Abstract
Objective: To compare effects of adjunctive active versus sham vagus nerve stimulation (VNS) on suicidal ideation (SI) in markedly treatment-resistant depression (TRD).
Methods: RECOVER trial participants with nonpsychotic major depressive disorder and insufficient benefit from ≥4 adequate antidepressant trials in the current episode were randomized to adjunctive active or sham VNS plus treatment as usual over 12 months. SI was assessed at baseline and monthly (months 3–12) following VNS parameter titration/ pseudotitration. A composite suicidal ideation (CSI) score (range, 0–9) used SI items from 3 depressive symptom ratings to assess VNS effects on SI for those with (CSI ≥3) and without (CSI ≤2) significant baseline SI.
Results: This exploratory study involved a sample (N = 463) who averaged 13.3 failed lifetime antidepressant treatments, with 17.7 years in the current depressive episode; 40.4% had previously attempted suicide. Among individuals with baseline SI, the likelihood of meaningful improvement (CSI score change ≥3) was greater with active than sham VNS (odds ratio [OR] = 1.43; 95% CI, 1.004–2.021; P < .05) over 10 months of evaluation. Additionally, active VNS was superior to sham VNS for SI remission (CSI ≤2) in months 10–12 (OR = 1.67; 95% CI, 1.007–2.763; P < .05). VNS did not significantly worsen SI in participants.
Conclusions: This study suggests that, compared to sham VNS, active VNS reduces SI and potentially induces SI remission among participants with chronic TRD and baseline SI. Furthermore, VNS does not appear to worsen or induce SI in participants, regardless of their baseline SI status. Further research is warranted.
Trial Registration: ClinicalTrials.gov identifier: NCT03887715
J Clin Psychiatry 2026;87(3):25m16296
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
The growing rate of suicide is an urgent national priority for the United States.1 Most suicide attempts and deaths occur in the context of major depressive disorder (MDD).2–4 Treatment-resistant depression (TRD) carries a particularly high risk of suicide attempts and deaths.5–7 Few psychiatric treatments have demonstrated specific effectiveness in reducing suicidal ideation (SI) or behavior.8 Antisuicidal effects have been linked to treatment with clozapine,9 intravenous ketamine,10 lithium,11–13 and electroconvulsive therapy (ECT),14–16 while multiple psychotropic medications, including antidepressants, are labeled as having the potential to increase SI and attempts in children and young adults.17,18
Vagus nerve stimulation (VNS), a US Food and Drug Administration (FDA)–cleared treatment for TRD, is not an acute intervention for SI or behaviors. However, previous studies have suggested that long-term treatment with VNS is associated with reduced suicidal behaviors, though these reports were predominantly open-label, observational, and insufficiently powered to provide definitive conclusions.19,20
The recently completed randomized, controlled, unipolar TRD arm of the RECOVER trial21 enrolled 493 participants with markedly treatment-resistant MDD to compare the efficacy of adjunctive active and sham VNS over 12 months. Although the primary outcome—months in response based on the Montgomery-Asberg Depression Rating Scale (MADRS)—did not differentiate between treatment groups, active VNS demonstrated statistically significant and clinically meaningful benefits across selected measures of depressive symptoms, quality of life, and functional outcomes.22–24
The assessment of suicide, both ideation and behaviors, is challenging in clinical trials. Completed suicides and suicide attempts are uncommon and thus relatively insensitive metrics for detecting differential treatment effects. However, SI, which is more common than attempts or completions, has recently been recognized as a major modifiable risk factor for death by suicide.25 In a meta-analysis by McHugh et al,26 patients with SI were 3.41 times more likely to die by suicide than those without SI and disproportionately likely to attempt suicide over an average duration of 9.1 years of follow-up.27 Additionally, SI severity is positively associated with suicide risk,28 and SI is associated with death by suicide with fairly strong specificity.26 For these reasons, it has been proposed that precise measurement of pre- versus post-SI is a valid measure for assessing treatments directed at reducing suicide (eg, intravenous ketamine).29
Composite metrics have been utilized in psychiatric and other clinical research to provide more robust measures of complex constructs, such as SI, by integrating multiple data sources. Prior studies have incorporated the Hamilton Depression Rating Scale (HDRS) item 3, MADRS item 10, and Beck Depression Inventory item 9 into a composite metric.30,31 Ballard et al31 demonstrated strong correlations between the clinician-administered suicide items of the HDRS and MADRS and the first 5 items of the Scale for Suicidal Ideation, suggesting these measures are highly concordant when tracking rapid changes in SI. Further, integrating data sources in a composite measure enhances the reliability and validity of SI assessment.32
Given the high risk of suicide attempts and completions with markedly TRD, determining the effects of VNS33 on SI is consequential for patients with and without meaningful ideation at the initiation of treatment. This report examines the effects of active versus sham adjunctive VNS (each administered with treatment as usual [TAU]) on SI over a 10-month blinded observation period, which provides important information for managing patients receiving VNS.
METHODS
Study Design
The first phase of the RECOVER trial used a multicenter, randomized, triple-blind, sham-controlled, 12-month design that evaluated the safety and efficacy of adjunctive VNS in participants with markedly TRD.34 Participants received either adjunctive active or sham VNS therapy, with TAU continued throughout the study. All participants provided written informed consent (ClinicalTrials.gov identifier: NCT03887715).
RECOVER participants were ≥18 years of age; were experiencing a current major depressive episode (MDE) of nonpsychotic MDD based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition; had failed at least 4 adequate, medical record–verified antidepressant treatments in the current MDE35; and had at least moderately severe depression at baseline (MADRS score ≥22 on 2 separate occasions, 14–16 days apart).36 Baseline MADRS severity was the average of these 2 measures.
Baseline demographic and clinical features of RECOVER participants,33 findings regarding the efficacy in reducing depression severity and safety of adjunctive VNS,22 and effects on quality of life and psychosocial function23 have been published.
Measurement of SI
We developed a composite scale a priori, termed the composite suicidal ideation (CSI) score, to quantify SI by combining responses to the suicide items on the MADRS, Quick Inventory of Depressive Symptomatology–Clinician (QIDS-C), and Quick Inventory of Depressive Symptomatology–Self-Report (QIDS-SR). This composite scale reflected the assessments by off-site blinded raters (MADRS and QIDS-C) and participants (QIDS-SR) combined into a single score. The rationale for combining these 3 metrics was to consider the multiple perspectives on SI available in the study. The composite metric balances the considerations that some participants may readily disclose ideation in the presence of a rater, while others may more readily disclose on self-report.
On the MADRS, the SI item (item 10) is rated 0–6, while it is rated 0–3 on both the QIDS-C and the QIDS-SR (item 12). We rescaled the MADRS ratings to match the QIDS scales; the original MADRS ratings were rescaled where 0 = none (0), 1–2 = mild (1), 3–4 = moderate (2), and 5–6 = severe (3). Thus, the composite metric, termed the CSI score, ranged from 0 to 9, with higher numbers indicating greater SI. The CSI values were considered missing at a given assessment time point if at least 2 of the 3 scales were not completed. If 1 scale was not completed, the CSI score for that assessment was calculated by taking the mean of the 2 available scores and multiplying by 3. Baseline SI item scores for the QIDS-C and QIDS-SR used in the CSI were the second of the 2 measures taken at baseline (baseline 2: 14–16 days after baseline 1). For the MADRS, the baseline score used in analyses was an average of the SI item at baseline 1 and baseline 2.
