In patients with severe mental illness, including autism spectrum disorder (ASD) and intellectual disability, hyponatremia due to compulsive water drinking (polydipsia), as part of restricted and repetitive behavior (RRB), can be resistant to behavioral interventions. Selective serotonin reuptake inhibitors (SSRIs), although potentially useful for obsessive-compulsive symptoms, can be counterintuitive, as they are associated with syndrome of inappropriate antidiuretic hormone secretion (SIADH) and thus are relatively contraindicated. Low-dose mirtazapine might be an alternative worth trying as portrayed in this case report.
Case Report
One of our consultation-liaison team members (A.N.) was asked to check on a 10-year-old prepubertal Kuwaiti boy, a known case of low-functioning essential ASD, who had been following up in the private sector and was recently admitted to the general pediatrics ward. He presented with his mother to the emergency department with new-onset serial seizures.
He was enrolled in special schooling and was minimally verbal, at times with immediate echolalia, as well as morbidly obese, normokinetic, and nonepileptic. There was no history of behavioral dyscontrol or previous trials on psychotropic medications.
Workup for new-onset seizures was undertaken. Hyponatremia (serum sodium level of 121 mmol/L) was the main culprit—characterized as hypotonic and euvolemic, with diluted urine. This was promptly, but cautiously, corrected, and he was medically cleared. It was then noted during hospitalization that he was repetitively overdrinking throughout the day every few minutes, and this culminated in repeated bouts of hyponatremia. Whenever his mother attempted to prevent him from overdrinking, he would become severely agitated. As reported by his mother, this behavior started only a few days prior to the current admission immediately following a dental procedure. A dental consultation was requested, but no specific directions were provided. It was made clear to us that compulsive polydipsia was part of his RRB and that it needed to be addressed to curb the resultant repeated hyponatremia.
With involvement of his mother, occupational therapist input was enlisted for completion of a sensory profile and diet, a plan to enforce a daily routine and structure, a visual schedule with timed drinking, and diversion/distraction techniques to prevent polydipsia with the help of hospital-based social workers. Although this sounded like a well-rounded plan of action, unfortunately, it failed to bring about any tangible behavioral response, as the patient remained fixated on overdrinking and would become agitated when restricted.
A more behaviorally focused approach was then suggested, capitalizing on classical Pavlovian conditioning, by coupling an alarm ring with timed drinking. But again, due to nonengagement of the patient, the application was erratic, and the response was not sustained.
A trial of an SSRI was considered to tackle this compulsion, but this was counterintuitive since SSRIs are notorious for inducing SIADH. An off-label trial of mirtazapine, unlikely to induce SIADH and allegedly possessing antiobsessional actions, was started at 3.75 mg at bedtime and was soon increased to twice daily (informed consent was obtained from his mother beforehand). Over a week, there was a marked reduction in his polydipsia without oversedation. This was shown on a behavioral chart devised by the occupational therapist depicting the frequency of compulsive polydipsia per hour (which declined after introducing mirtazapine from a mean of 11.8/h/d to 2.6/h/d). The response was impressive, incremental, and well sustained thereafter at the same daily dose. Mirtazapine also seemed to help him more readily engage with occupational therapy, facilitating the application of diversion/distraction techniques. He was safely discharged on this treatment regimen and linked to the outpatient department. Six months later, this response was maintained, with no reported hyponatremia incidents, and the patient was doing well.
Discussion
RRBs are a core and defining symptom in up to 85% of individuals with ASD, but less so in girls, and are among the earliest signs of ASD. RRBs may be all-enthralling and time-consuming, adding to caregivers’ stress dealing with the often “catastrophic” reactions by children when these behaviors are interrupted. These behaviors can also be potentially life-threatening as described in this case.
There is mounting evidence implicating altered basal ganglia function in the mediation of RRBs. RRBs encompass stereotyped movements (eg, hand flapping), repetitive self-injurious behaviors (low-order sensorimotor), rituals and elaborate routines, insistence on sameness and resistance to change (high order), and idiosyncratic interests, preoccupations, and attachments (circumscribed). RRBs might serve stress reduction, sensory stimulation, and reward.
SSRIs were shown to be generally ineffective given the egosyntonic nature of RRBs, but in our case, SSRIs were even counterproductive for a theoretical risk of SSRI-related SIADH, which might have otherwise exacerbated hyponatremia. Some focused intervention practices (eg, behavioral teaching strategies) such as prompting, differential reinforcement, and interruption/redirection can effectively reduce the occurrence of some types of RRBs and associated problem behaviors such as aggression, noncompliance, and self-injury. When severe, medications can be trialed.1
When generating the differential diagnosis of hyponatremia in a psychiatric context, it is crucial to include water intoxication (psychogenic polydipsia) and SIADH at the top of the list (with diluted urine in the former and concentrated in the latter). SSRIs, oxycarbazepine, valproate, desmopressin, and antipsychotics have all been incriminated. Fluid restriction is generally recommended. While clozapine can help with the former, demeclocycline has some evidence to help with the latter. Vaptans remain a promising option for both conditions.2 In a minority of patients, this could be a core part of illness (eg, a schizophrenic patient with psychotic polydipsia) or, as in our report, part of autistic RRBs triggered by a dental procedure that could have instigated xerostomia or a sensory issue.
