Acitretin, a second-generation systemic retinoid, is used to treat chronic plaque psoriasis.1 Although generally tolerated, long-term use may disrupt hepatic metabolism, leading to hyperhomocysteinemia via inhibition of cystathionine β-synthase (CBS) or reduced folate and vitamin B12 levels.2,3 Hyperhomocysteinemia, defined as serum homocysteine >15 μmol/L, impairs remethylation and transsulfuration pathways, causing neurotoxicity through N-methyl-D-aspartate receptor agonism, oxidative stress, endothelial dysfunction, and impaired monoamine synthesis.4,5 These effects may manifest as anxiety, sensory disturbances, and cognitive decline, particularly in elderly patients.4,6 This report describes acitretin-associated hyperhomocysteinemia inducing neuropsychiatric symptoms, highlighting the need for monitoring.
Case Report
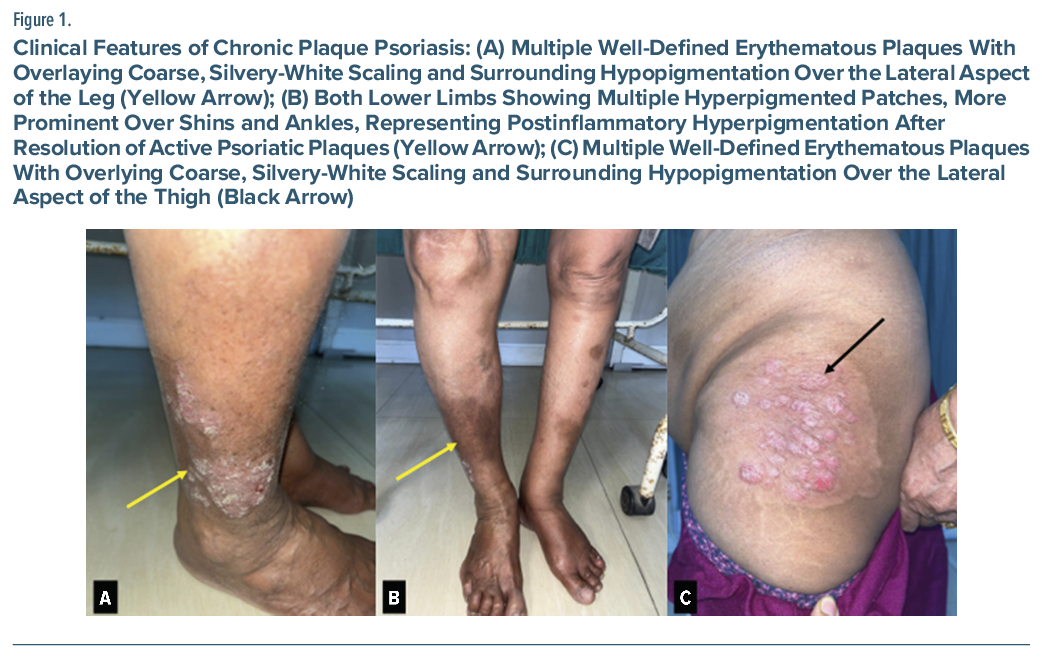
A 71-year-old woman (body mass index = 19.6 kg/m2) with chronic plaque psoriasis for 10 years presented with neuropsychiatric symptoms during acitretin therapy. Her diagnosis of psoriasis was based on clinical features, including multiple well-defined erythematous plaques with silvery-white scales symmetrically over extensor elbows, knees, lumbosacral region, and lower legs (Figure 1A, C). Plaques were indurated, nontender, with postinflammatory hyperpigmentation in healing areas (Figure 1B). Her scalp had mild diffuse scaling, nails had shallow pits without onycholysis or oil-drop sign, and oral/genital mucosa and hair were normal. Grattage test enhanced silvery scaling, candle grease sign revealed a shiny waxy surface, Auspitz sign showed pinpoint bleeding, and Koebner phenomenon was absent.
Acitretin had been initiated in October 2024 at 25 mg/10 mg on alternate days for 4–5 months, yielding marked lesion improvement, and tapered to 10 mg daily in March–April 2025 for 2 months, but a relapse in June 2025 prompted re-escalation to 25 mg/10 mg on alternate days through October 2025. Liver function and lipid values term acitretin therapy. Although acitretin is generally well tolerated, its influence on 1-carbon metabolism can lead to biochemical changes such as remained within normal limits. In October 2025, she reported a persistent cold/wet sensation over her upper back for 7 to 8 weeks, with associated apprehension, restlessness, and occasional slips in memory. Her Hindi-Montreal Cognitive Assessment7 (H-MOCA) score was 18/30.
