Huntington disease (HD) is an autosomal dominant neurodegenerative disorder caused by cytosine-adenine-guanine (CAG) trinucleotide repeats in the huntingtin (HTT) gene on chromosome 4.1 Common psychiatric manifestations include anxiety, disinhibition, and irritability.2 Psychosis is less frequent, affecting about 4.1% of patients, typically later in the course.3 Clinicians may be less familiar with phenotypically similar variants of HD that have emerged in the literature, including Huntington disease-like 2 (HDL2). HDL2 is an autosomal dominant disorder caused by CAG/cytosine-thymine-guanine repeat expansions in the junctophilin-3 gene on chromosome 16q24.2.4 Repeat length predicts age at onset but not disease severity.
HDL2 closely resembles HD, though chorea is less prominent, and visual disturbances are more common.3 As with HD, psychiatric symptoms often occur early, including depression, psychosis, and behavioral changes such as social withdrawal and irritability,2,3 which may worsen with disease progression.
HDL2 is rare, with only case reports in the literature and no prior reports on the use of electroconvulsive therapy (ECT) for refractory psychiatric symptoms. We describe a patient with genetically confirmed HDL2 and severe psychosis who improved with ECT.
Case Report
A 47-year-old African American woman with no psychiatric history presented with psychosis and disorganized behavior. She appeared thin, guarded, and minimally cooperative and exhibited paranoid and grandiose delusions.
She was started on risperidone 1 mg twice daily, titrated to 2 mg twice daily with benztropine 0.5 mg nightly, with minimal improvement. No gait abnormalities or choreiform movements were observed, though she declined a full neurological examination.
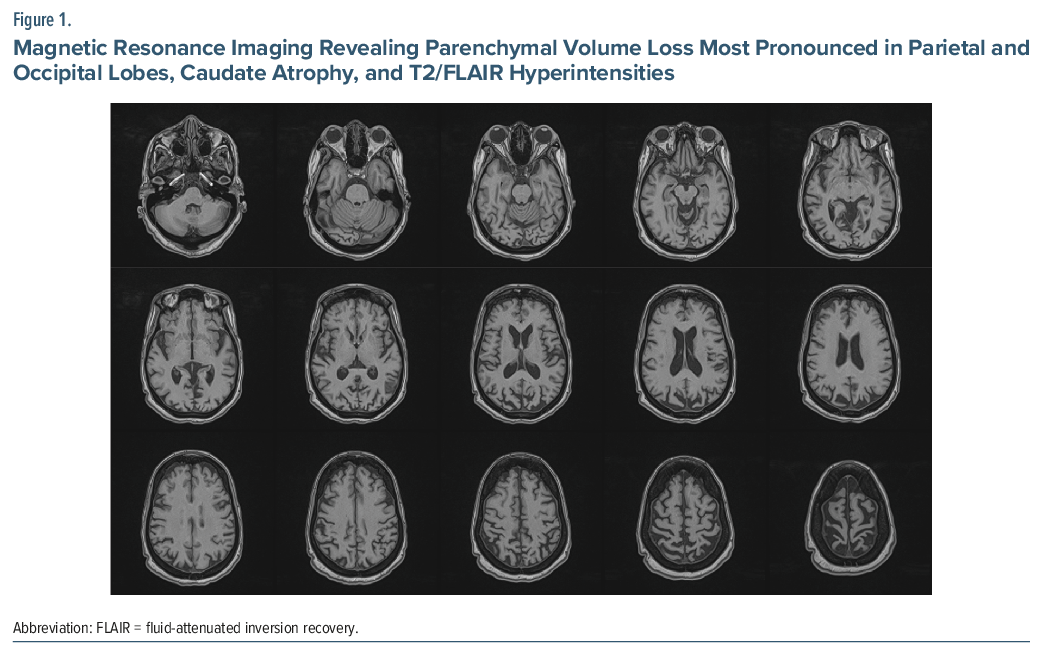
Family history revealed multiple relatives with confirmed HD. Genetic testing for HD and an extensive secondary workup (HIV, rapid plasma reagin, antinuclear antibody, N-methyl-D-aspartate antibodies, and metabolic and infectious panels) were negative. Magnetic resonance imaging (Figure 1) showed parenchymal volume loss most pronounced in parietal and occipital lobes, caudate atrophy, and T2/fluid-attenuated inversion recovery hyperintensities. The neurology department suggested HD or a related diagnosis. Further history clarified that family members had tested positive for HDL2. The patient’s mother had 44 repeats and died in 2017; siblings with 46 and 44 repeats are still living.
