Abstract
Objective: Collaborative care models (CoCMs) are modalities for treating mental health conditions in primary care. One such iteration of CoCM, antidepressant monitoring (ADM), is a pharmacologic treatment modality for the management of depression and anxiety. ADM programs have established efficacy, yet little is known about ideal patient selection or approaches related to program retention. The objective of this study was to address this need by examining predictors of referral from a CoCM ADM program to higher levels of psychiatric services.
Methods: A retrospective cohort analysis was conducted on individuals enrolled in the Tampa Veterans’ Affairs ADM program over 18 months (from June 4, 2018, through December 4, 2019). Data collected included information related to referral to a higher level of service, as well as baseline information and covariates of interest. Primary analysis was conducted utilizing a multivariable logistic regression model to evaluate whether baseline characteristics were associated with differences in referral rates to higher-level services.
Results: A total of 757 veterans were included in the analyses, with 131 (17.31%) referred on to a higher level of service for specialty psychiatric care. Multivariable modeling showed the following covariates to be associated with higher rates of referral to specialty psychiatric services: baseline 9-item Patient Health Questionnaire scores, sleep issues at the time of enrollment, alcohol use disorder, and cannabis use disorder.
Conclusions: Results show low rates of referral overall but identify a number of baseline characteristics associated with higher referral rates to specialty psychiatric services. Further research is needed, including prospective work and studies examining proactive interventions to limit required referrals to specialty mental health services.
Prim Care Companion CNS Disord 2026;28(2):25m04149
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Collaborative care models (CoCMs), sometimes referred to as collaborative care management or simply as collaborative care (CC), are treatment modalities for managing mental health conditions in primary care through a multidisciplinary approach of integrating care managers and psychiatric consultants along with primary care physicians (PCPs) and registered nurses (RNs). CoCM is a systems-level approach designed not only to improve individual patient outcomes but also to provide system-wide benefits in line with population-based care approaches such as optimization of the allocation of resources and treating individuals at the appropriate level on the mental health treatment continuum.1,2 There is a growing body of evidence supporting CoCM including randomized controlled trials that have demonstrated improvements in access to mental health care,3,4 improved treatment cost efficiency,5 and improvements in patient symptomatic outcomes for common mental illnesses.6
There are numerous models of collaborative mental health treatment that rely on 5 key components to achieve individual and system-wide benefits: population-based care, measurement-based care (MBC), care management, psychiatric consultation, and brief evidence-based psychotherapy.1 One such iteration of CoCM is antidepressant monitoring (ADM), which consists of collaboration between PCPs, consulting psychiatrists, and collaborative care managers (typically RNs). ADM is a protocol-driven treatment model consisting of frequent, regularly scheduled, telephonic follow-up contacts to monitor medication efficacy, tolerability, and adherence and to reinforce patient symptom self-management skills. These CoCM programs have been shown to be more effective at reducing symptoms of depression and anxiety, as well as leading to improvements in patient functioning, engagement, adherence, and all-cause mortality when compared to treatment as usual.3,7,8
Although this treatment model has established benefits, CoCM remains an emerging area with current unknowns related to treatment optimization, patient selection, and approaches related to enrollment and retention in CoCM programs. Efforts are underway to address these limitations in the literature, including previous work from our group examining predictors of adherence to completing the CoCM ADM treatment course.9 Although predicting adherence to the treatment model is an important patient-level factor as programmatic adherence and completion have been shown to be associated with improved outcomes, identifying individuals who will ultimately be referred to a higher level of mental health services may be more impactful from a system-wide, population-based care standpoint. That is, if pretreatment characteristics are found to be associated with lack of success in a CoCM program and predictive of referral to a higher level of service, algorithms could be developed to allow patient referral to the appropriate level of care more efficiently. This could represent early efforts toward developing an individualized, precision medicine approach within a population-based treatment model. However, presently, there is a paucity of information in this regard, and little has been reported on characteristics associated with referrals from CoCMs to required higher levels of specialty mental health services, an area in need of further research. This study aims to begin addressing this need by examining predictors of referral to higher-level mental health services in veterans treated for depression and anxiety in a primary case–based CoCM setting.