We established clinically meaningful thresholds for CSI scores a priori. No or minimal ideation was defined as CSI scores of 0–2, while ≥3 denoted “meaningful” SI. Finally, also a priori, we declared a clinically meaningful change in the CSI total score (either up or down) as ≥3 points (approximating a movement of 1 point on each of the 3 scales). For those with SI at baseline (CSI ≥3), remission of SI was established a priori as a CSI score drop of ≥3 and total CSI score of ≤2.
Time Periods for Assessing Treatment Effects on SI
We chose 2 distinct time periods with which to compare the differential effects of active versus sham VNS. First, to capture the overall effect, we used all measurement occasions (baseline and months 3–12 following implantation). Second, since previous VNS clinical trials showed improved benefit after 6–12 months of stimulation and the RECOVER trial showed the efficacy of VNS relative to sham was greatest in months 10–12 of the randomized, blinded phase,37,38 we compared active and sham VNS during these last 3 months of the randomized phase.
Statistical Analyses
The analytic sample (N = 463) included all participants with a baseline CSI score and at least 1 postimplantation assessment. Participants who withdrew prior to the first postimplantation assessment (15 in active VNS, 15 in sham VNS) were excluded. The analyses were conducted separately on those with meaningful baseline SI (CSI score ≥3; N = 286) and those with minimal or no baseline SI (CSI score = 0–2; N = 177).
The active VNS (N = 234) and sham VNS (N = 229) groups and the subsamples defined by the presence/absence of meaningful SI at baseline were compared by demographic, treatment history, and clinical characteristics, using t tests and χ2 analyses on continuous and categorical variables, respectively. In each sample, the treatment groups were also compared in continuous score on the suicide item on each of the 3 scales, as well as total baseline CSI score and in the classification of CSI scores.
Analyses were conducted of those with meaningful SI (CSI ≥3) at baseline, testing whether the treatment groups differed in the proportion of participants who showed meaningful reduction in SI (reduction of ≥3 from baseline CSI score) over the 10 assessment occasions (months 3–12). For the repeated measures assessments, missing data were assumed to be missing at random using a generalized linear mixed model (GLMM) with a binomial distribution, random intercept, and a logit link function to test the treatment effect, adjusted for the covariates of treatment arm, visit, treatment-by-visit interaction, age group (<65, ≥65), MADRS baseline score group (<34, ≥34), and baseline continuous value of the outcome variable. Treatment effects were estimated as odds ratios (ORs) with corresponding 95% CIs derived from the GLMM parameter estimates. The Wilcoxon rank-sum test was used to compare the 2 treatment groups in the percent time with meaningful CSI improvement across all observed assessments from months 3 to 12. Across this interval, the rate of missing visits per assessment occasion was low and comparable across the treatment arms (1.7%–7.9% in the active VNS group, 5.6%–13.7% in the sham VNS group). Similar analyses tested whether the treatment arms differed in the proportion of participants who achieved remission of SI. For those without meaningful SI at baseline (CSI <3), the same analytic strategy was used to determine whether the treatment groups differed in worsening of SI (defined a priori as a CSI score increase ≥3).
The CSI scores at each time point were plotted by treatment group. The change from baseline in the continuous CSI score was analyzed using the repeated GLMM described above, applied to data from months 3 to 12, but with a normal distribution and identity link function.
An additional set of analyses was conducted using data aggregated over the 3-month period (months 10–12). The same GLMM was applied to a single time point corresponding to each participant’s average CSI score, calculated as the mean of available CSI scores across this period. The average was defined only for participants with at least 2 nonmissing monthly CSI scores; otherwise, it was set to missing.
The consistency of the treatment effect for each of the 3 SI items comprising the CSI and for every combination of 2 items was also tested. For those with SI at baseline (CSI ≥3), GLMMs were conducted over the entire observation period (3–12 months), with monthly classifications of “meaningful benefit” or “remission” serving as repeated measures. Meaningful benefit corresponded to reductions ≥2 for combinations of 2 items and ≥1 for individual items. Remission corresponded to reductions ≥2 and total score ≤1 for combinations of 2 items and a reduction ≥1 and total score ≤1 for individual items. The ORs for the main effect of treatment condition (active versus sham) were examined to assess consistency of the treatment effect.
Given the exploratory nature of these analyses and the fact that the study was neither designed nor statistically powered to detect a treatment effect on SI, no correction for multiple comparisons was applied. The reported P values and confidence intervals were accordingly presented as descriptive rather than confirmatory.
RESULTS
Characteristics of the Treatment Groups
Table 1 describes the analytic sample (N =463). Participants averaged approximately 29 years of depression (lifetime), with 13 failed antidepressant treatments. About 71.0% had treatment failures of at least 1 interventional treatment (ECT, repetitive transcranial magnetic stimulation, esketamine) in the current MDE; 40.4% of participants had attempted suicide.
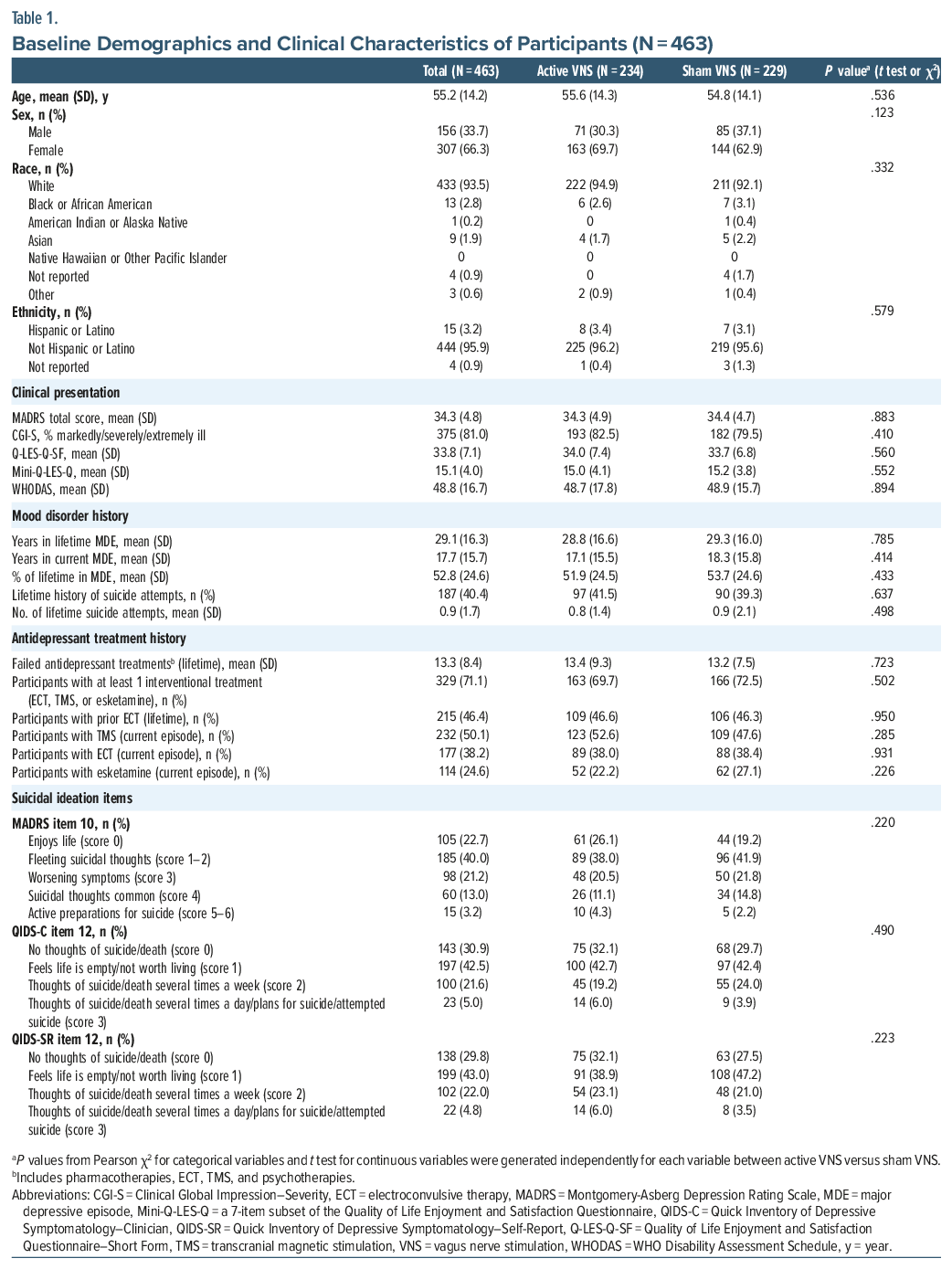
Supplementary Table 1 details degree of SI by treatment group and presence or absence of baseline SI using the CSI categorization (CSI <3 or CSI ≥3, respectively). About 62% of each treatment group had clinically meaningful baseline SI. Neither overall baseline SI (P=.79) nor category of CSI severity (eg, minimal/none, mild, moderate, and severe; P=.59) distinguished the 2 treatment groups. For the entire analytic sample and for participants with and without significant baseline SI, the treatment groups were similar in demographic, treatment history, and clinical features at baseline. Similarly, in those with meaningful baseline SI, there were no between-treatment-group differences in baseline CSI, whether by total CSI score or CSI category of severity.
