can They Be Managed?
Primary care clinicians may encounter patients with acute alcohol intoxication during routine visits or urgent evaluations. Recognition is critical, as intoxication can range from mild impairment to life-threatening conditions requiring urgent referral. Presentations may be subtle, atypical, or disproportionate to reported alcohol intake, particularly in patients with tolerance, polysubstance use, or ingestion of nonbeverage alcohols (eg, methanol). Clinicians should also ask about potential nonbeverage or surrogate alcohol exposure (eg, “Have you consumed anything other than beverage alcohol—such as hand sanitizer, mouthwash, antifreeze, or rubbing alcohol?”), particularly when symptoms are severe, atypical, or accompanied by unexplained metabolic abnormalities.
Targeted history should include the quantity and timing of alcohol use, physical and neurological symptoms, and concurrent use of benzodiazepines, opioids, or stimulants. Discrepancies between reported intake and clinical severity should heighten concern. When available, laboratory evaluation may aid in risk stratification and identification of atypical intoxication. Useful studies include blood glucose, comprehensive metabolic panel (with attention to bicarbonate and anion gap, osmolar gap), serum ethanol level, magnesium, and liver enzymes. Findings such as hypoglycemia, significant electrolyte abnormalities, or anion gap metabolic acidosis should prompt concern for coingestion or surrogate alcohol exposure and warrant urgent evaluation.
Phosphatidylethanol (PEth) is a highly specific blood biomarker formed only in the presence of ethanol and reflects moderate to heavy alcohol use over the prior 2–3 weeks.40 Elevated PEth levels support recent sustained alcohol exposure and may be particularly useful when patients minimize intake, when monitoring treatment response, or when clarifying risk in medically vulnerable populations (eg, liver disease, preoperative evaluation). Other biomarkers include carbohydrate-deficient transferrin, which reflects sustained heavy drinking over weeks, and nonspecific markers such as γ-glutamyl transferase and mean corpuscular volume, which may support chronic alcohol exposure when interpreted in clinical context.40 Ethyl glucuronide and ethyl sulfate detect very recent alcohol use (hours to days) but are prone to false positives from incidental exposures and should be used cautiously.40
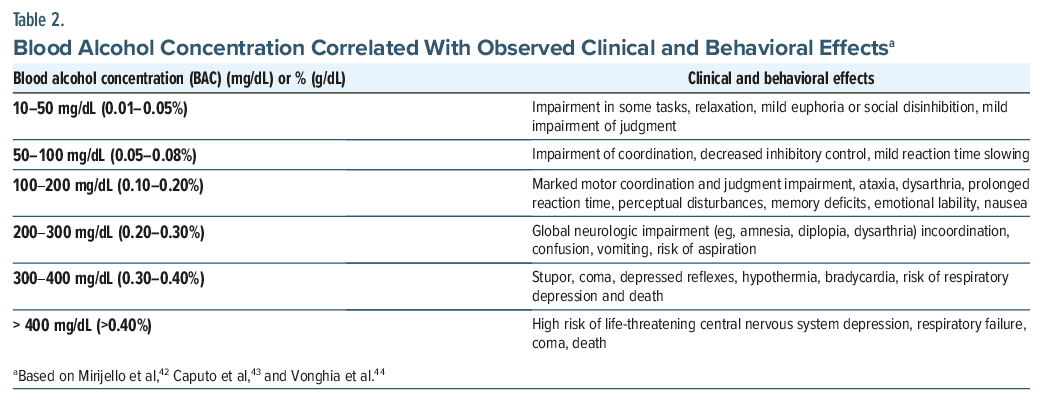
Alcohol intoxication is a common but potentially life threatening condition that resulted in over 3.2 million alcohol-related emergency department (ED) visits in the United States in 2024,41 which represented 1.2% of total visits.42 The most common alcohol use pattern associated with alcohol intoxication was binge drinking.42 Acute alcohol intoxication may present with myriad physiological disturbances, ranging from mild euphoria to life-threatening complications that depend on the quantity ingested, the individual’s tolerance, and concurrent use of other substances, roughly correlating with blood alcohol concentration (Table 2).43,44
The most significant complications involve the neurological, respiratory, cardiovascular, metabolic, and thermoregulatory systems.42 Central nervous system (CNS) effects include delirium, stupor, and coma due to alcohol’s enhancement of GABA activity and inhibition of N-methyl-D-aspartate receptors, though seizures or central pontine myelinolysis may also occur.42 Respiratory depression or arrest may occur from suppression of the brain stem respiratory centers, leading to hypoventilation and hypoxia. Cardiovascular effects include arrhythmias as well as hypotension caused by peripheral vasodilation that can lead to shock. Alcohol inhibits gluconeogenesis, leading to hypoglycemia, confusion, seizures, or coma.43 Hypothermia occurs due to systemic vasodilation and impairment of the HPA axis. Alcohol is a gastrointestinal (GI) irritant, and direct inflammation can lead to vomiting with subsequent aspiration pneumonia, pancreatitis, Mallory-Weiss tears, and gastritis.42 Metabolic abnormalities, such as acidosis, hypoalbuminemia, and electrolyte disturbances (ie, hyponatremia, hypokalemia, hypomagnesemia, hypocalcemia, and hypophosphatemia), are also common and should be screened and corrected.42,45 Further, patients with acute intoxication are at a higher risk of experiencing psychological trauma and would benefit from screening and referral to treatment, if indicated.