METHODS
A retrospective cohort analysis was conducted on all individuals who were referred for enrollment in the Tampa Veterans’ Affairs (VA) ADM CoCM program from June 4, 2018, through December 4, 2019. Data were obtained from the facility’s electronic health record (EHR) and from a preexisting clinical database. A secondary analysis was conducted for this study, and regulatory approval of the study was obtained from the local VA Research and Development Committee and the affiliated university institutional review board.
The ADM program is a clinical program for the management of veterans with depression and/or anxiety disorders receiving treatment exclusively in primary care clinics as opposed to specialty mental health clinics. The patient population studied is a pragmatic, clinical cohort, and as such, co-occurring mental health disorders were allowed for program enrollment. However, individuals with severe mental illness (SMI) such as bipolar affective disorder and psychotic disorders who would not be appropriate for management in primary care clinics were not included, as they require a higher level of service. As this was a clinical cohort, no additional predefined inclusionary or exclusionary criteria were utilized. There were no predetermined pharmacologic treatment algorithms, and medications were selected by consulting psychiatrist on an individual basis based on clinical patient-level factors. In the CoCM ADM program, veterans are contacted telephonically by RN collaborative care managers in every 3- to 4-week intervals, and information related to symptomatology (9-item Patient Health Questionnaire [PHQ-9]10 and 7-item Generalized Anxiety Disorder Scale [GAD-7]11), medication adherence, and tolerability is collected. This information is utilized by the consulting psychiatrist to inform ongoing treatment decisions in collaboration with the patient’s PCP. Patients are followed in the program for a goal minimum of 6 months, although follow-up for a period of greater than 6 months is possible if there are medication changes or other indications for additional monitoring arise.
The consulting psychiatrist, in addition to reviewing every new case enrolled in the program, also reviews every patient contact between the RN CoCMs and the veterans in the program, and medication changes are generally guided by the consulting psychiatrists in collaboration with the individual’s PCP. Consulting psychiatrists were either onsite or remotely located, most commonly remotely located, to allow implementation of this model across the broad catchment area of the facility. The CoCM utilized does not specifically limit the classes of medications that primary care providers can prescribe; however, generally early-line antidepressants and nonbenzodiazepine anxiolytics, such as selective serotonin reuptake inhibitors, serotonin-norepinephrine reuptake inhibitors, bupropion, buspirone, and mirtazapine, are the agents used in this treatment model. Although adjunct agents such as second-generation psychotics are not explicitly prohibited, individuals requiring such medications are typically more appropriate for management through a higher level of service with specialty mental health clinics, so their use in this model is rare. Behavioral therapy and evidence-based psychotherapies such as cognitive-behavioral therapy (CBT) were available and could be given concurrently with participation in the CoCM pharmacologic program. Further information on programmatic details can be found in the previous article.9
The current study examined predictors of referral to higher levels of service for veterans enrolled in the ADM program. Specifically, CoCM ADM is part of a stepped care model, and those who do not have a positive response to interventions in the ADM model may then be referred to a higher level of service, which is generally to establish with a general mental health clinic or a subspecialty mental health clinic to be followed directly with a psychiatrist in a typical outpatient treatment model. Data collected for this study included information related to referral including the clinic of referral and reason for referral. Other collected data included baseline information and covariates of interest that may have been associated with referral to higher levels of service (sociodemographic data, baseline depression and anxiety symptomatology as defined by scores on the PHQ-9 and the GAD-7, clinical contact with a psychologist within 4 weeks prior to ADM program enrollment, psychiatric polypharmacy, suicidal thoughts at the time of program enrollment, sleep impairments at the time of program enrollment, presence of co-occurring psychiatric disorders, and presence of co-occurring substance use disorders). Symptomatic outcomes were also recorded and can be found in the previous article.9 Referral to a higher level of service was defined as any consultation or referral made from the veteran’s PCP or the consulting CoCM psychiatrist for the veteran to be evaluated or to establish with a psychiatrist for direct psychiatric management in an outpatient mental health clinic (hereafter referred to as specialty mental health clinics, inclusive of both general psychiatric clinics and subspecialty psychiatry clinics such as posttraumatic stress disorder [PTSD] clinics or substance use disorders clinics). Referrals could be made at any time during the veteran’s participation in the CoCM ADM program at the discretion of the treating or consulting physicians, and reasons for referral were recorded.