Effects of VNS on Clinically Meaningful Baseline SI (CSI ≥3)
Figure 1 shows the average monthly CSI scores for months 3–12 for participants with meaningful baseline SI. Both the active and sham VNS treatment groups demonstrated a substantial decline in overall CSI score starting at month 3. By month 12, the mean (SD) drop in CSI score was 2.42 (0.19) for the active VNS group and 2.12 (0.19) for the sham VNS group. There was a trend for the effect of treatment group in the GLMM (P = .091). The treatment-by-visit interaction was not statistically significant (P = .953), while the visit effect across both treatments was significant (P<.001), with reductions increasing from months 3 to 12.
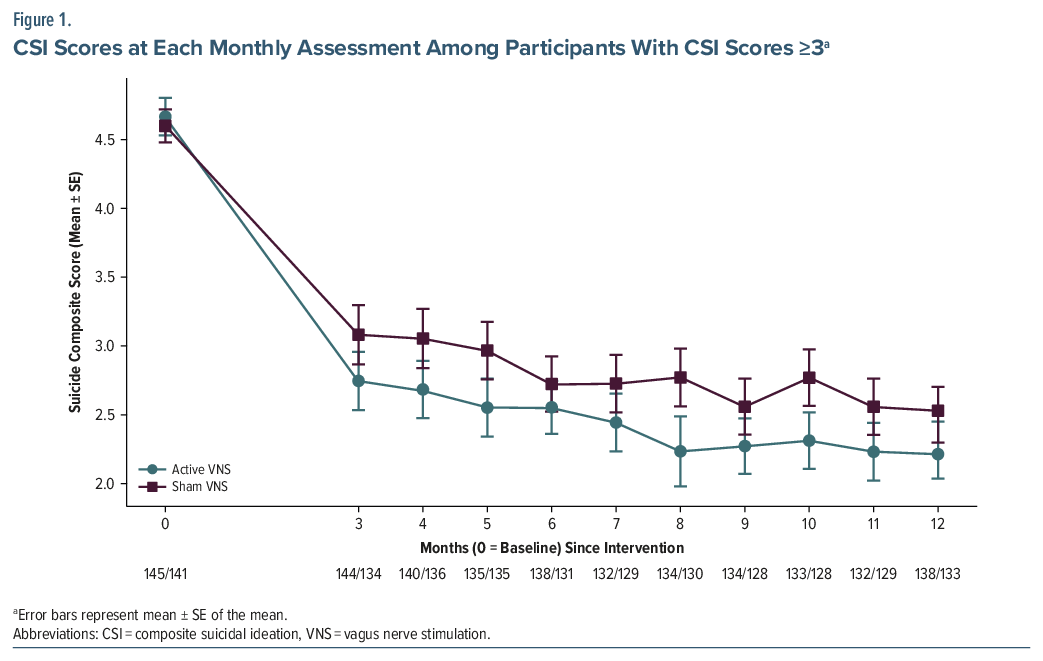
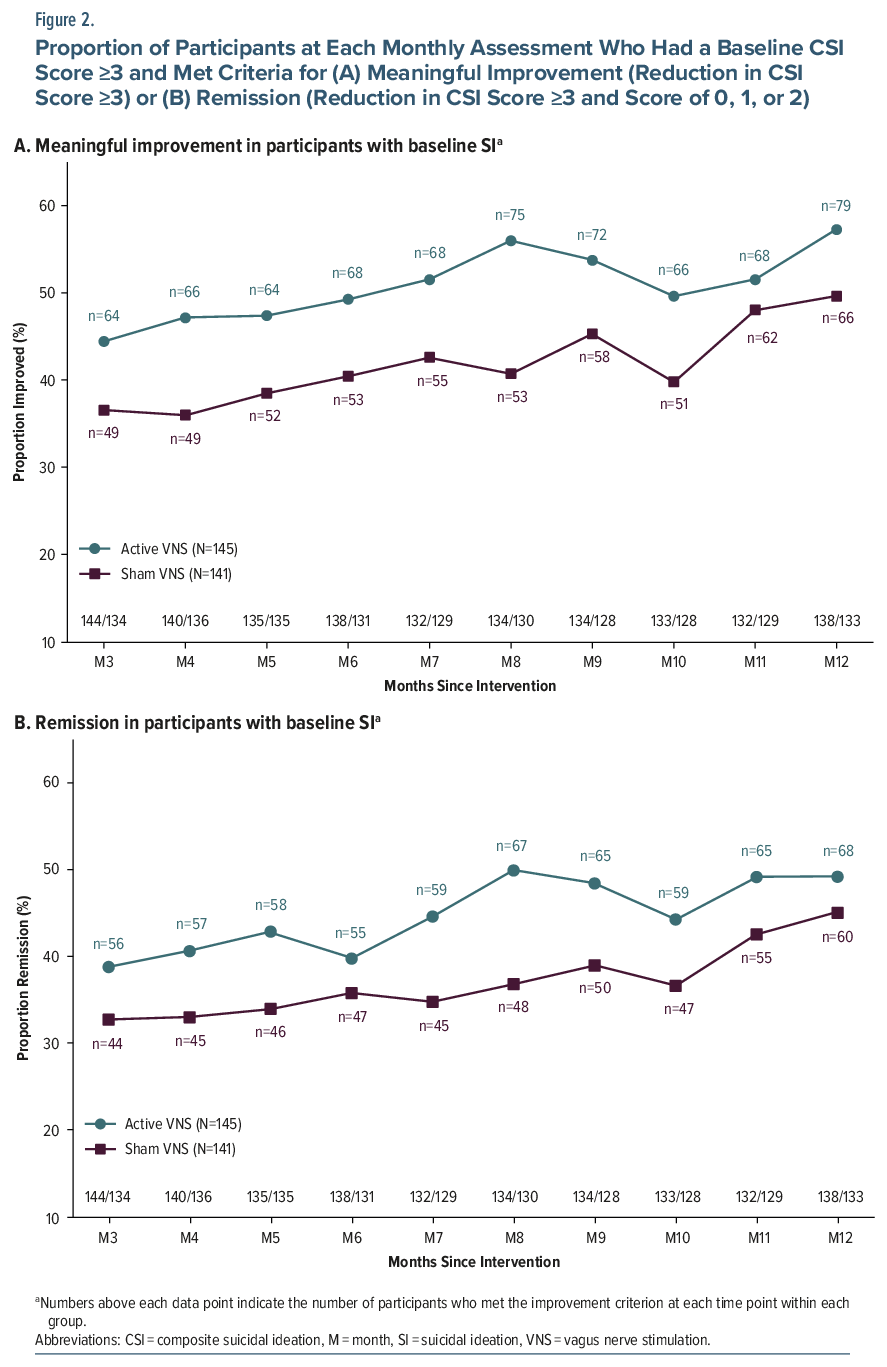
Figure 2, Panel A, and Supplementary Table 2 present the number and proportion of participants with a clinically meaningful change in SI (≥3 CSI points) at each monthly assessment. Compared to those in the sham VNS group (n = 141), participants in the active VNS group (n = 145) had more months in clinically meaningful improvement in SI during the 12-month study period, with consistent separation through the observation period (Figure 2, Panel A). The repeated measures GLMM indicated that the active VNS group had a statistically significant advantage over the sham VNS group in time in meaningful improvement across the entire 10-month observation period (OR = 1.43; 95% CI, 1.004–2.021; P = .047; Table 2). The treatment-by-visit interaction was not significant (P = .991), indicating that the treatment group difference was consistent across time. Similar analyses of rates of categorical improvement performed on the average score for the last 3 months (months 10–12) favored active VNS numerically but were not statistically significant (Table 2). It should be noted that differences in mean CSI scores between the active and sham groups were not statistically significant at any time point.
