Have you ever wondered why metastatic brain lesions can result in affective, behavioral, and cognitive symptoms? Would you be surprised to learn that this symptom cluster can arise due to lesions in the cerebellum? Have you been uncertain about how best to manage these manifestations? If you have, the following case vignette and discussion should prove useful.
CASE VIGNETTE
Mr D, a 72-year-old man with benign prostatic hyperplasia, tobacco use disorder, and depression, presented to the emergency department (ED) with 2 weeks of fatigue, polydipsia, polyuria, insomnia, anorexia, weight loss, and shortness of breath on exertion. During his initial evaluation, computed tomography scans of his head, chest, abdomen, and pelvis revealed a bevy of lesions in his liver, right lung, thoracic spine, and the right side of his cerebellum (a 2.8 x 2.6–cm lesion with mass effect into the right peduncle), concerning for metastatic disease. Although he was urged to undergo additional workup and treatment in the hospital, he elected to leave the hospital against medical advice with a plan to follow up in the outpatient neurosurgery clinic. One week after discharge, he arrived at the neurosurgery clinic with worsening confusion, disorganized thoughts, paranoia, mood lability, irritability, anger, and aggression directed toward his wife. He was sent to the ED for further evaluation.
Although Mr D understood that he had lesions in his liver, spine, lungs, and brain, he was unable to appreciate the risks of leaving the hospital again without further workup. Moreover, he was paranoid and agitated and demonstrated worsening cognition. Mr D’s wife noted that he had not been paying their mortgage bills nor their homeowner’s insurance for several months prior to his hospital admission.
On mental status examination, he revealed paranoid delusions, tangential thinking, and episodic disorganization. However, he was alert and oriented to self, location, and date. He could name the days of the week backward, but he was unable to spell “world”
backward. Neurological examination showed slow, rapid alternating movements in his left hand, and he had difficulty completing these movements with his right hand. Finger-nose-finger testing was intact. He was unable to complete the Luria test, a bedside examination of executive functioning in which a patient is asked to imitate 3 specific hand gestures made by the examiner (making a fist, placing the hand with the palm facing down, and holding the hand with the edge of the hand facing down) and then complete the hand gestures in the correct sequence on their own. Laboratory studies revealed a carcinoembryonic antigen level of >47,000 ng/mL, transaminitis, hypoalbuminemia, a normal ammonia level, negative serum autoimmune and paraneoplastic panels, a negative rheumatoid factor, a negative antinuclear antibody, and a urinalysis without evidence of infection.
A biopsy of his liver mass led to a diagnosis of non–small cell lung cancer (NSCLC). His cognitive and affective symptoms were attributed to cerebellar cognitive affective syndrome (CCAS) secondary to his right medial cerebellar lesion.
DISCUSSION
What Contributes to the Development of Brain Metastases?
Brain metastases are a common and serious complication of systemic cancers that occur in up to 40% of all people with cancer.1 Multiple steps are involved in the development of metastases including cancerous cells invading the tissue surrounding the tumor, intravasation into the blood stream, systemic hematogenous spread, arrest of the movement of the cancer cell at a specific location (this frequently includes branches in the vasculature supply), extravasation from the vasculature into the tissue, and then angiogenesis.2 Several factors play a role in metastatic spread and, potentially, to the specific location where the cancer cell metastasizes.2 These factors include specific genetic and molecular features of the cancer cell, characteristics of the microenvironments in which the cancer cell metastasizes, and systemic features.
The overall incidence of brain metastases has been increasing. This rise is multifactorial. Improvements in systemic cancer treatments have increased patient life expectancy and thus the potential for brain metastases as patients with cancer live longer.3 Another contributor is the limited ability of certain systemic treatments to cross the blood-brain barrier. Because of this, the central nervous system (CNS) has been referred to as a “sanctuary,” enabling tumor cells to proliferate within the CNS, even when there is effective systemic disease control.2,3
The most common cancers that metastasize to the brain are lung cancer, breast cancer, skin cancer (particularly melanoma), and gastrointestinal cancers. Among all primary cancer types, NSCLC most commonly often metastasizes to the brain.3 As was the case with Mr D, many individuals with NSCLC are diagnosed with a brain metastasis during their initial cancer workup, rather than later in their illness course.3,4 Unlike Mr D who had multiple metastatic lesions, among all people with NSCLC who have been diagnosed with a metastatic brain tumor, 30%–43% show no evidence of other metastatic disease.3
What Types of Neuropsychiatric Signs and Symptoms Can Develop in an Individual With Lung Cancer?