Management of severe acute alcohol intoxication focuses on supportive care, protecting the airway, and preventing complications. Initial priorities include airway protection, supplemental oxygen, continuous pulse oximetry, and hemodynamic stabilization.42 Aspiration risk must be considered in any patient with vomiting and an altered mental status, and patients with absent gag reflex may require endotracheal intubation to protect their airways. Hypotension should be treated initially with intravenous (IV) fluids, with vasopressors (eg, norepinephrine) reserved for cases unresponsive to fluids. Recommendations from the American Academy of Emergency Medicine do not support routine administration of fluids to hydrate patients.45 Blood glucose should be checked upon arrival, and hypoglycemia should be corrected with IV dextrose.43 High-dose IV thiamine should be administered prior to glucose administration to prevent the development of Wernicke encephalopathy. Electrolyte abnormalities, such as hypokalemia, hypomagnesemia, and metabolic acidosis, should be corrected, with careful monitoring of cardiac rhythm due to the risk of arrhythmias (ie, “holiday heart syndrome”).43 Hypothermia should be treated by rewarming. In severe cases, admission to the intensive care unit may be warranted, particularly for patients with respiratory depression, hemodynamic instability, significant metabolic derangements, or coma.
Risks and Management of Surrogate Alcohol Ingestion
The ingestion of surrogate alcohols (ie, methanol, ethylene glycol, and isopropyl alcohol) poses unique challenges. These substances, sometimes consumed in settings of alcohol scarcity, are metabolized by alcohol dehydrogenase and aldehyde dehydrogenase into dangerous metabolites. Methanol is metabolized to formaldehyde and subsequently formic acid, which causes metabolic acidosis, retinal toxicity, and blindness.46 Ethylene glycol is converted into oxalic acid by aldehyde dehydrogenase, which results in acute kidney injury and severe acidosis.47 Isopropyl alcohol, although not metabolized to a toxic acid, leads to profound CNS depression and hemorrhagic gastritis.48 The management of surrogate alcohol ingestion differs significantly from that of ethanol intoxication and often requires therapy with fomepizole for methanol and ethylene glycol, correction of acidosis, and consideration of hemodialysis to dialyze both the alcohol and its metabolites.46–48
Risks and Management of Polysubstance Use
Coingestion of alcohol with other substances is seen in 20% of alcohol-related presentations to the ED and significantly increases morbidity and mortality, so taking a substance use history and checking a urine drug screen are beneficial.41 Benzodiazepines can have a synergistic effect with alcohol, leading to more profound respiratory depression, sedation, and coma than either substance alone. In contrast, when cocaine is combined with alcohol, the liver metabolizes both into cocaethylene. Cocaethylene is similar in psychoactive effects to cocaine but with a longer half-life and increased cardiotoxicity and hepatotoxicity.49 Cocaethylene significantly increases the risk of arrhythmias, myocardial infarction, and sudden cardiac death.50 Patients who present with coingestions may exhibit an unpredictable clinical course, requiring additional monitoring and interventions.
What Medical and Neurologic Sequelae Are Associated With Chronic and Severe Alcohol Use, and Why Do They Develop?