Demographic and baseline characteristics were summarized as median and interquartile range for continuous variables and as frequencies and percentages for categorical variables. Characteristics were compared between participants who were referred to higher levels of service and those who were not using Mann-Whitney U tests for continuous variables and χ2 tests for categorical variables. Significance was set to .05.
Primary analysis was carried out using logistic regression models. For each baseline characteristic, a univariable logistic regression model was used to evaluate the association between that variable and referral to higher-level psychiatric services. Results were summarized as odds ratios (ORs) accompanied by 95% CIs. Variables that were significantly associated with referral to higher levels of service were then included in a multivariable logistic regression model to control for all baseline characteristics associated with referral to higher-level services. Results in this model were also summarized as OR with 95% CI. The multivariable logistic regression model was developed using a purposeful variable selection approach. Specifically, variables were selected through univariable logistic regression based on statistical significance and clinical relevance. This method was used rather than forward or backward stepwise methods to prioritize clinical relevance and integrate results of prior research. Additionally, interaction terms were not evaluated, as the primary goal of the study was to assess the main effects of the model. All analyses were performed using IBM SPSS Statistics.12
RESULTS
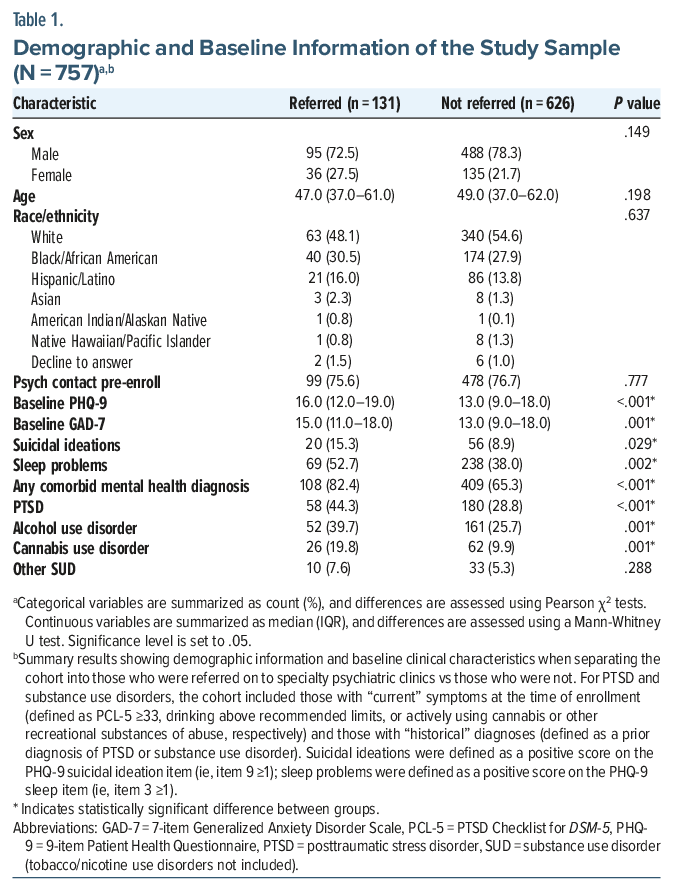
A total of 791 individuals were referred to the ADM program during the 18-month study period. Individuals who were referred but were never reached by the ADM treatment team were excluded, resulting in 757 veterans included in analyses. Demographic data were consistent with general VA population demographics, that is, most veterans included were male (77.01%) and white (53.24%). Veterans who were black/African American accounted for 28.27% of the cohort, and 14.3% were Hispanic/Latino. The mean age was 50.36 years (SD=15.34); the age range was 21–93 years. Baseline symptomatology reflected a cohort experiencing a mean moderate degree of depression and anxiety symptoms at the time of CoCM program enrollment (PHQ-9=13.57 [SD=5.65]; GAD-7=12.85 [SD=5.38]). Co-occurring psychiatric and substance use disorders were common, particularly PTSD (31.44% either meeting active PTSD symptomatic criteria [PTSD Checklist for DSM-513 ≥33] or having a prior diagnosis of PTSD) and alcohol use disorder (27.74% having current or past diagnoses of alcohol use disorder, with 19.42% drinking alcohol above recommended limits at the time of ADM program enrollment). Sleep disorders were prominent at the time of ADM program enrollment (87.22% as defined by the sleep item on the PHQ-9, item 3), and suicidal ideations were not uncommon (15.97% as defined by the suicidal ideations item on the PHQ-9, item 9).