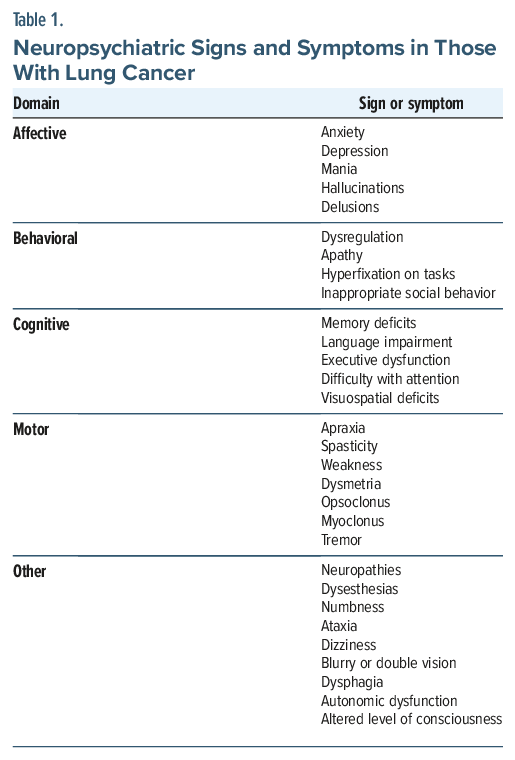
Neuropsychiatric signs and symptoms in individuals with lung cancer can include affective, behavioral, cognitive, and motor abnormalities (Table 1). The specific signs and symptoms may be due to the cancer or develop as a side effect of cancer-directed treatments. Affective and behavioral symptoms include dysregulation, apathy, hyperfixation on tasks, and inappropriate social behavior. All cognitive domains can be impacted. Neuropsychiatric signs and symptoms to monitor for include neuropathies, dysesthesias, ataxia, dizziness, blurry or double vision, dysphagia, autonomic dysfunction, and a decreased level of consciousness.5,6 Motor symptoms can also arise with specific symptoms varying depending on their cause and the location of the insult.5 Like other individuals with cancer, those with lung cancer may also develop an adjustment disorder, depression, anxiety, mania, or psychotic symptoms.
Patients with cancer who develop an acute onset of behavioral or neurological symptoms should undergo a thorough evaluation for potential contributors. Primary care providers (PCPs) should assess for changes in neurological and cognitive functioning. Mild-to moderate symptoms may benefit from referral for neuropsychological testing, which can help discriminate between potential triggers and better understand the deficits the patient is experiencing. Sudden onset of confusion, psychosis, or behavioral dysregulation, as was seen in Mr D following initial discharge from the hospital against medical advice, requires emergent evaluation with consideration of head imaging and additional workup.
Why Do Neuropsychiatric Symptoms Develop in Those With Lung Cancer?