Gastrointestinal. Certain medical conditions and interventions can also increase vulnerability to AUD, including bariatric surgery, which alters alcohol absorption, metabolism, and reward sensitivity, leading to higher peak blood alcohol concentrations and increased risk of problematic use.51 In addition, alcohol consumption can damage the entire GI tract, starting with the oral cavity (eg, with salivary gland hypertrophy, esophageal dysmotility, gingival disease, esophageal mucosa degradation and bleeding) and progressing throughout the gut. Weakening of the esophageal sphincter increases risk of gastroesophageal reflux disease, disruptions of the normal esophageal mucosa, Barrett esophagus, Mallory-Weiss syndrome, and the risk of aspiration. Chronic consumption of alcohol is associated with an increased risk of bleeding and associated gastric mucosa damage, bacterial colonization, and a higher risk for infection.52
When the intestinal mucosa is damaged, nutrients are inadequately absorbed, bacterial toxins accumulate, and the risk of GI bleeding rises. Uptake of some macromolecules is reduced, due to delayed motility and malnutrition. Those with chronic alcohol use often develop vitamin deficiencies (eg, thiamine, B12, folic acid) leading to pernicious anemia.52
Alcohol is metabolized through oxidative (eg, via alcohol dehydrogenase, peroxisomal catalase, and microsomal cytochrome P450 enzymes) and nonoxidative pathways. Acetaldehyde, a byproduct of alcohol metabolism, is highly reactive and compromises the normal cell function of cellular proteins, nucleic acids, and lipids. In low concentrations, acetaldehyde is quickly converted to less toxic acetate via aldehyde dehydrogenase.53
Among those who routinely drink alcohol, there is often increased expression and activity of CYP 2 × 101, a leaky cytochrome responsible for the conversion of ethanol to acetaldehyde in the presence of a high concentration of ethanol. Subsequent metabolism of ethanol leads to an excess of reactive oxygen species (ROS), even when the substrate is not present. Acetaldehyde and ROS lead to cellular damage that is worsened by alterations in the immune system and gut microbiota. Damaged cellular material (eg, proteins, nucleic acids, lipids) begins to accumulate in hepatocytes, which leads to impaired cellular function and activation of induction pathways (with unfolding of proteins or an endoplasmic reticulum stress response). If the hepatocyte’s stress response is insufficient, pathways for cell death are activated.53
Alcohol-associated liver disease is comprised by a spectrum of hepatic conditions that progress from fatty liver disease to fibrosis, alcoholic hepatitis, nonviral cirrhosis, and hepatocellular carcinoma. Approximately 8%–20% of those who drink alcohol chronically will develop alcohol-related cirrhosis with 2% of them developing hepatocellular carcinoma.53
Individuals with alcohol-induced acute liver failure may present with jaundice, portal hypertension, and ascites (along with impairments in gluconeogenesis, synthesis of vitamin K-dependent factors, coagulation factors, and lactic acid degradation). Moreover, an individual may present with acute encephalopathy, either secondary to alcohol withdrawal or hyperammonemia. GI bleeding is common secondary to esophageal varices and Mallory-Weiss tears. High output cardiac failure, hepatorenal syndrome, hepatopulmonary syndrome, and portopulmonary syndrome can also be observed in those who drink alcohol on a chronic basis.52
Alcohol is also one of the most common risk factors for the development of acute pancreatitis. Although its etiology is unknown, speculation about its cause has included an inflammatory cascade secondary to cell death from acetaldehyde and ROS.52
Renal
As the hepatic system begins to fail, urine becomes more acidic, with the development of hyperkalemia, hyperphosphatemia, and an elevated creatinine level. Hyponatremia is not uncommon, secondary to free-water ingestion and poor free-water excretion.52
Neurologic
Thiamine serves an integral role in various brain stem and cerebellar processes. Chronic alcohol use can reduce thiamine’s ability to cross the intestinal wall, which leads to a thiamine deficit in the brain stem and cerebellum. Wernicke-Korsakoff syndrome, a neurological manifestation of thiamine deficiency, often arises in those who drink alcohol excessively, with peripheral neuropathy, encephalopathy, a gait imbalance, psychosis, and memory loss.52 Wernicke encephalopathy usually presents acutely (ie, over the course of days to weeks), and it is notable for a cognitive disorder, opthalmoparesis, and gait ataxia. Korsakoff syndrome presents with anterograde amnesia, confabulation, and retrograde amnesia.54
Cognitive impairment and dementia may also arise in the absence of micronutrient deficiencies among those who drink chronic alcohol excessively, a presentation often conceptualized as alcohol-related neurocognitive disorder (ARND). ARND can present with prominent executive dysfunction, memory impairment, and slowed processing speed and may be misattributed to primary neurodegenerative disease if alcohol history is not carefully assessed. These manifestations are thought to be related to alcohol binges that impact GABA-mediated inhibition and glutamatergic excitation, which leads to loss of hippocampal and neocortical neurons.54
Sleep and Circadian Disruption
Acute and subacute alcohol use has predictable but often misunderstood effects on sleep architecture. Alcohol initially shortens sleep onset latency and increases slow-wave sleep (SWS) during the first half of the night via GABA-A–mediated sedation; however, as blood alcohol levels fall and acetaldehyde accumulates, sleep becomes fragmented, with reduced SWS, rapid eye movement (REM) suppression, and increased awakenings later in the night driven by autonomic activation.55 These effects contribute to nonrestorative sleep and circadian disruption, even when total sleep time appears preserved.