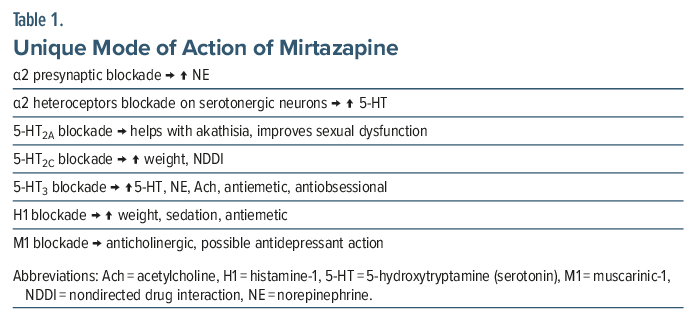
We elected to choose mirtazapine, an atypical antidepressant, classified as a noradrenergic and specific serotonergic antidepressant, as it is one of the few antidepressants that are unlikely to induce SIADH (the other ones being bupropion and minaserin). Moreover, mirtazapine has putative antiobsessional properties that might be ascribed to composite proserotonergic actions3 (Table 1) via α2 heteroceptor blockade on serotonergic neurons and 5-hydroxytryptamine type 3 antagonism. Mirtazapine has also been shown to confer additional relapse prevention in OCD and to hasten SSRI response as an adjunctive.4
Use of mirtazapine in the child and adolescent psychiatry population is off label. Two unpublished industry-sponsored RCTs with mirtazapine yielded negative results.
For ASD, in an open-label trial, 35% were considered responders as measured with the Clinical Global Impressions-Improvement scale, with reduced aggression, self-injury, irritability, hyperactivity, anxiety, insomnia, and depression. A retrospective study found mirtazapine helpful for inappropriate sexual behaviors.5 However, a double-blind randomized controlled trial for anxiety revealed a nonsignificant trend toward the superiority of mirtazapine compared to placebo.6 All studies indicated favorable tolerability.
This report illustrates how RRBs in autistic children could be potentially serious while being recalcitrant to behavioral interventions. Such cases might dictate atypical choices on clinical grounds, as shown here, that need to be carefully crafted given the intricacies inherent to each case. Mirtazapine remains a viable option to explore in children with ASD and obsessive-compulsive symptoms, with good tolerability and efficacy. Larger, rigorous, and well-conducted studies in this population are warranted before generalizing these findings.
Article Information
Published Online: April 30, 2026. https://doi.org/10.4088/PCC.25cr04099
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04099
Submitted: October 3, 2025; accepted December 16, 2025.
To Cite: Naguy A, Pridmore S, Abul HH, et al. Compulsive polydipsia-related symptomatic hyponatremia in a low-functioning autistic boy. Prim Care Companion CNS Disord 2026;28(2):25cr04099.
Author Affiliations: Al-Manara CAP Centre, Kuwait Centre for Mental Health, Shuwaikh, State of Kuwait (Naguy, Alamiri); Department of Psychiatry, University of Tasmania, Hobart, Tasmania, Australia (Pridmore); Sayed Abdulrazzag Clinic, Kuwait City, Kuwait (Abul).
Corresponding Author: Ahmed Naguy, MBBch, MSc, MRCPsych (UK), Al-Manara CAP Centre, Kuwait Centre for Mental Health (KCMH), Jamal Abdul-Nassir St, Shuwaikh, State of Kuwait ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient’s guardian to publish the case report, and information has been de-identified to protect patient anonymity.
References (6)

- Naguy A, Yahya B. Restricted and repetitive behaviours in autism spectrum disorder through a clinical lens. Asian J Psychiatr. 2018;31:79–80. PubMed CrossRef
- Pinkhasov A, Xiong G, Burgeois JA, et al. Management of SIADH-related hyponatremia due to psychotropic medications – an expert consensus from the Association of Medicine and Psychiatry. J Psychosom Res. 2021;151:110654. PubMed CrossRef
- Naguy A. Onco-psychopharmacology: is mirtazapine a catholicon?. Prim Care Companion CNS Disord. 2025;27(3):25lr03918. PubMed CrossRef
- Naguy A, Alamiri B. Treatment-resistant OCD - a psychopharmacological ’touche d’art. Asian J Psychiatr. 2018;34:98–99. PubMed CrossRef
- Posey DJ, Guenin KD, Kohn AE, et al. A naturalistic open-label study of mirtazapine in autistic and other pervasive developmental disorders. J Child Adolesc Psychopharmacol. 2001;11(3):267–277. PubMed CrossRef
- McDougle CJ, Thom RP, Ravichandran CT, et al. A randomized double-blind, placebo-controlled pilot trial of mirtazapine for anxiety in children and adolescents with autism spectrum disorder. Neuropsychopharmacology. 2022;47(6):1263–1270. PubMed CrossRef
Please sign in or purchase this PDF for $40.