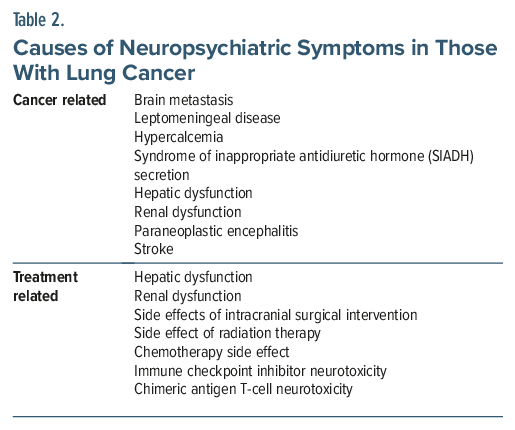
Neuropsychiatric symptoms in those with lung cancer can be triggered by cancer-related pathology or treatment-related complications (Table 2). Brain metastases, leptomeningeal disease, delirium, paraneoplastic syndromes, cancer-associated hypercalcemia, the syndrome of inappropriate antidiuretic hormone (SIADH) secretion, and hepatic or renal dysfunction secondary to malignancy or its therapies can precipitate neuropsychiatric symptoms. Brain metastases may cause neuropsychiatric symptoms via direct infiltration of the CNS, increased intracranial pressure, mass effect, and disruptions in brain network connectivity. The effects of brain metastases vary by location, although lesions may be difficult to localize if multiple metastases are present and they disrupt brain network connectivity.7 Brain metastases in the frontal lobes often present with impaired executive function, a lack of motivation, mood lability, or a lack of social awareness. Temporal lobe metastases can manifest with memory impairments, aphasia, and other cognitive deficits.7 Parietal lobe tumors may present with difficulties with spatial orientation. Occipital lobe tumors can cause visual perceptual deficits.7 Although cerebellar lesions are classically associated with ataxia and coordination problems, they can also provoke neuropsychiatric symptoms (including cognitive deficits, psychosis, and affective changes).7–9
Patients often undergo multimodal cancer treatment, which may include surgical resection, radiation therapy, chemotherapy, immunotherapy, and other cellular therapies. Surgical resection of brain metastases or radiation therapy that targets brain metastases may also induce or worsen symptoms. In general, whole brain radiation is more likely to cause cognitive impairment than is more localized and targeted radiotherapy. Chemotherapy-induced cognitive impairment (eg, deficits in attention, memory, or language skills or decreased information processing speed) is a well recognized phenomenon in those undergoing treatment for cancers of all types. Immune checkpoint inhibitors and chimeric antigen receptor T-cell (CAR T-cell) therapies can also cause neurotoxicity—ranging from mild confusion to fulminant encephalitis or immune effector cell–associated neurotoxicity syndrome—which necessitates immunomodulatory interventions.10–12
Individuals with lung cancer also experience high rates of psychosocial distress that may have a significant impact on a patient’s ability to cope with their illness and reduce their quality of life. In addition, they may experience physical and psychosocial symptoms at different stages in their cancer treatment or in tandem with it. The resultant clinical picture can be complex and include cognitive deficits, affective disturbances, behavioral dysregulation, and other neuropsychiatric symptoms. PCPs familiar with a patient’s precancer history provide important context regarding a patient’s baseline cognition and mental health. They also assist in the management of affective symptoms related to psychosocial distress secondary to a cancer diagnosis and provide referrals to specialists for further evaluation when indicated.
What Is CCAS, and When Was It First Described?
The cerebellum plays an integral role in coordination of movements, balance, and posture. Reports of behavioral anomalies associated with cerebellar injury date back to the 19th century. Functional imaging studies from the 1980s and 1990s showed activation of the cerebellum in nonmotor tasks; yet, at the time, few clinical case examples were correlated with these imaging findings, a fact that limited the identification of a circumscribed cognitive and affective syndrome associated with cerebellar pathology. Then, in 1998, Schmahmann and Sherman defined CCAS after identifying 15 cases referred to the Neurology Department at Massachusetts General Hospital over a 7-year period.8 The cases included individuals with cognitive and affective symptoms associated with cerebellar pathology. Once identified, the individuals underwent a bedside examination, imaging studies (eg, a magnetic resonance imaging scan) and an electroencephalogram, and a battery of neuropsychological studies. Through these evaluations, Schmahmann and Sherman defined CCAS by 4 qualities: disruption in executive function, impaired spatial cognition, personality change, and linguistic difficulties.8 Over the past several decades, the role of the cerebellum in cognition and affective regulation has been firmly established.
Specifically, CCAS is related to damage to lobules VI and VII and potentially lobule IX. CCAS can also result from an insult to the posterior lobe of the cerebellum. These insults include developmental abnormalities, stroke, infection, trauma, some neurodegenerative processes, and tumors.8 Interestingly, the cases that involved tumors typically developed CCAS in the postoperative period, following tumor resection. Several pediatric patients have developed CCAS postresection.13–15 Given the cerebellum’s role in coordination and its connection to cortical areas, CCAS has been conceptualized as a dysmetria of thought.8,16,17
What Might Neuropsychiatric Testing Reveal About an Individual With CCAS?