Chronic Insomnia and Relapse Risk
With chronic AUD, sleep disturbances often persist well into abstinence and are characterized by sustained reductions in SWS and altered REM regulation.55 Persistent insomnia is clinically significant, as patients may attempt to self-treat sleep disturbance with alcohol, increasing relapse risk. Chronic reductions in SWS may also impair glymphatic clearance and contribute to cognitive vulnerability. While low doses of alcohol may transiently enhance glymphatic function, higher or chronic exposure suppresses glymphatic activity and is associated with cognitive decline, paralleling patterns observed in ARND.56
Evidence-based interventions available in primary care, including cognitive-behavioral therapy for insomnia, mindfulness-based approaches, and pharmacologic strategies (such as use of acamprosate), may improve sleep and reduce relapse risk.
Cardiovascular
Cardiac complications of AUD include hypertension, atrial fibrillation, and high-output heart failure. Sympathetic discharges increase due to high cortisol levels along with alcohol’s stimulation of vasoconstrictors (endothelin 1 and 2, norepinephrine, angiotensin II), though the underlying mechanisms are incompletely understood.52
Heart failure secondary to alcohol use presents as high-output heart failure or as a dilated cardiomyopathy, likely secondary to an underlying thiamine deficiency with elevated levels of ROS. Since thiamine serves a pivotal role in facilitating adenosine triphosphate production (ATP), a deficiency in thiamine leads to less ATP production, which reduces the systemic vascular resistance and augments venous return, thereby producing a state of high-output heart failure. An underlying thiamine deficiency can also present as wet beriberi, which leads to shortness of breath, tachycardia, right heart failure, acidosis, and ankle swelling.52
Atrial fibrillation corresponds to increased alcohol-mediated adrenal secretions, oxidative stress, toxic metabolites, and increased circulating levels of norepinephrine and epinephrine. Comorbid conditions associated with AUD include obstructive sleep apnea (OSA), hypertension, and obesity and increase the risk of developing atrial fibrillation.52
Pulmonary
Although AUD does not cause pulmonary complications, it magnifies the risk associated with the development of pulmonary-related complications. AUDs are associated with a higher risk of intubation and mechanical ventilation in those receiving critical care. Gingivodental disease, aspiration risks, and colonization of the oropharynx, each of which is associated with alcohol use, worsen the risk for ventilator-associated pneumonias, with AUDs doubling the risk of developing acute respiratory distress syndrome. Outside of critically ill patients, individuals with AUD are more likely to develop OSA with apnea and snoring episodes becoming more common as the quantity of alcohol use increases.52
What Additional Resources Are Available to Providers, Patients, and Their Family Members Regarding AUDs?
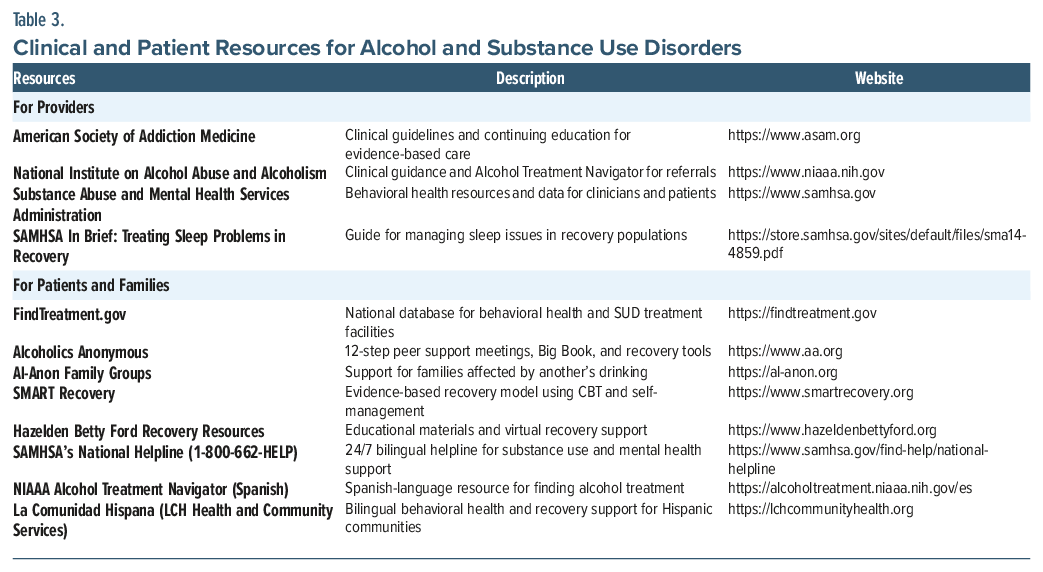
Several professional and governmental organizations provide valuable educational and clinical resources to support the identification and management of AUD. The NIAAA offers evidence-based clinical guidance and the Alcohol Treatment Navigator to help providers and patients locate quality and care. The Substance Abuse and Mental Health Services Administration provides a wide range of behavioral health tools, including the National Helpline (1-800-662-HELP), which offers 24/7 bilingual support, and findtreatment.gov, a national director of behavioral health and addiction treatment facilities. Peer support resources such as Alcoholics Anonymous and Al-Anon Family Groups also offer free, 12-step community-based recovery and family support. Spanish-language resources, including the NIAAA Alcohol Treatment Navigator (Espanol) and La Comunidad Hispana, further enhance accessibility for Hispanic and bilingual populations. These and other resources are summarized in Table 3.
