Reversible cerebral vasoconstriction syndrome (RCVS) is a rare disorder marked by sudden, severe “thunderclap” headaches and can be accompanied by nausea, vomiting, photophobia, or transient neurologic deficits.1–4 The incidence of this condition is estimated to be 2.7 cases per million adults.2 These headaches are frequently triggered by exertion, sexual activity, or Valsalva maneuvers.4 RCVS involves transient multifocal constriction of cerebral arteries with spontaneous recovery but can still lead to ischemic stroke, subarachnoid hemorrhage, posterior reversible encephalopathy syndrome, or, rarely, death.1,3,5 Although rare, up to 80% of patients have an identifiable trigger, most often the postpartum state or exposure to vasoactive substances with adrenergic or serotonergic activity.3,6 Such agents range from cocaine and other stimulants to prescribed medications including antidepressants.1,3,7 Digital subtraction angiography remains the diagnostic gold standard, though magnetic resonance angiography and computed tomography angiography (CTA) are more commonly implemented to detect the classic “string-of-beads” arterial pattern.4,6,8 Given the widespread use of serotonergic antidepressants, heightened awareness of RCVS risk in psychiatric patients is warranted.9
Case Report
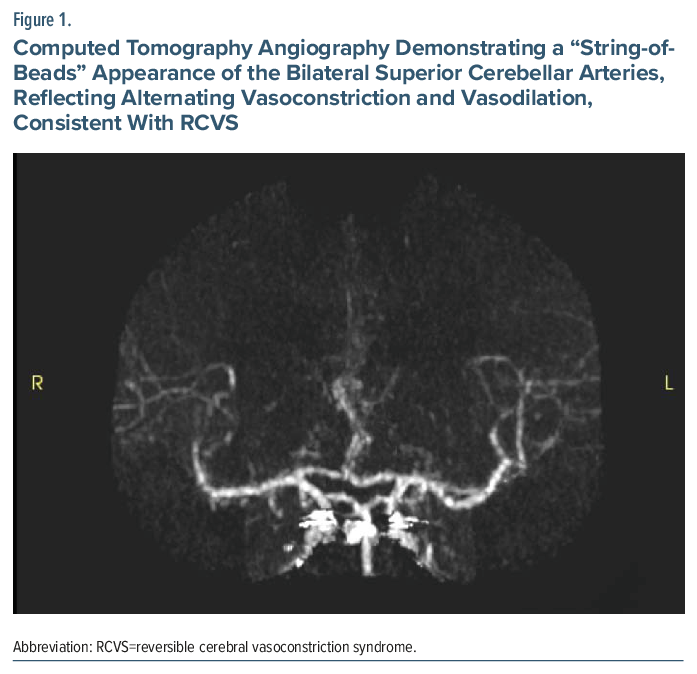
A 28-year-old man with recurrent major depressive disorder, chronic posttraumatic stress disorder, generalized anxiety disorder, migraine, and obstructive sleep apnea presented to the emergency department after an acute episode of intense hot flash, mild chest discomfort, and paresthesia of the left face, tongue, and lower extremity. He also reported a feeling of heavy pressure on his posterior head and neck. Code stroke was activated. CTA revealed diffuse partial attenuation of major intracranial arteries around the circle of Willis and within the posterior circulation, including the bilateral superior cerebellar arteries and posterior inferior cerebellar arteries, interpreted as multifocal vasospasm (Figure 1). The rest of the workup, including brain magnetic resonance imaging, routine laboratory testing, and urine toxicology, was unrevealing.
The patient was prescribed sertraline 200 mg/d and bupropion 150 mg/d for mood management. He had been stable on this regimen for years and attempted to self-discontinue, resulting in him being off these medications for about 6 weeks. Following the return of his depressive symptoms, the patient reinitiated his medications at full doses prior to hospitalization without consulting his physician. Because serotonergic agents have been implicated in RCVS, the psychiatry department was consulted, and sertraline was tapered and discontinued while bupropion was continued. No calcium-channel blocker or other vasodilator therapy was initiated given the absence of recurrent headaches or neurologic decline. The patient remained clinically stable and was discharged; on follow-up, he reported no recurring headaches.