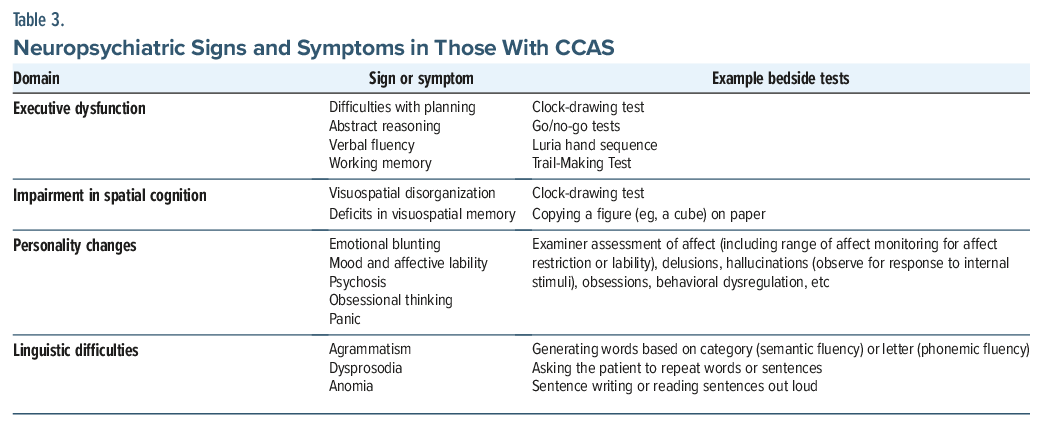
CCAS can manifest despite the absence of other cerebellar motor or vestibular syndromes (Table 3). The defining features of CCAS are deficits in executive function, impaired spatial cognition, personality change, and linguistic difficulties. Of these domains, executive dysfunction is the most widely reported in the literature. Executive dysfunction can manifest in difficulty with planning, abstract reasoning, verbal fluency, and working memory. Spatial cognition deficits include visuospatial disorganization and deficits in visuospatial memory. Linguistic difficulties can include agrammatism, dysprosody, and anomia.8 Affective and behavioral manifestations vary and include emotional blunting, affective lability, psychosis, obsessional thinking, and panic symptoms.18
How Can CCAS Be Distinguished From Other Conditions With Affective, Behavioral, Cognitive, and Motor Signs and Symptoms?
CCAS should be considered in those with posterior cerebellar pathology that impacts lobules VI and VII and possibly lobule IX. The differential diagnosis often includes delirium, treatment-related effects, primary psychiatric disorders, paraneoplastic disorders, and dementia. The presenting symptoms in each of these disorders may overlap to some extent. Clinicians should complete a thorough history of the time course of symptom development as well as the presence of associated neurological conditions, especially those that suggest cerebellar pathology (eg, ataxia). The CCAS/ Schmahmann Syndrome Scale can be used for diagnostic clarification.17 The likelihood of CCAS can be assessed based on the patient’s results in various categories: Failure in 1 test suggests possible CCAS, failure in 2 tests suggests probable CCAS, and definite CCAS is considered if a patient fails 3 or more tests.17
How Can Manifestations of CCAS Be Treated?
Addressing the underlying cerebellar injury and preventing further injury to the extent possible are priorities in managing CCAS. There is limited evidence regarding pharmacologic treatments for CCAS, and no randomized controlled trials on this disorder have been conducted. Case reports and small case series have reported on the use of donepezil and aripiprazole.19,20
Management of the affective symptoms of CCAS targets symptoms and can follow management strategies like those from other causes of an altered mental status. It begins with nonpharmacologic interventions (eg, providing reorientation; minimizing environmental stressors, such as loud noise and frequent room changes; optimizing lighting for normal sleep-wake cycles; and involving family or caregivers to provide comfort and familiarity). Ensuring adequate pain control and hydration and addressing sensory impairments (eg, with hearing aids and glasses) also help to reduce agitation.