What Happened to Mrs A?
Following her brief intervention, Mrs A engaged in ongoing counseling with the CASAC and was referred to a virtual outpatient program that allowed her to attend sessions from home while caring for her daughter and providing childcare to neighboring families. She appreciated the flexibility and privacy this offered, which made it easier to maintain consistency with treatment. Over the next several weeks, she worked to identify triggers for her drinking and develop healthier coping strategies, including structured daily routines and mindfulness-based stress management.
In collaboration with the addiction psychiatry provider, Mrs A began naltrexone 50 mg daily, reporting a noticeable reduction in alcohol cravings within the first month. While she has not yet achieved complete abstinence, she has substantially decreased her drinking—typically limiting herself to 2–3 drinks on the weekends—and reports feeling “more in control” and less preoccupied with alcohol. Her mood, energy, and confidence have also improved, and she has expressed gratitude for having a care team that treats her with respect rather than judgment.
Her husband, initially resistant to the idea of therapy, agreed to participate in marital counseling and has scheduled his own intake appointment at the clinic. The couple now views recovery as a shared process, one that strengthens their partnership and family. They have begun spending more time together with their daughter in leisure activities outside the home and with her neighborhood playmates, noting the positive ripple effects of the treatment on their family life.
CONCLUSION
AUD (characterized by a pattern of problematic alcohol use that leads to significant distress or impairment in functioning, loss of control over consumption, involvement in risky behaviors, and with continued use despite its negative consequences) is a term that reflects a spectrum of severity (from mild to severe) and embraces more person-centered, nonstigmatizing language. AUD is diagnosed when individuals meet at least 2 of 11 criteria within a 12-month period, with the number of criteria present determining the severity of the disorder. The risk of developing an AUD is cumulative and multifactorial, involving an interplay of genetic, environmental, and psychological factors. Social determinants of health play a major role in the morbidity and mortality associated with alcohol use, with lower socioeconomic groups bearing the greatest burden. These risks are primarily driven by higher levels of chronic stress, including a greater prevalence of childhood trauma. Early recognition and treatment can mitigate or prevent the myriad medical and neurological sequelae associated with AUDs.
Article Information
Published Online: May 21, 2026. https://doi.org/10.4088/PCC.25f04133
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 5, 2025; accepted January 30, 2026.
To Cite: Matta SE, Terechin O, Braford MB, et al. Alcohol use disorders in primary care: screening, risk factors, and clinical implications. Prim Care Companion CNS Disord. 2026;28(3):25f04133.
Author Affiliations: Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts (Matta, Stern); Department of Psychiatry, Harvard Medical School, Boston, Massachusetts (Matta, Terechin, Stern); Home Base, Massachusetts General Hospital, Boston, Massachusetts; Department of Psychiatry, Brigham and Women’s Hospital, Boston, Massachusetts (Terechin); Lewis Gale Medical Center, Salem, Virginia (Braford); Bayhealth Medical Center, Dover, Delaware (DeSimone); Philadelphia College of Osteopathic Medicine, Philadelphia, Pennsylvania (DeSimone); Department of Psychiatry, Drexel University College of Medicine, Philadelphia, Pennsylvania (DeSimone).