After 4 weeks of limited response, we discussed ECT with the family. They supported treatment as consistent with the patient’s values. She received 3 inpatient ECT sessions with good tolerance, improved interactivity, and spontaneous speech. Upon eating consistently and showing reduced paranoia, she was discharged to her daughter’s care.
She continued outpatient ECT, completing 9 treatments to date with a Thymatron System IV (bitemporal, 0.5-msec pulse, 25–35% energy). Seizures lasted 46–96 seconds (mean of 67.6 seconds).
Discussion
This patient with genetically confirmed HDL2 had refractory psychosis and functional decline but responded well to ECT. Her paranoia, agitation, and refusal to eat improved substantially, restoring self-care and quality of life.
HDL2 should be suspected in patients of African descent with HD-like features but negative genetic testing.4 Imaging parallels HD, with caudate and hemispheric degeneration; in some reports, occipital and thalamic involvement is more pronounced.5 Our patient’s occipital and caudate changes align with these findings.
Psychiatric symptoms are common in HD and HDL2, which are often resistant to medication, and antipsychotics may worsen motor symptoms. ECT, well documented in HD, has improved psychosis, agitation, and sometimes motor function.6,7 Our case suggests a similar benefit in HDL2, with attention to potential cognitive side effects.8 Importantly, improvement in psychiatric symptoms also benefits caregivers.9
Conclusion
HDL2 should be considered in patients with HD-like features but negative HTT testing. ECT appears safe and effective for refractory psychiatric symptoms in HDL2 and should be considered when standard treatments fail.
Article Information
Published Online: May 19, 2026. https://doi.org/10.4088/PCC.25cr04163
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(3):25cr04163
Submitted: December 7, 2025; accepted January 26, 2026.
To Cite: Kadan J, Doxey C, Noe G, et al. Using electroconvulsive therapy to treat psychosis associated with Huntington disease-like 2. Prim Care Companion CNS Disord 2026;28(3):25cr04163.
Author Affiliations: Wake Forest University School of Medicine, Winston-Salem, North Carolina (all authors).
Corresponding Author: Jacob Kadan, BM, MS, Wake Forest University School of Medicine, Winston-Salem, North Carolina ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and information has been de-identified to protect patient anonymity.
References (9)

- Huntington G. On chorea. George Huntington, MD. J Neuropsychiatry Clin Neurosci. 2003;15(1):109–112. PubMed CrossRef
- Margolis RL, O’Hearn E, Rosenblatt A, et al. A disorder similar to Huntington’s disease is associated with a novel CAG repeat expansion. Ann Neurol. 2001;50(6):373–380. PubMed
- Fischer CA, Licht EA, Mendez MF. The neuropsychiatric manifestations of Huntington’s disease-like 2. J Neuropsychiatry Clin Neurosci. 2012 Fall;24(4):489–92. PubMed CrossRef
- Krause A, Mitchell C, Essop F, et al. Junctophilin 3 (JPH3) expansion mutations causing Huntington disease like 2 (HDL2) are common in South African patients with African ancestry and a Huntington disease phenotype. Am J Med Genet B Neuropsychiatr Genet. 2015;168(7):573–585. PubMed CrossRef
- Anderson DG, Haagensen M, Ferreira-Correia A, et al. Emerging differences between Huntington’s disease-like 2 and Huntington’s disease: a prospective comparison of MRIs. Neuroimage Clin. 2019;21:101666. PubMed CrossRef
- Nakano T, Ono S, Yamaguchi J, et al. Modified electroconvulsive therapy for the treatment of refractory schizophrenia-like psychosis associated with Huntington’s disease. J Neurol. 2013;260(1):312–314. PubMed CrossRef
- Adrissi J, Nadkarni NA, Gausche E, et al. Electroconvulsive therapy (ECT) for refractory psychiatric symptoms in Huntington’s disease: a case series and review of the literature. J Huntingtons Dis. 2019;8(3):291–300. PubMed CrossRef
- Jensen P, Sorensen SA, Fenger K, et al. A study of psychiatric morbidity in patients with Huntington’s disease, their relatives, and controls. Admissions to psychiatric hospitals in Denmark from 1969 to 1991. Br J Psychiatry. 1993;163:790–797. PubMed CrossRef
- Kirov GG, Owen L, Ballard H, et al. Evaluation of cumulative cognitive deficits from electroconvulsive therapy. Br J Psychiatry. 2016;208(3):266–270. 2 Prim Care Companion CNS Disord 2026;28(3):25cr04163 PubMed CrossRef
Please sign in or purchase this PDF for $40.