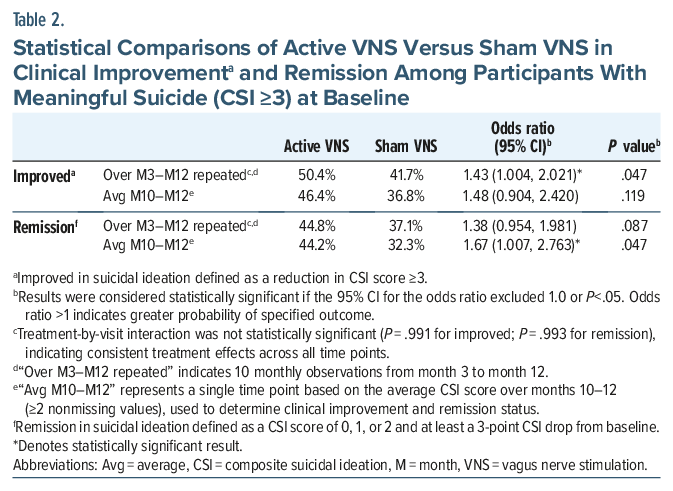
Attaining Minimal to No SI (“Remission”) for Those With Meaningful Baseline SI
Figure 2, Panel B, and Supplementary Table 2 show the percentage of participants who began treatment with meaningful baseline SI whose SI remitted (CSI score of 0, 1, or 2 and at least a 3-point CSI score drop from baseline). Active and sham VNS did not differ in the observed number of months achieving remission over the full 12 months (OR = 1.38; 95% CI, 0.954–1.981; P = .087). However, those in active VNS had significantly more months in remission than those in sham VNS for months 10–12 (OR = 1.67; 95% CI, 1.007–2.763; P = .047; Table 2).
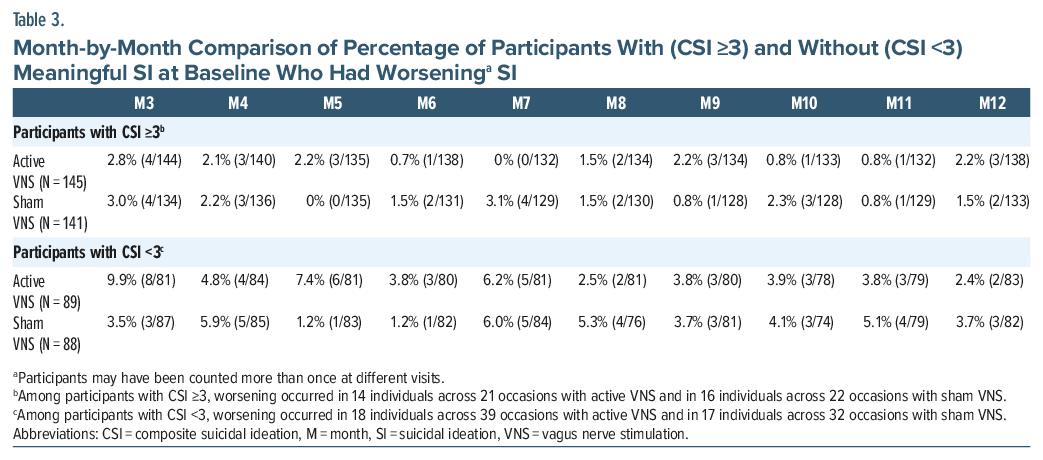
Worsening SI Regardless of Initial Degree of SI
For those starting with meaningful SI (CSI ≥3), the number of cases of worsening was limited. No meaningful difference between active and sham VNS was identified (Table 3). A substantial proportion of participants in the active VNS (38.4%) and sham VNS (38.0%) groups had no clinically meaningful baseline SI (CSI ≤2; Supplementary Table 1). Among the participants without initial SI, the emergence of meaningful SI (an increase of 3 or more points in CSI score) during the trial was infrequent in both treatment conditions. There was no difference in emergence of clinically meaningful SI over the 12-month study period in participants without clinically meaningful SI at baseline (OR = 1.24; 95% CI, 0.49–3.11; P = .650).
Individual Scale and 2-Scale Combination Consistency
Supplementary Figure 1 documents that, regardless of the measure employed (single depression scale suicide item or any 2-scale combination), active VNS consistently reduced SI more than sham VNS over months 3–12. Effect sizes ranged from 1.31 to 1.49 for meaningful or better improvement and from 1.27 to 1.46 for remission.
Mortality During the Trial
There were 6 deaths during the 1-year randomized controlled trial (RCT) phase: 4 in the VNS ON group (1 suicide completion) and 2 in the VNS OFF group (2 suicide completions).22
DISCUSSION
In the context of limited treatment options for SI and behaviors, especially among patients with markedly TRD, this exploratory study yielded 3 key findings. First, as compared to adjunctive sham VNS, adjunctive active VNS reduced SI for participants with SI at baseline. Second, for these same participants, VNS was associated with a higher likelihood of resolution of ideation (remission) in months 10–12. Third, active VNS did not worsen SI in those with SI initially, nor did SI emerge in participants who initiated treatment without SI.