Matta, Terechin, Braford, and DeSimone are co-first authors; Stern is the senior author.
Corresponding Author: Sofia Matta, MD, Department of Psychiatry, Massachusetts General Hospital, Harvard Medical School, 55 Fruit St, Boston, MA 02114 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Clinical Points
- Screening tools for the detection of alcohol use disorders (AUDs) include the Alcohol Use Disorders Identification Test-Concise; the CAGE Questionnaire (where even a single positive response is considered a positive screen); the Michigan Alcoholism Screening Test; the Tolerance, Annoyed, Cut down, Eye-opener (which adds an assessment of tolerance); the Screening, Brief Intervention and Referral to Treatment; the Parents, Peers, Partner, Past, Pregnancy (5-Ps); and the NIAAA Single-Item Alcohol Screening Questionnaire.
- A family history of AUD is one of the strongest predictors for the development of the disorder, with heritability estimates suggesting that approximately half of the risk for developing an AUD is genetic. Many psychiatric conditions co-occur with AUD, especially those that involve dysregulation of stress- and fear-related neural circuits, reward system pathways, and impulse control circuitry.
- Patients with major depressive disorder and a comorbid AUD often present with more severe manifestations, including thoughts of suicide, co-occurring personality disorders, and higher rates of smoking.
- Early recognition, through screening, and then referral for treatment, can reduce the adverse consequences of AUDs on biological (eg, multiple organ systems), psychological, and social domains.
References (56)

- Diagnostic and Statistical Manual of Mental Disorders, 4th edition. American Psychiatric Association; Washington, DC; 1994:194-204.
- Diagnostic and Statistical Manual of Mental Disorders, 5th edition, (DSM-5). American Psychiatric Association; Washington, DC; 2013:490-497.
- National Institute on Alcohol Abuse and Alcoholism. Alcohol use disorder: from risk to diagnosis to recovery. The Healthcare Professional’s Core Resource on Alcohol. 2025. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/alcohol-use-disorder-risk-diagnosis-recovery
- National Institute on Alcohol Abuse and Alcoholism. Screen and assess: use quick, effective methods. May 8, 2025. https://www.niaaa.nih.gov/health-professionals-communities/core-resource-on-alcohol/screen-and-assess-use-quick-effective-methods
- National Library of Medicine. AUDIT-C questionnaire. NIH Common Data Elements Repository. https://cde.nlm.nih.gov/formView?tinyId=myWNfJaZwe
- Nisavic M, Bains A. Substance use disorders. In: Stern TA, Beach SR, Smith FA, et al, eds. Massachusetts General Hospital Handbook of General Hospital Psychiatry. Eighth Edition. Philadelphia, PA: Elsevier;2025:682–686.
- Chang G, Fisher ND, Hornstein MD, et al. Identification of risk drinking women: T-ACE screening tool or the medical record. J Womens Health (Larchmt). 2010;19(10):1933–1939. PubMed CrossRef
- Ondersma SJ, Chang G, Blake-Lamb T, et al. Accuracy of five self-report screening instruments for substance use in pregnancy. Addiction. 2019;114(9):1683–1693. PubMed CrossRef
- Gordan AJ, Conigliaro J. Selective methods used in alcohol research: screening in primary care - methods and approaches. In: Preedy VR, Watson RR, eds. Comprehensive Handbook of Alcohol Related Pathology. Academic Press;2004:1327–1345.