If these measures prove insufficient or if the safety of a patient or the staff is jeopardized, a low dose of a second generation antipsychotic (eg, risperidone, quetiapine, and olanzapine) or intravenous (IV) haloperidol may be employed. Antiepileptic drugs (eg, valproic acid) can be considered an off-label practice for severe agitation that has been unresponsive to standard therapies.17
What Happened to Mr D?
Mr D’s course was complicated by intermittent agitation (which was managed with oral and intermittent IV haloperidol, as needed, when it posed an imminent risk to himself or others) and insomnia (which was managed with trazodone). He refused further workup and interventions, although he lacked the capacity to refuse these interventions given his lack of understanding of his medical conditions. Since he had no designated health care proxy, guardianship was granted through the court system. In discussion with his guardian and his family, it was determined that Mr D would have wanted a workup to diagnose his metastatic lesions. Mr D’s guardian consented to the workup that resulted in a diagnosis of NSCLC, which helped guide discussions about his prognosis and treatment options. During the workup, Mr D’s liver and kidney function worsened progressively, and treatment options were limited in the setting of his multiorgan decline. Once his diagnosis was confirmed, Mr D’s family was clear that he would not have wanted to pursue further interventions. In collaboration with the family and treatment team members, Mr D was transitioned to hospice care, and he died 7 weeks after his hospital admission.
CONCLUSION
Brain metastases are a common and serious complication of systemic cancers that occur in up to 40% of all people with cancer, related to specific genetic and molecular features of the cancer cell, systemic features, and characteristics of the microenvironments of the areas to which cancer cells spread. The cancers that most commonly metastasize to the brain are lung cancer, breast cancer, skin cancer (in particular melanoma), and gastrointestinal cancers. The differential diagnosis for neuropsychiatric symptoms present in patients with cancer includes brain metastases, delirium, paraneoplastic syndromes, treatment-related symptoms, or as a consequence of other complications related to the cancer (eg, dysfunction of other organs). When lesions arise in the cerebellum, CCAS can develop, which is manifested by deficits in executive function, impaired spatial cognition, personality changes, and linguistic difficulties. CCAS can be assessed by using the Schmahmann Syndrome Scale (which assesses fluency, phonemic fluency, category switching, verbal registration and recall, digit span [forward and backward], cube drawing and copying, similarities, go/no-go testing, and rater assessment of the patient’s affect) at the bedside for diagnostic purposes.
Article Information
Published Online: May 19, 2026. https://doi.org/10.4088/PCC.25f04134
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 5, 2025; accepted January 29, 2026.
To Cite: Miran DM, Ramirez KJ, Naughton JC, et al. Affective, behavioral, and cognitive manifestations associated with central nervous system lesions. Prim Care Companion CNS Disord 2026;28(3):25f04134.
Author Affiliations: Department of Supportive Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts (Miran); Harvard Medical School, Boston, Massachusetts (Miran, Ramirez, Stern); Department of Psychiatry, Beth Israel Deaconess Medical Center, Boston, Massachusetts (Ramirez); Department of Psychiatry, University of Rochester Medical Center, Rochester, New York (Naughton); Department of Psychiatry, Massachusetts General Hospital, Boston, Massachusetts (Stern).
Author Contributions: Dr Miran, Dr Ramirez, and Dr Naughton are co-first authors; Dr Stern is the senior author.
Corresponding Author: Damien M. Miran, MD, Department of Supportive Oncology, Dana-Farber Cancer Institute, Boston, Massachusetts ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Clinical Points
- Neuropsychiatric manifestations of brain metastases are varied, although certain symptoms can be associated with the brain region in which there is a metastasis.
- Lesions that affect certain parts of the cerebellum can interfere with an individual’s cognition and affect.
- Cerebellar cognitive affective syndrome (CCAS) is related to damage to lobules VI and VII and potentially lobule IX. Defining features include deficits in executive function, spatial cognition, personality, and linguistic function.
- The Schmahmann Syndrome Scale is a bedside tool used to evaluate individuals for CCAS.