Prior research on the effect of VNS therapy on suicide and SI is limited to secondary exploratory analyses of VNS trials. Nahas et al39 found 3 suicide attempts among 60 participants over 24 months; Rush et al40 noted 1 death by suicide and 7 attempts in 235 participants. In a European VNS TRD trial, Bajbouj et al41 documented 2 suicide deaths and 2 attempts among 74 participants; Aaronson et al,42 in a VNS dose-finding trial, reported 2 suicide deaths (1 each in the low- and high-dose groups) and numerically higher rates of attempts and worsening depression in the low-dose group (6.3% and 7.2%, respectively) across 331 participants. Finally, in a 60-month registry study, Aaronson et al20 showed that VNS + TAU led to greater reduction in SI than TAU alone, achieving statistical significance with 2 of the 3 SI scales. Completed suicides were arithmetically lower in the VNS + TAU group vis-à-vis TAU (1.01 per 1000 person-years [95% CI, 0.11–3.64] and 2.20 per 1000 person-years [95% CI, 0.24–7.79], respectively).
Few pharmacologic and interventional treatments have substantive effects on SI.43 ECT is the gold-standard treatment for TRD.44,45 Recently, several large registry studies and meta-analyses have documented that, compared to non-ECT controls, participants treated with ECT have reduced rates of all-cause mortality and, specifically, mortality due to suicide.15,46 ECT has also been shown to result in rapid, acute effects on SI and suicidal intent.16,47 Pharmacologic agents with antisuicidal effects in participants with MDD include racemic ketamine, lithium, and clozapine. Racemic ketamine, in particular, has shown improvements in SI in RCTs.48,49 Esketamine, FDA-approved for TRD and MDD with acute SI or behavior, has had less consistent effects. In some trials, esketamine improved depressive symptoms without significant improvement in SI.50,51
Of psychotropic agents, lithium has been most touted for its antisuicidal properties (ie, effects on ideation, behaviors, and completed suicide), and meta-analyses have sought to document this benefit. These analyses, however, have been heterogeneous, combining RCTs with retrospective and ecological studies that were variable in study duration, phase of illness, and methods.52 A meta-analysis from Cipriani et al53 on unipolar depression, bipolar disorder, schizoaffective disorder, dysthymia, and rapid cycling examined 48 RCTs (double-blind, single-blind, or open) and found that lithium was more effective than placebo in reducing suicide and all-cause mortality. The few RCTs that have prospectively examined the antisuicidal properties of lithium were less favorable. Oquendo et al54 prospectively compared lithium versus valproate in patients with bipolar depression or mixed episodes with prior suicide attempts and found no difference in time to suicide attempts/events. Similarly, Katz et al55 examined lithium + TAU and placebo + TAU in veterans with bipolar disorder or unipolar depression, stratified into those with recent suicide attempts and those without. This study was discontinued due to futility, as no difference in suicide-related events was detected.55 Clozapine is the only antipsychotic medication indicated for the treatment of recurrent suicidal behavior in schizophrenia and schizoaffective disorder, with randomized controlled and naturalistic studies demonstrating its superiority over other agents.9,56,57 In summary, there are limited options available to address SI, particularly in patients who are chronically ill and those with markedly TRD.
This study has several limitations. The findings may not generalize to those with suicidal intent. RECOVER excluded participants with severe suicidal intent/behavior at baseline to minimize risk of suicide in a blinded trial with a 12-month period of sham intervention (with TAU). Second, the CSI, a novel index developed for this report, has not been validated in other contexts. The CSI was used to classify outcomes as improved, unchanged, or worsened, based on a 3-point or greater change in scores relative to baseline. These categorical outcomes were intended to reflect meaningful change in each patient, but their validity requires further investigation.
To summarize, compared to adjunctive sham VNS, for patients with markedly TRD and baseline clinically meaningful SI, adjunctive VNS may effectively reduce SI. It does not appear to meaningfully worsen SI, if present at baseline. It also is unlikely to precipitate the onset of meaningful SI, if absent at baseline.
Article Information
Published Online: July 8, 2026. https://doi.org/10.4088/JCP.25m16296
© 2026 Physicians Postgraduate Press, Inc.
Submitted: December 23, 2025; accepted May 13, 2026.
To Cite: Hristidis VC, De Leon V, Van Der Vaart AD, et al. Impact of vagus nerve stimulation on suicidal ideation in markedly treatment-resistant major depression: a RECOVER study report. J Clin Psychiatry 2026;87(3):25m16296.
Author Affiliations: Department of Psychiatry, Washington University in St. Louis, St. Louis, Missouri (Hristidis, De Leon, Gott, Kriedt, Conway); Institute for Advanced Diagnostics and Therapeutics, Sheppard Pratt Health System, Baltimore, Maryland (Van Der Vaart, Aaronson); Department of Psychiatry, Medical University of South Carolina, Charleston, South Carolina (Sackeim); Duke-NUS Medical School, Singapore (Rush); Curbstone Consultant LLC, Dallas, Texas (Rush); LivaNova PLC (or a subsidiary), London, United Kingdom (Bunker, Lee, Gordon, Shy, Tran); Seattle Neuropsychiatric Treatment Center, Seattle, Washington (Allen); UPenn Perelman School of Medicine, Philadelphia, Pennsylvania (Sheline); University of Minnesota, Department of Psychiatry, Minneapolis, Minnesota (Nahas); Center for Anxiety and Depression, Mercer Island, Washington (Dunner); Center for Interventional Psychiatry, Faillace Department of Psychiatry and Behavioral Sciences, McGovern Medical School, The University of Texas Health Science Center at Houston, Houston, Texas (Quevedo); Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, Atlanta, Georgia (Riva-Posse); Department of Psychiatry and Behavioral Sciences, Rush University Medical Center, Chicago, Illinois (Zajecka); Psychiatric Medicine Associates, LLC, Skokie, Illinois (Zajecka); Department of Psychiatry, Huntsman Mental Health Institute, University of Utah, Salt Lake City, Utah (Mickey); Alivation Research, Lincoln, Nebraska (Duffy); Perelman School of Medicine, University of Pennsylvania, Philadelphia, Pennsylvania (Oquendo).
Corresponding Author: Charles R. Conway, MD, Washington University in St. Louis, 600 South Taylor Ave, Ste 122, St. Louis, MO 63110 ([email protected]).
Notice of Correction 7/9/26: The funding/support statement has been corrected to include support to Dr Hristidis through National Institutes of Health grant R25MH112473.