- Babor TF, McRee BG, Kassebaum PA, et al. Screening, brief intervention, and referral to treatment (SBIRT): toward a public health approach to the management of substance abuse. Focus. 2011;9(1):130–148. CrossRef
- Hammock K, Velasquez MM, Alwan H, et al. Alcohol screening, brief intervention, and referral to treatment (SBIRT) for girls and women. Alcohol Res. 2020;40(2):07. PubMed CrossRef
- Bradley KA, DeBenedetti AF, Volk RJ, et al. AUDIT-C as a brief screen for alcohol misuse in primary care. Alcohol Clin Exp Res. 2007;31(7):1208–1217. PubMed CrossRef
- Selzer ML. The Michigan alcoholism screening test: the quest for a new diagnostic instrument. Am J Psychiatry. 1971;127(12):1653–1658. PubMed CrossRef
- National Institute on Drug Abuse. Screening and Assessment Tools Chart. NIDAMED: Clinical Resources. National Institutes of Health; 2025. https://nida.nih.gov/nidamed-medical-health-professionals/screening-tools-resources/chart-screening-tools
- Agabio R, Pisanu C, Gessa GL, et al. Sex differences in alcohol use disorder. Curr Med Chem. 2017;24(24):2661–2670. PubMed CrossRef
- Verhulst B, Neale MC, Kendler KS. The heritability of alcohol use disorders: a meta-analysis of twin and adoption studies. Psychol Med. 2015;45(5):1061–1072. PubMed CrossRef
- Edenberg HJ, McClintick JN. Alcohol dehydrogenases, aldehyde dehydrogenases, and alcohol use disorders: a critical review. Alcohol Clin Exp Res. 2018;42(12):2281–2297. doi:10.1111/acer.13904. PubMed CrossRef
- Li D, Sulovari A, Cheng C, et al. Association of gamma-aminobutyric acid A receptor α2 gene (GABRA2) with alcohol use disorder. Neuropsychopharmacology. 2014;39(4):907–918. PubMed CrossRef
- Ray LA, Bujarski S, MacKillop J, et al. Subjective response to alcohol among alcohol-dependent individuals: effects of the μ-opioid receptor (OPRM1) gene and alcoholism severity. Alcohol Clin Exp Res. 2013;37(Suppl 1):E116–E124. PubMed CrossRef
- Glaser YG, Zubieta JK, Hsu DT, et al. Indirect effect of corticotropin-releasing hormone receptor 1 gene variation on negative emotionality and alcohol use via right ventrolateral prefrontal cortex. J Neurosci. 2014;34(11):4099–4107. PubMed CrossRef
- Gowin JL, Sloan ME, Stangl BL, et al. Vulnerability for alcohol use disorder and rate of alcohol consumption. Am J Psychiatry. 2017;174(11):1094–1101. PubMed CrossRef
- World Health Organization. Addressing alcohol consumption and socioeconomic inequalities: How a health promotion approach can help (Snapshot series on alcohol control policies and practice; brief, 1). World Health Organization. Published June 4, 2021. https://www.who.int/publications/i/item/9789240043312
- Levis SC, Baram TZ, Mahler SV. Neurodevelopmental origins of substance use disorders: evidence from animal models of early-life adversity and addiction. Eur J Neurosci. 2022;55(9-10):2170–2195. PubMed CrossRef
- DeWit DJ, Adlaf EM, Offord DR, et al. Age at first alcohol use: a risk factor for the development of alcohol disorders. Am J Psychiatry. 2000;157(5):745–750. PubMed CrossRef
- Creswell KG. Drinking together and drinking alone: a social-contextual framework for examining risk for alcohol use disorder. Curr Dir Psychol Sci. 2021;30(1):19–25. CrossRef
- Mojica-Perez Y, Willoughby B, Anderson-Luxford D, et al. Exploring the relationship between solitary drinking and living without other adults on alcohol consumption during the COVID-19 pandemic. Alcohol Alcohol. 2024;59(3):age013. CrossRef
- Puddephatt JA, Irizar P, Jones A, et al. Associations of common mental disorder with alcohol use in the adult general population: a systematic review and meta-analysis. Addiction. 2022;117(6):1543–1572. PubMed CrossRef
- Anker JJ, Kushner MG. Co-occurring alcohol use disorder and anxiety: bridging psychiatric, psychological, and neurobiological perspectives. Alcohol Res Curr Rev. 2019;40(1):arcr.v40.1.03.
- Mason BJ. Looking Back, Looking Forward: current medications and innovative potential medications to treat alcohol use disorder. Alcohol Res. 2022;42(1):11. PubMed CrossRef
- Holma KM, Holma I, Isometsä E. Comorbid alcohol use disorder in psychiatric MDD patients: a five-year prospective study. J Affect Disord. 2020;267:283–288. PubMed CrossRef
- Yang P, Tao R, He C, et al. The risk factors of the alcohol use disorders-thorough review of its comorbidities. Front Neurosci. 2018;12:303. PubMed CrossRef
- Luderer M, Quiroga JAR, Faaone SV, et al. Alcohol use disorders and ADHD. Neurosci Biobehav Rev. 2021;128:648–660.