Laboratory findings at the current presentation included hemoglobin of 12.2 g/dL (normal), platelet count of 1.10×105/µL (mild thrombocytopenia), serum vitamin B12 of 159 pg/mL (low), thyroid-stimulating hormone of 0.906 µIU/mL (normal), serum homocysteine of 50 μmol/L (elevated; reference <15), and serum ferritin of 19 ng/mL (borderline low). Neuroimaging was unremarkable. The diagnosis was acitretin-induced hyperhomocysteinemia causing neuropsychiatric manifestations, per Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, criteria for substance-induced neurocognitive disorder (minor).7
Acitretin was discontinued; intramuscular vitamin B12 (1,000 µg on alternate days ×5), folic acid 5 mg daily, and etizolam 0.25 mg twice daily were started. The dermatology consultant planned nonretinoid options for psoriasis if needed.
At the last 3-week follow-up, the patient reported improvement. Her H-MOCA8 score increased to 25/30 (38.9% relative improvement).
Discussion
This case highlights a rare but important metabolic and neuropsychiatric side effect of long-term acitretin therapy. Although acitretin is generally well tolerated, its influence on 1-carbon metabolism can lead to biochemical changes such as raised homocysteine, particularly in elderly or nutritionally deficient patients.2,3 Retinoids have been known to alter hepatic methylation reactions, potentially reducing CBS enzyme activity and indirectly affecting folate and vitamin B12 pathways.2,3 Such metabolic interference may explain the neurosensory symptoms observed in this patient, even in the absence of overt hepatic or renal dysfunction.4–6 Furthermore, the improvement in neuropsychiatric symptoms following vitamin B12 supplementation supports the possible role of hyperhomocysteinemia in these manifestations.
Most published data describe adverse effects at high doses (25–50 mg/day), but our case demonstrates that even low-dose, long-duration regimens (10–25 mg on alternate days) can produce measurable metabolic disturbances.2,3 Chronic, subclinical disruption of the homocysteine-folate-B12 axis may accumulate over time, resulting in elevated homocysteine and neuropsychiatric symptoms. This emphasizes the need for periodic monitoring of vitamin B12 and homocysteine even during maintenance therapy, especially in older patients.
Conclusion
Clinicians should monitor homocysteine, vitamin B12, and folate during prolonged retinoid therapy, especially in elderly patients, to mitigate risks. Supplementation may prevent complications without compromising psoriasis control.
Article Information
Published Online: April 14, 2026. https://doi.org/10.4088/PCC.25cr04137
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04137
Submitted: November 12, 2025; accepted January 6, 2026.
To Cite: Singh B, Sandhu MS, Alam A, et al. Neuropsychiatric manifestations of acitretin-induced hyperhomocysteinemia in a patient with chronic plaque psoriasis. Prim Care Companion CNS Disord 2026;28(2):25cr04137.
Author Affiliations: Department of DVL, Shri Guru Ram Rai Institute of Medical and Health Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India (Singh, Alam, Kumari); Department of Psychiatry, Shri Guru Ram Rai Institute of Medical and Health Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, India (Sandhu, Garg).
Corresponding Author: Shobit Garg, MD, Department of Psychiatry, Shri Guru Ram Rai Institute of Medical and Health Sciences, Shri Guru Ram Rai University, Dehradun, Uttarakhand, 248001 India ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and information, including dates, has been de-identified to protect anonymity.
References (8)

- Bozzo C, Harrison R, Purgina B. Acitretin. [Updated 2024 May 21]. In: StatPearls [Internet]. StatPearls Publishing; 2024. https://www.ncbi.nlm.nih.gov/books/NBK535174/
- Majchrzak-Wieczorek M, Szymańska M, Słowik-Rylska M, et al. The effect of acitretin on plasma homocysteine, vitamin B12 and folic acid concentrations in psoriatic patients. J Dermatolog Treat. 2016;27(1):31–35. PubMed
- Akar A, Ozgöztasi O, Uçmak D, et al. Acitretin treatment in psoriasis: a study of its effects on plasma homocysteine, vitamin B12 and folic acid. Cutan Ocul Toxicol. 2012;31(4):287–290.
- Boldyrev AA. Molecular mechanisms of homocysteine neurotoxicity. Biochem (Mosc). 2009;74(8):791–798.
- Obeid R, Herrmann W. Homocysteine and the B-vitamins in nervous system diseases. Subcell Biochem. 2012;56:295–316.
- Smith AD, Refsum H. Homocysteine, B vitamins, and cognitive impairment. Annu Rev Nutr. 2016;36:211–239. PubMed CrossRef
- American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders. 5th ed. American Psychiatric Association; 2013.
- Gupta M, Gupta V, Nagar Buckshee R, et al. Validity and reliability of Hindi translated version of Montreal Cognitive Assessment in older adults. Asian J Psychiatr. 2019;45:125–128. PubMed CrossRef
Please sign in or purchase this PDF for $40.