Of the 757 veterans in the ADM program, 131 (17.31%) were ultimately referred on to a higher level of service for specialty psychiatric care. Of these 131, 64 (48.85%) were referred to the general outpatient mental health clinic; 27 (20.61%) to the women’s center psychiatry clinic; 17 (12.98%) to the PTSD clinic; 14 (10.69%) to the geriatric psychiatry clinic; 5 (3.82%) to the SUDS clinic; and 5 (3.82%) to other specialty psychiatrist run clinics (traumatic brain injury clinic, polytrauma, etc). Reasons for referral to a higher level of service were nearly exclusively due to lack of symptomatic improvements in ADM, with 121 (92.37%) of the patients referred continuing to have at least moderate range symptoms of depression and/or anxiety at the time of referral. Other reasons for referral include 3 veterans who had symptomatic improvements but requested to establish with a psychiatrist in a traditional, face-to-face treatment model; 3 who had improvements in depression and anxiety but residual PTSD symptoms requiring additional treatment; 2 who had symptomatic improvements per MBC but a worsening objective presentation (including 1 who had a psychiatric hospitalization and 1 who developed bupropion-emergent suicidal ideations); 1 who had persistent sleep issues not responsive to numerous early-line sleep aids; and 1 who had improvements in depression and anxiety but continued substance abuse issues and accepted a referral to the SUDS clinic.
Demographic information and baseline clinical characteristics were then analyzed, separating the cohort into those who were referred on to higher levels of psychiatric services and those who were not. Categorical variables were assessed using Pearson χ2 tests; continuous variables were assessed using Mann-Whitney U tests. A number of baseline covariates of interest were found to differ between those who were referred to higher levels of service compared to those who were not, including baseline PHQ-9 scores (P<.001), baseline GAD-7 scores (P =.001), suicidal ideations (P=.029), sleep issues (P =.002), concurrence of any comorbid mental health diagnoses (P<.001), comorbid PTSD (P <.001), current or past diagnosis of alcohol use disorder (P=.001), and current or past diagnosis of cannabis use disorder (P =.001). Results are summarized in Table 1.
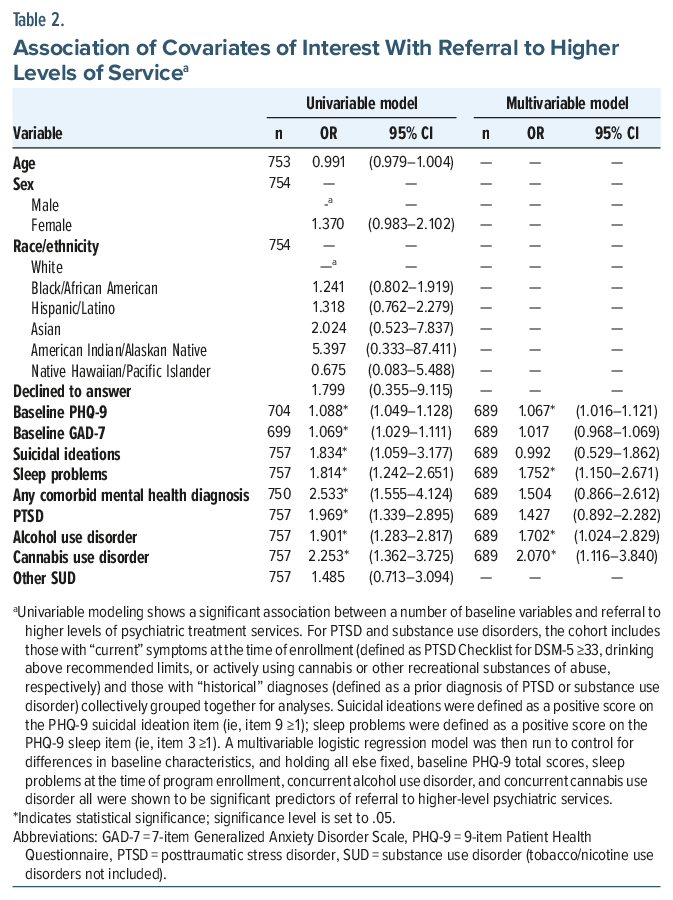
Next, regression models were used to analyze covariates as potential predictors of referral to higher-level services, first utilizing univariable regression models to assess baseline covariates associated with differences in completion rates, followed by a multivariable logistic regression model utilized to identify if associations with program completion remained after controlling for variables with significant baseline differences identified in the univariable model. Although the univariable model showed a number of statistically significant differences, after controlling for baseline differences the multivariable model showed the following to be associated with higher rates of referral to specialty psychiatric services: baseline PHQ-9 scores (OR=1.067, 95% CI, 1.016–1.121); sleep issues at the time of program enrollment (OR=1.752, 95% CI, 1.150–2.671); current or past history of alcohol use disorder (OR =1.702, 95% CI, 1.024–2.829); and current or past history of cannabis use disorder (OR=2.070, 95% CI, 1.116–3.840). Results of univariable and multivariable regression analyses are summarized in Table 2.