Relevant Financial Relationships: Dr Sackeim serves as a scientific advisor and receives consulting fees from Cerebral Therapeutics, Holmusk Technologies, LivaNova, MECTA, Neumarker, NeuroInsights, Neurolief, Neuronetics, Parow Entheobiosciences, and SigmaStim; receives honoraria and royalties from Cambridge University Press, Elsevier, and Oxford University Press; is the inventor of nonremunerative US patents for focal electrically administered seizure therapy (FEAST), titration in the current domain in electroconvulsive therapy (ECT), and the adjustment of current in ECT devices, each held by SigmaStim LLC; and is also the originator of magnetic seizure therapy (MST). Dr Rush has received consulting fees from Better Up, Inc., Beckley Psytech Inc., Compass Inc., Curbstone Consultant LLC, Emmes Corp., Evecxia Therapeutics, Inc., Holmusk Technologies, Inc., ICON, PLC, Johnson & Johnson (Janssen), LivaNova, MindStreet, Inc., Neurocrine Biosciences Inc., and Otsuka-US; speaking fees from LivaNova and Johnson & Johnson (Janssen); and royalties from Wolters Kluwer Health, Guilford Press, and the University of Texas Southwestern Medical Center, Dallas, TX (for the Inventory of Depressive Symptomology and its derivatives); he is also named co-inventor on 2 patents: US Patent No. 7,795,033: Methods to Predict the Outcome of Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S, Wilson AS; and US Patent No. 7,906,283: Methods to Identify Patients at Risk of Developing Adverse Events During Treatment with Antidepressant Medication, Inventors: McMahon FJ, Laje G, Manji H, Rush AJ, Paddock S. Dr Aaronson is a consultant to Genomind, Janssen, LivaNova, Neuronetics, and Sage Therapeutics and has received research support from Compass Pathways and Neuronetics. Dr Bunker is a former employee of and current consultant for LivaNova. Dr Allen has received research support from LivaNova, Compass Pathways, MindMed, Transcend Therapeutics, Wave Neuroscience, Magnus Medical, Janssen, Kernel, Usona Institute, and Alto Neuroscience and has served on the advisory board for LivaNova and consulted for Starfish Neuroscience. Dr Nahas is a consultant to LivaNova, Magnus Medical, and Motif and has also received research support from LivaNova. Dr Dunner receives payment for clinical services for a former research patient from LivaNova, is a speaker for Janssen (esketamine nasal spray), and conducts forensic consultations, independent medical evaluations, and legal testimony for various firms. Ms Lee, Mr Gordon, Ms Shy, and Ms Tran are employees of LivaNova. Ms Lee, Mr Gordon, and Ms Shy hold LivaNova stock. Dr Quevedo receives clinical research support from LivaNova, Neumora Therapeutics, and Johnson & Johnson; has been a consultant for LivaNova; and receives copyrights from Artmed Editora, Artmed Panamericana, and Elsevier/Academic Press. Dr Riva-Posse is a consultant for LivaNova, Janssen Pharmaceuticals, Motif Neurotech, and Abbott Neuromodulation. Dr Zajecka receives research support from Boehringer Ingelheim, Compass Pathways, Hoffman LaRoche, Johnson & Johnson (Janssen), LivaNova, Otsuka, Neurocrine Bioscience, and Sage Therapeutics and has received consulting fees from Alfasigma USA and Johnson & Johnson (Janssen). Dr Mickey has received research support from NIH, NSF, Wellcome Leap, PCORI, Health Rhythms, LivaNova, Compass, and Abbott and consulting fees from Inside Edge, VML, Atheneum, Guidepoint, Kx Advisors, and S2N Health. Dr Duffy has received research support from Abbott Nutrition, AbbVie, Acadia, Akili, Alkermes, Allergan, Alto Neuroscience, AriBio, Axsome, Biohaven, Bionomics, Clexio, Compass Pathways, Corcept, Corium, Denovo Biopharma, Emalex, GlaxoSmithKline Biologicals, Hoffmann-LaRoche, Intra-Cellular, Ironshore, Janssen, Jazz, LivaNova, Lumos, Merck Sharp & Dohme, Neurocrine Biosciences, NRx, Otsuka, Sage Therapeutics, Sanofi Pasteur, Shire, Sirtsei, Spark Neuro, Sumitomo, Sunovion, and Supernus. He is on a speakers bureau or advisory board or is a consultant for Abbott Neuromodulation, Corium, and LivaNova. Dr Oquendo receives royalties from the Research Foundation for Mental Hygiene for the commercial use of the Columbia Suicide Severity Rating Scale. She serves as an advisor to Mind Medicine (pro bono), and Fundacion Jimenez Diaz. She reviews grants for Alkermes, and her family formerly owned stock in Bristol Myers Squibb (sold March 2024). Dr Conway has received research support from the American Foundation for Suicide Prevention, Assurex Health, August Busch IV Foundation, Barnes-Jewish Hospital Foundation, LivaNova, National Institute of Mental Health, and the Taylor Family Institute for Innovative Psychiatric Research and has also consulted for LivaNova. Drs Hristidis, De Leon, Van Der Vaart, and Sheline; Ms Gott; and Mr Kriedt have no conflicts to declare.
Funding/Support: This work was supported by LivaNova PLC, the developer and manufacturer of the Vagus Nerve Stimulation Therapy system. Conducting the study, analyzing the data, and drafting the report were supported by LivaNova PLC. Conducting the study was also supported by the Centers for Medicare & Medicaid Services. Dr Hristidis received support through National Institutes of Health grant R25MH112473.
Role of the Sponsor: Final approval of the content of this manuscript and the decision to submit it were determined solely by the authors, some of whom are affiliated with LivaNova PLC.
Acknowledgments: The authors are deeply grateful to the patients and their families for participating in the RECOVER study. We greatly appreciate the Centers for Medicare & Medicaid Services for providing financial support for the Vagus Nerve Stimulation Therapy system devices and implantation surgeries. The authors thank Zeeba Kabir, PhD, and Paul Cao, PhD, of Simpson Healthcare, for their editorial assistance in accordance with the Good Publication Practice 2022 guidelines, which was supported by LivaNova PLC.
The authors also thank the RECOVER Study Group: Advanced Mental Health Care, Palm Beach, FL; Alivation Research, Lincoln, NE; AMR Baber Research, Naperville, IL; APG Research, Orlando, FL; ATP Clinical Research, Costa Mesa, CA; Barnes-Jewish Hospital, St Louis, MO; Beacon Medical Group Behavioral Health South Bend, South Bend, IN; Carilion Clinic, Roanoke, VA; Center for Anxiety and Depression, Mercer Island, WA; Center for Neuropsychiatry and Brain Stimulation, Durham, NC; Charak Center for Health and Wellness, Garfield Heights, OH; DENT Neurologic Institute, Amherst, NY; Emory University, Atlanta, GA; Florida Behavioral Medicine, Largo, FL; Florida Center for TMS, Orlando, FL; Florida Center for TMS, St Augustine, FL; Galiz Research, Hialeah, FL; Hapworth Research, New York, NY; Healthy Perspectives, Nashua, NH; Icahn School of Medicine at Mount Sinai, New York, NY; Kaizen Brain Center, La Jolla, CA; Marshall Psychiatry, Huntington, WV; Massachusetts General Hospital, Boston, MA; Medical College of Georgia at Augusta University, Augusta, GA; Medical University of South Carolina, Charleston, SC; Michigan Clinical Research Institute, Ann Arbor, MI; Mindful Behavioral Health, Boca Raton, FL; Neuropsychiatric Associates at Woodstock Research Center, Woodstock, VT; NeuroScience and TMS Treatment Center, Brentwood, TN; Northwest Behavioral Research Center, Marietta, GA; Nova Psychiatry, Orlando, FL; Offices of Psychiatry & Counseling Services, Moosic, PA; Ohio State University, Columbus, OH; OU Physicians, Tulsa, OK; Precise Research Centers, Flowood, MS; PsychCare Consultants Research, St Louis, MO; Psychiatry Care and Research Center, O’Fallon, MO; Rush University Medical Center, Chicago, IL; Seattle Neuropsychiatric Treatment Center, Seattle, WA; SF-Care, San Rafael, CA; Sheppard Pratt Health Systems, Baltimore, MD; Signature Research Associates, Fairlawn, OH; Southern Illinois University School of Medicine, Springfield, IL; Stedman Clinical Trials, Tampa, FL; Stony Brook University Hospital, Stony Brook, NY; Syrentis Clinical Research, Santa Ana, CA; Texas Tech University Health Science Center, El Paso, TX; Trinity Medical, Lewiston, NY; UC San Diego, San Diego, CA; University of Alabama Heersink School of Medicine, Birmingham, AL; University of Alabama Huntsville Regional Medical Center, Huntsville, AL; University of Minnesota, Minneapolis, MN; University of Missouri, Columbia, MO; University of Utah Neuropsychiatric Institute, Salt Lake City, UT; University of Wisconsin, Madison, WI; UPenn Perelman School of Medicine, Philadelphia, PA; USC Keck School of Medicine, Los Angeles, CA; UT Dell Medical School, Austin, TX; and UT McGovern Medical School, Houston, TX.