- Healy M, Richard A, Kidia K. How to reduce stigma and bias in clinical communication: a narrative review. J Gen Intern Med. 2022;37(10):2533–2540. PubMed CrossRef
- ASAM guideline on engagement and retention of nonabstinent patients in substance use treatment. https://www.asam.org/quality-care/clinical-recommendations/asam-clinical-considerations-for-engagement-and-retention-of-non-abstinent-patients-in-treatment
- Haber PS. Identification and treatment of alcohol use disorder. N Engl J Med. 2025;392(3):258–266. PubMed CrossRef
- Schwenker R, Dietrich CE, Hirpa S, et al. Motivational interviewing for substance use reduction. Cochrane Database Syst Rev. 2023;12(12):CD008063. PubMed CrossRef
- Matta SE, Terechin O, Podesta A, et al. Strategies for cutting down and stopping alcohol use. Prim Care Companion CNS Disord. 2024;26(3):23f03644. PubMed CrossRef
- Krebs P, Norcross JC, Nicholson JM, et al. Stages of change and psychotherapy outcomes: a review and meta-analysis. J Clin Psychol. 2018;74(11):1964–1979. PubMed CrossRef
- Krist AH, Bradley KA. Addressing alcohol use. N Engl J Med. 2025;392(17):1721–1731. PubMed CrossRef
- Andresen-Streichert H, Müller A, Glahn A, et al. Alcohol biomarkers in clinical and forensic contexts. Dtsch Arztebl Int. 2018;115(18):309–315. PubMed CrossRef
- Substance Abuse and Mental Health Services Administration. Drug Abuse Warning Network: National Estimates From Drug-Related Emergency Department Visits; 2024. Publication No. PEP25-07-005, Substance Abuse and Mental Health Services Administration, 2025. https://www.samhsa.gov/data/sites/default/files/reports/rpt56252/dawn-national-estimates-2024.pdf
- Mirijello A, Sestito L, Antonelli M, et al. Identification and management of acute alcohol intoxication. Eur J Intern Med. 2023;108:1–8. PubMed CrossRef
- Caputo F, Agabio R, Vignoli T, et al. Diagnosis and treatment of acute alcohol intoxication and alcohol withdrawal syndrome: position paper of the Italian Society on Alcohol. Intern Emerg Med. 2019 Jan;14(1):143–160. PubMed CrossRef
- Vonghia L, Leggio L, Ferrulli A, et al. Acute alcohol intoxication. Eur J Intern Med. 2008;19(8):561–567. PubMed CrossRef
- Strayer RJ, Friedman BW, Haroz R, et al. Emergency department management of patients with alcohol intoxication, alcohol withdrawal, and alcohol use disorder: a white paper prepared for the American Academy of Emergency Medicine. J Emerg Med. 2023;64(4):517–540. CrossRef
- Ashurst JV, Schaffer DH, Nappe TM. Methanol toxicity. [Updated 2025 Feb 6]. In: StatPearls [Internet]. StatPearls Publishing; 2025. https://www.ncbi.nlm.nih.gov/books/NBK482121
- Iqbal A, Glagola JJ, Nappe TM. Ethylene glycol toxicity. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025 Jan. https://www.ncbi.nlm.nih.gov/books/NBK537009/
- Ashurst JV, Nappe TM. Isopropanol toxicity. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan. https://www.ncbi.nlm.nih.gov/books/NBK493181
- Pergolizzi J, Breve F, Magnusson P, et al. Cocaethylene: when cocaine and alcohol are taken together. Cureus. 2022;14(2):e22498. PubMed CrossRef
- Shastry S, Manoochehri O, Richardson LD, et al. Cocaethylene cardiotoxicity in emergency department patients with acute drug overdose. Acad Emerg Med. 2023;30(2):82–88. PubMed CrossRef
- Bramming M, Becker U, Jørgensen MB, et al. Bariatric surgery and risk of alcohol use disorder: a register-based cohort study. Int J Epidemiol. 2021;49(6):1826–1835. doi:10.1093/ije/dyaa147. PubMed CrossRef
- Patel A. Alcohol use disorder and critical illness. In: Karamchandani K, Grant JE, et al, eds. Substance Use Disorders in Adult Critically Ill Patients. Nature Switzerland: Springer;2024:27–37.
- Wu X, Fan X, Miyata T, et al. Recent advances in understanding of pathogenesis of alcohol-associated liver disease. Annu Rev Pathol. 2023;18:411–438. PubMed CrossRef
- Noble JM, Weimer LH. Neurologic complications of alcoholism. Contin (Minneap Minn). 2014;20(3 Neurology of Systemic Disease):624–641. PubMed CrossRef
- Colrain IM, Nicholas CL, Baker FC. Alcohol and the sleeping brain. Handb Clin Neurol. 2014;125:415–431. PubMed CrossRef
- Lin JY, Zhang HB, Luo L, et al. Glymphatic system dysfunction in alcohol use disorder: current understanding and future directions. World J Psychiatry. 2025;15(10):107936. PubMed CrossRef
Please sign in or purchase this PDF for $40.