DISCUSSION
Results reveal several findings applicable to clinical and future research endeavors. First, greater than 82% of veterans in the CoCM ADM program did not require referral to higher levels of service. This is important for entities that focus on population-based treatment services. Specialty mental health care with outpatient psychiatrists remains a limited resource,14 and keeping mental health care in the appropriate setting is one of the primary systematic benefits of CoCM programs. Our results showing low referral rates strongly support the effectiveness of this intervention in keeping patients at the appropriate level of mental health treatment services. This has immediate and long-term impacts on systems including decreasing wait times to specialty MHCs and allowing MHCs to focus on individuals with higher degrees of symptomatic burdens and individuals with SMI. Further, limiting referrals to higher levels of service is financially important for entities that provide population-based care services, such as the VA, as CoCM services have been shown to provide economic benefits including reducing costs compared to treatment as usual in various populations and clinical settings.5,15,16
Regarding predictors of referral from a CoCM ADM program to higher levels of mental health services, there is a paucity of research in this area. Although there are studies examining referrals to psychiatry services in the context of traditional treatment models17 and one study looking at referrals in clinics that have embedded collaborative care providers,18 to the authors’ knowledge, there are no reported studies examining referrals from individuals established in CoCM programs such as ADM to higher levels of psychiatric service. Identifying predictors of referrals has important implications. If specific baseline factors are associated with need for referral to higher levels of service, clinical treatment flow algorithms could be established to guide patient placement in CoCM vs. specialty psychiatric care. Alternatively, if baseline factors are known to increase referral rates, studies could be designed to examine if proactive interventions targeted toward these factors could improve outcomes in the CoCM program and decrease the requirement for referrals to higher levels of service. Our results show that several baseline characteristics were associated with referral to higher-level services including baseline depression symptoms, sleep issues, and substance abuse issues (both alcohol and cannabis). Although baseline depressive symptoms would likely be a nonmodifiable characteristic, as it is the reason for seeking treatment, targeted interventions for improving sleep or addressing substance abuse issues could be implemented. For example, pre-CoCM CBT for insomnia or earlier/more aggressive pharmacologic management of insomnia could be considered. Similarly, psychotherapy services directed toward abstinence from substances could be implemented prior to or during the early phases of the CoCM program. Medication-assisted treatment for alcohol use could also be considered either prior to or concurrently with the CoCM pharmacologic antidepressant intervention. Future research including prospective clinical trials should be conducted.
Notably, nonalcohol/noncannabis substance abuse issues were not found to be associated with referral to higher levels of service. This may be explained by the low number of veterans with use disorders of other substances included in our cohort. A selection bias may also have been observed, as treatment-seeking individuals with other substance use disorders such as stimulants or opioids are more appropriately treated with higher levels of services than are offered in primary care. Lastly, as this was a retrospective review that relies on the accuracy of EHRs, it is possible that substance use that did not accurately meet diagnostic criteria for a use disorder was inappropriately diagnosed as such (eg, uncommon historical use may have been misdiagnosed as a use disorder, which could be more likely to occur with opioids or stimulants as opposed to more commonly used substances such as alcohol or cannabis).