ORCID: Vasilis C. Hristidis, MD: https://orcid.org/0000-0003-1442-6507; Victoria De Leon, MD: https://orcid.org/0000-0002-5811-2086; Andrew D. Van Der Vaart, MD: https://orcid.org/0000-0001-6680-6769; Harold A. Sackeim, PhD: https://orcid.org/0000-0002-1107-4553; A. John Rush, MD: https://orcid.org/0000-0003-2004-2382; Scott T. Aaronson, MD: https://orcid.org/0000-0001-7616-8801; Yvette Sheline, MD: https://orcid.org/0000-0002-6929-9659; Ziad Nahas, MD:
https://orcid.org/0000-0002-8391-5673; João Quevedo, MD: https://orcid.org/0000-0003-3114-6611; Patricio Riva-Posse, MD: https://orcid.org/0000-0002-5887-0557; John Zajecka, MD: https://orcid.org/0000-0001-8398-636X; Brian J. Mickey, MD: https://orcid.org/0000-0002-7847-7680; Walter Duffy, MD: https://orcid.org/0009-0006-5261-9659; Maria A. Oquendo, MD: https://orcid.org/0000-0002-7901-5082; Charles R. Conway, MD: https://orcid.org/0000-0001-6849-9416
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- Compared to sham vagus nerve stimulation (VNS), adjunctive active VNS was associated with reduced suicidal ideation (SI) over months 3–12 in participants with baseline SI.
- Adjunctive active VNS was associated with greater rates of SI remission in months 10–12.
- Adjunctive active VNS was unlikely to worsen SI in participants with baseline SI, or have SI emerge in those without baseline SI.
Editor’s Note: We encourage authors to submit papers for consideration as a part of our Early Career Psychiatrists section. Please contact Joseph F. Goldberg, MD at Psychiatrist.com/contact/goldberg.
References (57)

- US Department of Health and Human Services. The Surgeon General’s Call to Action to Implement the National Strategy for Suicide Prevention. 2021. Accessed April 9, 2026. https://www.hhs.gov/sites/default/files/sprc-call-to-action.pdf
- Arsenault-Lapierre G, Kim C, Turecki G. Psychiatric diagnoses in 3275 suicides: a meta-analysis. BMC Psychiatry. 2004;4:37. PubMed CrossRef
- Cavanagh JT, Carson AJ, Sharpe M, et al. Psychological autopsy studies of suicide: a systematic review. Psychol Med. 2003;33(3):395–405. PubMed CrossRef
- Henriksson MM, Aro HM, Marttunen MJ, et al. Mental disorders and comorbidity in suicide. Am J Psychiatry. 1993;150(6):935–940.
- Gronemann FH, Jorgensen MB, Nordentoft M, et al. Treatment-resistant depression and risk of all-cause mortality and suicidality in Danish patients with major depression. J Psychiatr Res. 2021;135:197–202. CrossRef
- Rhee TG, Bommersbach TJ, Rosenheck RA, et al. National trends and correlates of treatment resistance in major depressive episode and associated suicidal ideation and behaviors among adults in the United States. J Affect Disord. 2024;358:342–349. CrossRef
- Bergfeld IO, Mantione M, Figee M, et al. Treatment-resistant depression and suicidality. J Affect Disord. 2018;235:362–367. PubMed CrossRef
- Zisook S, Domingues I, Compton J. Pharmacologic approaches to suicide prevention. Focus (Am Psychiatr Publ). 2023;21(2):137–144. CrossRef
- Meltzer HY, Alphs L, Green AI, et al. Clozapine treatment for suicidality in schizophrenia: International Suicide Prevention Trial (InterSePT). Arch Gen Psychiatry. 2003;60(1):82–91.
- Hochschild A, Grunebaum MF, Mann JJ. The rapid anti-suicidal ideation effect of ketamine: a systematic review. Prev Med. 2021;152(pt 1):106524. CrossRef
- Goodwin FK, Fireman B, Simon GE, et al. Suicide risk in bipolar disorder during treatment with lithium and divalproex. JAMA. 2003;290(11):1467–1473. PubMed CrossRef
- Hayes JF, Pitman A, Marston L, et al. Self-harm, unintentional injury, and suicide in bipolar disorder during maintenance mood stabilizer treatment: a UK population-based electronic health records study. JAMA Psychiatry. 2016;73(6):630–637.
- Lewitzka U, Severus E, Bauer R, et al. The suicide prevention effect of lithium: more than 20 years of evidence—a narrative review. Int J Bipolar Disord. 2015;3(1):32. PubMed CrossRef
- Kaster TS, Blumberger DM, Gomes T, et al. Risk of suicide death following electroconvulsive therapy treatment for depression: a propensity score-weighted, retrospective cohort study in Canada. Lancet Psychiatry. 2022;9(6):435–446. CrossRef
- Rönnqvist I, Nilsson FK, Nordenskjöld A. Electroconvulsive therapy and the risk of suicide in hospitalized patients with major depressive disorder. JAMA Netw Open. 2021;4(7):e2116589. CrossRef
- Kellner CH, Fink M, Knapp R, et al. Relief of expressed suicidal intent by ECT: a Consortium for Research in ECT study. Am J Psychiatry. 2005;162(5):977–982. PubMed CrossRef
- Stone M, Laughren T, Jones ML, et al. Risk of suicidality in clinical trials of antidepressants in adults: analysis of proprietary data submitted to US Food and Drug Administration. BMJ. 2009;339:b2880. PubMed CrossRef
- Friedman RA. Antidepressants’ black-box warning—10 years later. N Engl J Med. 2014;371(18):1666–1668. PubMed CrossRef
- Olin B, Jayewardene AK, Bunker M, et al. Mortality and suicide risk in treatment-resistant depression: an observational study of the long-term impact of intervention. PLoS One. 2012;7(10):e48002. PubMed CrossRef
- Aaronson ST, Sears P, Ruvuna F, et al. A 5-year observational study of patients with treatment-resistant depression treated with vagus nerve stimulation or treatment as usual: comparison of response, remission, and suicidality. Am J Psychiatry. 2017;174(7):640–648. PubMed CrossRef
- A prospective, multi-center, randomized controlled blinded trial demonstrating the safety and effectiveness of VNS Therapy® system as adjunctive therapy versus a no stimulation control in subjects with treatment-resistant depression (RECOVER). Accessed October 9, 2025. https://clinicaltrials.gov/study/NCT03887715?term=NCT03887715&rank=1
- Conway CR, Aaronson ST, Sackeim HA, et al. Vagus nerve stimulation in treatment-resistant depression: a one-year, randomized, sham-controlled trial. Brain Stimul. 2025;18(3):676–689. CrossRef
- Rush AJ, Conway CR, Aaronson ST, et al. Effects of vagus nerve stimulation on daily function and quality of life in markedly treatment-resistant major depression: findings from a one-year, randomized, sham-controlled trial. Brain Stimul. 2025;18(3):690–700. CrossRef
- Conway CR, Rush AJ, Gordon C, et al. An examination of symptoms, function and quality of life as conjoint clinical outcome domains for treatment-resistant depression. J Mood Anxiety Disord. 2025;10:100121. CrossRef
- Weissman CR, Stapper N, Valmadrid LC, et al. Suicidal ideation as a risk factor for suicide: insights from hypertension screening. J Affect Disord. 2025;393(pt B):120501.