Discussion
The pathophysiology of RCVS involves abrupt dysregulation of cerebral arterial tone resulting from sympathetic overactivity and direct serotonergic effects on vascular smooth muscle.2,6 Serotonin receptors, notably 5-HT1B/1D subtypes, mediate vasoconstriction of intracranial vessels; therefore, pharmacologic agents that increase synaptic serotonin can provoke vasospasm in susceptible individuals.7 Selective serotonin reuptake inhibitors (SSRIs) are the most frequently reported antidepressant class associated with RCVS, with case reports implicating fluoxetine, sertraline, paroxetine, and citalopram.1,3 Polypharmacy and concurrent sympathetic stimuli may further elevate risk. Importantly, while thunderclap headache is the hallmark symptom, “headache-poor” presentations with focal deficits or sensory symptoms without severe headache are described and may delay diagnosis.3
Management centers on prompt identification and removal of offending agents, symptomatic support, and monitoring for complications. Calcium-channel blockers (eg, nimodipine) are commonly employed, though randomized trial data are lacking. Magnesium and blood pressure optimization are other treatment options.2,6,8 Early discontinuation of the suspected trigger often coincides with clinical improvement and angiographic reversibility, emphasizing the need for rapid medication review in affected patients. This case, in which our patient experienced a rare syndrome following reinitiation of his SSRI at a high dose despite previous tolerability, reinforces the importance of monitoring for acute neurologic symptoms in patients treated with high-dose SSRIs.
Article Information
Published Online: April 23, 2026. https://doi.org/10.4088/PCC.25cr04151
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04151
Submitted: November 26, 2025; accepted December 29, 2025.
To Cite: Savoldy M, Bojkovic K, Klippel C, et al. Psychotropic-induced reversible cerebral vasoconstriction syndrome in a young man taking sertraline. Prim Care Companion CNS Disord 2026;28(2):25cr04151.
Author Affiliations: Department of Psychiatry and Behavioral Neurosciences, University of South Florida College of Medicine, Tampa, Florida (Savoldy); University of South Florida College of Medicine, Tampa, Florida (Bojkovic, Klippel, Fusick); Mental Health and Behavioral Sciences Service, James A. Haley Veterans Hospital, Tampa, Florida (Klippel, Fusick)
Corresponding Authors: Adam J. Fusick, MD, Mental Health and Behavioral Sciences Service, James A. Haley Veterans Hospital, 13000 Bruce B. Downs Blvd #116A, Tampa, Florida 33612 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and information has been de-identified to protect patient anonymity.
References (9)

- Manning T, Bartow C, Dunlap M, et al. Reversible cerebral vasoconstriction syndrome associated with fluoxetine. J Acad Consult Liaison Psychiatry. 2021;62(6):634–644. PubMed CrossRef
- Postolowski M, Shakil O, Ramachandran L, et al. Reversible cerebral vasoconstriction syndrome secondary to escitalopram. Clin Med Res. 2024;22(4):222–226. PubMed CrossRef
- Ribas MZ, Paticcié GF, de Medeiros SDP, et al. Reversible cerebral vasoconstriction syndrome: literature review. Egypt J Neurol Psychiatr Neurosurg. 2023;59(1):5. PubMed CrossRef
- Arnold M. Headache Classification Committee of the International Headache Society (IHS) the International Classification of Headache Disorders. Cephalalgia. 2018;38(1):1–211.
- Valencia-Mendoza M, Ramírez-Rodríguez N, Vargas-Avila N, et al. Fatal reversible cerebral vasoconstriction syndrome: a systematic review of case series and case reports. J Clin Neurosci. 2019;70:183–188. PubMed CrossRef
- Ducros A. Reversible cerebral vasoconstriction syndrome. Lancet Neurol. 2012;11(10):906–917. PubMed CrossRef
- Vanhoutte PM. Serotonin and the vascular wall. Int J Cardiol. February 1987;14(2):189–203. PubMed CrossRef
- Miller TR, Shivashankar R, Mossa-Basha M, et al. Reversible cerebral vasoconstriction syndrome, Part 1: epidemiology, pathogenesis, and clinical course. AJNR Am J Neuroradiol. 2015;36(8):1392–1399. PubMed CrossRef
- Gutlapalli SD, Chaudhuri D, Khan KI, et al. Statins and antidepressants: a comprehensive review and clinical outlook of the risks and benefits of Co-prescription (2022). Cureus. 2022;14(12):e32331. PubMed CrossRef
Please sign in or purchase this PDF for $40.