Lastly, it is of note that referral to a higher level of service should not be considered a failure in this treatment model. Stepped care as a component of population-based services involves starting treatments at lower levels of service and escalating treatment modalities to higher levels if/as needed. This should be considered when interpreting the results of this study.
Limitations
Limitations of the study include the retrospective nature of the work, which include relying on the accuracy of the written record and difficulty in controlling bias/confounders.19,20 Another limitation in retrospective research is the potential for missing data. However, in our study, data that are missing are missing at random and not due to study design or implementation, thus reducing potential bias that could be introduced due to missing data. Another common limitation of retrospective studies is lack of longitudinal follow-up. However, our study had a longitudinal tracking component, which could be viewed as a strength of this retrospective work. Additional limitations specific to this study include that this was a secondary analysis and included a wholly veteran cohort, which may make the findings less generalizable. Specific strengths of the study include the large sample size, longitudinal patient monitoring, and pragmatic design utilizing a clinical population and clinical interventions, which make the findings directly relevant to clinical practice.
CONCLUSIONS
CoCMs have proven efficacy in the treatment of mental health disorders in primary care settings, yet there is a need to examine these models further including patient selection and factors related to retention and referral to optimize these approaches. The presented study examined baseline characteristics associated with the need for referral from a CoCM program to higher levels of services and, to the authors’ knowledge, is the first study reporting on predictors of referral from a CoCM pharmacologic treatment program to higher levels of psychiatric services. Results revealed baseline characteristics associated with referral to higher levels of psychiatric services including severity of baseline depressive symptoms, sleep issues, alcohol use disorder, and cannabis use disorder. Future studies, including prospective work, should be conducted to further examine associations and predictors of referrals. Additionally, studies examining interventions targeted toward known predictors of referral should be conducted to analyze whether proactive interventions can decrease requirements for referrals to specialty mental health services.
Article Information
Published Online: April 23, 2026. https://doi.org/10.4088/PCC.25m04149
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 25, 2025; accepted January 19, 2026.
To Cite: Zuschlag ZD, Lord B, Smith T, et al. Baseline characteristics associated with referrals from a primary care mental health collaborative care model to specialty mental health services. Prim Care Companion CNS Disord. 2026;28(2):25m04149.
Author Affiliations: Mental Health and Behavioral Sciences Service, James A. Haley Veterans’ Hospital, Tampa, Florida (Zuschlag, Lord, Norred, Leventhal, Milsom); Department of Psychiatry and Behavioral Neurosciences, University of South Florida, Tampa, Florida (Zuschlag, Norred); Research Methodology and Biostatistics Core, University of South Florida, Tampa, Florida (Smith); Internal Medicine and Special Care Service, James A. Haley Veterans’ Hospital, Tampa, Florida (Nedervelt).
Corresponding Author: Zachary D. Zuschlag, DO, 13000 Bruce B. Downs Blvd, Tampa, FL 33612 ([email protected]).
Financial Disclosure: None.
Funding/Support: Grant support for this work was provided by the Tampa VA Research and Education Foundation (Tampa, Florida). Material support, resources, and the use of facilities were provided by the James A. Haley Veterans’ Hospital.
Disclaimer: This material is the result of work supported with resources and the use of facilities at the James A. Haley Veterans’ Hospital. The contents of this publication do not represent the views of the Department of Veterans Affairs or the United States Government.
ORCID: Zachary D. Zuschlag: https://orcid.org/0000-0001-8556-7767; Teagan Smith: https://orcid.org/0000-0002-5573-3178; Michael A. Norred: https://orcid.org/0000-0002-5879-7994
Clinical Points
- Pharmacologic collaborative care models can be effective treatments for the management of depression and anxiety in primary care settings.
- Certain baseline characteristics are associated with higher rates of referral from a CoCM to specialty psychiatric services including higher severity of baseline depression symptoms, sleep issues, alcohol use disorder, and cannabis use disorder.
- Individuals with these characteristics may be more appropriate for specialty mental health clinics as their initial level of care; proactive targeted interventions may also be considered to mitigate concerns related to these characteristics.