- McHugh CM, Corderoy A, Ryan CJ, et al. Association between suicidal ideation and suicide: meta-analyses of odds ratios, sensitivity, specificity and positive predictive value—Erratum. BJPsych Open. 2019;5(2):e24. CrossRef
- Nock MK, Borges G, Bromet EJ, et al. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–154.
- Louzon SA, Bossarte R, McCarthy JF, et al. Does suicidal ideation as measured by the PHQ-9 predict suicide among VA patients? Psychiatr Serv. 2016;67(5):517–522. PubMed CrossRef
- Ballard ED, Fields J, Farmer CA, et al. Clinical trials for rapid changes in suicidal ideation: lessons from ketamine. Suicide Life Threat Behav. 2021;51(1):27–35. CrossRef
- Perroud N, Aitchison KJ, Uher R, et al. Genetic predictors of increase in suicidal ideation during antidepressant treatment in the GENDEP project. Neuropsychopharmacology. 2009;34(12):2517–2528. PubMed CrossRef
- Ballard ED, Luckenbaugh DA, Richards EM, et al. Assessing measures of suicidal ideation in clinical trials with a rapid-acting antidepressant. J Psychiatr Res. 2015;68:68–73. PubMed CrossRef
- Nunnally JC. Psychometric Theory. McGraw Hill; 1967.
- Conway CR, Aaronson ST, Sackeim HA, et al. Clinical characteristics and treatment exposure of patients with marked treatment-resistant unipolar major depressive disorder: a RECOVER trial report. Brain Stimul. 2024;17(2):448–459. CrossRef
- Conway CR, Olin B, Aaronson ST, et al. A prospective, multi-center randomized, controlled, blinded trial of vagus nerve stimulation for difficult to treat depression: a novel design for a novel treatment. Contemp Clin Trials. 2020;95:106066. PubMed CrossRef
- Sackeim HA, Aaronson ST, Bunker MT, et al. Update on the assessment of resistance to antidepressant treatment: rationale for the Antidepressant Treatment History Form: Short Form-2 (ATHF-SF2). J Psychiatr Res. 2024;176:325–337. CrossRef
- Montgomery SA, Asberg M. A new depression scale designed to be sensitive to change. Br J Psychiatry. 1979;134:382–389. PubMed CrossRef
- Sackeim HA, Conway CR, Aaronson ST, et al. Characterizing the effects of vagus nerve stimulation on symptom improvement in markedly treatment-resistant major depressive disorder: a RECOVER trial report. J Affect Disord. 2025;380:135–145. CrossRef
- Berry SM, Broglio K, Bunker M, et al. A patient-level meta-analysis of studies evaluating vagus nerve stimulation therapy for treatment-resistant depression. Med Devices (Auckl). 2013;6:17–35. PubMed CrossRef
- Nahas Z, Marangell LB, Husain MM, et al. Two-year outcome of vagus nerve stimulation (VNS) for treatment of major depressive episodes. J Clin Psychiatry. 2005;66(9):1097–1104. PubMed CrossRef
- Rush AJ, Marangell LB, Sackeim HA, et al. Vagus nerve stimulation for treatment- resistant depression: a randomized, controlled acute phase trial. Biol Psychiatry. 2005;58(5):347–354. PubMed CrossRef
- Bajbouj M, Merkl A, Schlaepfer TE, et al. Two-year outcome of vagus nerve stimulation in treatment-resistant depression. J Clin Psychopharmacol. 2010;30(3):273–281. PubMed CrossRef
- Aaronson ST, Carpenter LL, Conway CR, et al. Vagus nerve stimulation therapy randomized to different amounts of electrical charge for treatment-resistant depression: acute and chronic effects. Brain Stimul. 2013;6(4):631–640. PubMed CrossRef
- Fox KR, Huang X, Guzman EM, et al. Interventions for suicide and self-injury: a meta-analysis of randomized controlled trials across nearly 50 years of research. Psychol Bull. 2020;146(12):1117–1145. PubMed CrossRef
- Espinoza RT, Kellner CH. Electroconvulsive therapy. N Engl J Med. 2022;386(7):667–672.
- Sackeim HA. Modern electroconvulsive therapy: vastly improved yet greatly underused. JAMA Psychiatry. 2017;74(8):779–780.
- Odermatt J, Sarlon J, Schaefer N, et al. Electroconvulsive therapy reduces suicidality and all-cause mortality in refractory depression: a systematic review and meta-analysis of neurostimulation studies. Neurosci Appl. 2025;4:105520. CrossRef
- Prudic J, Sackeim HA. Electroconvulsive therapy and suicide risk. J Clin Psychiatry. 1999;60(suppl 2):104–110.
- Grunebaum MF, Galfalvy HC, Choo TH, et al. Ketamine for rapid reduction of suicidal thoughts in major depression: a midazolam-controlled randomized clinical trial. Am J Psychiatry. 2018;175(4):327–335. CrossRef
- Fan W, Yang H, Sun Y, et al. Ketamine rapidly relieves acute suicidal ideation in cancer patients: a randomized controlled clinical trial. Oncotarget. 2017;8(2):2356–2360. PubMed CrossRef
- Fu DJ, Ionescu DF, Li X, et al. Esketamine nasal spray for rapid reduction of major depressive disorder symptoms in patients who have active suicidal ideation with intent: double-blind, randomized study (ASPIRE I). J Clin Psychiatry. 2020;81(3):19m13191.
- Ionescu DF, Fu DJ, Qiu X, et al. Esketamine nasal spray for rapid reduction of depressive symptoms in patients with major depressive disorder who have active suicide ideation with intent: results of a phase 3, double-blind, randomized study (ASPIRE II). Int J Neuropsychopharmacol. 2021;24(1):22–31. CrossRef
- Del ML, Muscas M, Murru A, et al. Lithium and suicide prevention in mood disorders and in the general population: a systematic review. Neurosci Biobehav Rev. 2020;116:142–153.
- Cipriani A, Hawton K, Stockton S, et al. Lithium in the prevention of suicide in mood disorders: updated systematic review and meta-analysis. BMJ. 2013;346:f3646. PubMed CrossRef
- Oquendo MA, Galfalvy HC, Currier D, et al. Treatment of suicide attempters with bipolar disorder: a randomized clinical trial comparing lithium and valproate in the prevention of suicidal behavior. Am J Psychiatry. 2011;168(10):1050–1056. PubMed CrossRef
- Katz IR, Rogers MP, Lew R, et al. Lithium treatment in the prevention of repeat suicide-related outcomes in veterans with major depression or bipolar disorder: a randomized clinical trial. JAMA Psychiatry. 2022;79(1):24–32. PubMed CrossRef
- Lee BJ, Cotes RO, Mojtabai R, et al. The protective effect of clozapine on suicide: a population mortality study of statewide autopsy records in Maryland. J Clin Psychiatry. 2023;84(3):22m14587.
- Hennen J, Baldessarini RJ. Suicidal risk during treatment with clozapine: a meta-analysis. Schizophr Res. 2005;73(2-3):139–145. PubMed CrossRef
This PDF is free for all visitors!