References (20)

- Soffietti R, Franchino F, Rudà R, et al. Brain metastasis as complication of systemic cancers. In: Schiff D, Arrillaga I, Wen P, eds. Cancer Neurology in Clinical Practice. Springer International Publishing AG;2017:57–79. CrossRef
- Lamba N, Wen PY, Aizer AA. Epidemiology of brain metastases and leptomeningeal disease. Neuro-oncology. 2021;23(9):1447–1456. PubMed CrossRef
- Nayak L, Lee EQ, Wen PY. Epidemiology of brain metastases. Curr Oncol Rep. 2012;14(1):48–54. PubMed CrossRef
- Yin G, Li C, Chen H, et al. Predicting brain metastases for non-small cell lung cancer based on magnetic resonance imaging. Clin Exper Metastasis. 2017;34(2):115–124. PubMed CrossRef
- Sands JM, Daly ME, Lee EQ. Neurologic complications of lung cancer. Cancer. 2020;126(20):4455–4465. PubMed CrossRef
- Graus F, Dalmau J. Paraneoplastic neurological syndromes in the era of immune checkpoint inhibitors. Nat Rev. Clin Oncol. 2019;16(9):535–548. PubMed CrossRef
- Dietrich J, Parsons MW, Schiff D, et al. Cognitive dysfunction, mood disorders, and fatigue as complications of cancer. In: Schiif D, Arillaga I, Wen PY, eds. Cancer Neurology in Clinical Practice. Springer International Publishing AG;2018:203–219.
- Schmahmann JD, Sherman JC. The cerebellar cognitive affective syndrome. Brain. 1998;121(4):561–579. PubMed CrossRef
- Rønning C, Sundet K, Due-Tønnessen B, et al. Persistent cognitive dysfunction secondary to cerebellar injury in patients treated for posterior fossa tumors in childhood. Pediatr Neurosurg. 2005;41(1):15–21. PubMed CrossRef
- Zhao Z, Zhang C, Zhou L, et al. Immune checkpoint inhibitors and neurotoxicity. Curr Neuropharmacol. 2021;19(8):1246–1263. PubMed CrossRef
- Morris EC, Neelapu SS, Giavridis T, et al. Cytokine release syndrome and associated neurotoxicity in cancer immunotherapy. Nat Rev. Immunol. 2022;22(2):85–96. PubMed CrossRef
- Neelapu SS, Tummala S, Kebriaei P, et al. Chimeric antigen receptor T-cell therapy — assessment and management of toxicities. Nat Rev. Clin Oncol. 2018;15(1):47–62. PubMed CrossRef
- Wallesch CW, Horn A. Long-term effects of cerebellar pathology on cognitive functions. Brain Cognition. 1990;14(1):19–25. PubMed CrossRef
- Kingma A, Mooij JJ, Metzemaekers JD, et al Transient mutism and speech disorders after posterior fossa surgery in children with brain tumours. Acta Neurochir, 199. 4;131(1-2):74–79. PubMed CrossRef
- van Dongen HR, Catsman-Berrevoets CE, van Mourik M. The syndrome of ’cerebellar’ mutism and subsequent dysarthria. Neurology. 1994;44(11):2040–2046. PubMed CrossRef
- Schmahmann JD. From movement to thought: Anatomic substrates of the cerebellar contribution to cognitive processing. Hum Brain Mapp. 1996;4(3):174–198. PubMed CrossRef
- Hoche F, Guell X, Vangel MG, et al. The cerebellar cognitive affective/ Schmahmann Syndrome Scale. Brain J Neurol. 2018;141(1):248–270. PubMed CrossRef
- Schmahmann JD, Weilburg JB, Sherman JC. The neuropsychiatry of the cerebellum—Insights from the clinic. The Cerebellum. 2007;6(3):254–267. PubMed CrossRef
- Nishida Y, Hizume M, Fumimura Y, et al. Cerebellar cognitive affective syndrome improved by Ddonepezil. Intern Med. 2019;58(7):1003–1006. PubMed CrossRef
- Yap JL, Wachtel LE, Ahn ES, et al. Treatment of cerebellar cognitive affective syndrome with aripiprazole. J Pediatr Rehabil Med. 2012;5(3):233–238. PubMed CrossRef
Please sign in or purchase this PDF for $40.