References (20)

- Reist C, Petiwala I, Latimer J, et al. Collaborative mental health care: a narrative review. Med Baltim. 2022;101(52):e32554. PubMed CrossRef
- Goodrich DE, Kilbourne AM, Nord KM, et al. Mental health collaborative care and its role in primary care settings. Curr Psychiatry Rep. 2013;15(8):383. PubMed CrossRef
- Coventry PA, Hudson JL, Kontopantelis E, et al. Characteristics of effective collaborative care for treatment of depression: a systematic review and Meta-regression of 74 Randomised controlled trials. In: Hay PJ, ed.. 9;2014.PLoS ONE9e108114 PubMed CrossRef
- Guo T, Xiang YT, Xiao L, et al. Measurement-based care versus standard care for major depression: a randomized controlled trial with blind raters. Am J Psychiatry. 2015;172(10):1004–1013. PubMed CrossRef
- Miller CJ, Griffith KN, Stolzmann K, et al. An economic analysis of the implementation of team-based collaborative care in outpatient general mental health clinics. Med Care. 2020;58(10):874–880. PubMed CrossRef
- Huffman JC, Niazi SK, Rundell JR, et al. Essential articles on collaborative care models for the treatment of psychiatric disorders in medical settings: a publication by the academy of psychosomatic medicine research and evidence-based practice committee. Psychosomatics. 2014;55(2):109–122. PubMed CrossRef
- Gilbody S., Bower P, Fletcher J, et al. Collaborative care for depression: a cumulative meta-analysis and review of longer-term outcomes. Arch Intern Med. 2006;166(21):2314–2321. PubMed CrossRef
- Unützer J, Katon W, Callahan CM, et al. Collaborative care management of late-life depression in the primary care setting: a randomized controlled trial. JAMA. 2002;288(22):2836–2845. PubMed CrossRef
- Zuschlag ZD, Lord B, Smith T, et al. The management of depression and anxiety in primary care: examining predictors of adherence to a psychopharmacological collaborative care management program for veterans. J Behav Health Serv Res. 2025;52(1):19–31. PubMed CrossRef
- Kroenke K, Spitzer RL, Williams JB. The PHQ-9: validity of a brief depression severity measure. J Gen Intern Med. 2001;16(9):606–613. PubMed CrossRef
- Spitzer RL, Kroenke K, Williams JBW, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. PubMed CrossRef
- IBM SPSS Statistics for Windows. Published online 2020.
- Weathers FW, Litz BT, Keane TM, et al. The PTSD Checklist for DSM-5 (PCL-5). 2013. https://www.ptsd.va.gov/professional/assessment/adult-sr/ptsd-checklist.asp
- Aggarwal R, Balon R, Beresin EV, et al. Addressing psychiatry workforce needs: where are we now?. Acad Psychiatry. 2022;46(4):407–409. PubMed CrossRef
- Wright DR, Haaland WL, Ludman E, et al. The costs and cost-effectiveness of collaborative care for adolescents with depression in primary care settings: a randomized clinical trial. JAMA Pediatr. 2016;170(11):1048–1054. PubMed CrossRef
- HR Policy Association. Collaborative Care Model Reduces Total Health Care Costs. American Health Policy Institute; 2024. https://www.hrpolicy.org/insight-and-research/resources/2024/hr_workforce/public/05/collaborative-care-model-reduces-total-health-care/. Accessed October 10, 2025
- Kravitz RL, Franks P, Feldman M, et al. What drives referral from primary care physicians to mental health specialists? A randomized trial using actors portraying depressive symptoms. J Gen Intern Med. 2006;21(6):584–589. PubMed CrossRef
- Auxier A, Runyan C, Mullin D, et al. Behavioral health referrals and treatment initiation rates in integrated primary care: a Collaborative Care Research Network study. Transl Behav Med. 2012;2(3):337–344. PubMed CrossRef
- Hess DR. Retrospective studies and chart reviews. Respir Care. 2004;49(10):1171–1174. PubMed CrossRef
- Sartwell PE. Retrospective studies: a review for the clinician. Ann Intern Med. 1974;81(3):381–386. PubMed CrossRef
Please sign in or purchase this PDF for $40.




