Abstract
Objective: Adult attention-deficit/hyperactivity disorder (ADHD) is commonly associated with comorbidities, including depression and anxiety; however, most ADHD treatment studies exclude people with these conditions. This phase 4, open-label, decentralized clinical trial (conducted March 25, 2024–December 11, 2024) evaluated viloxazine ER (extended-release capsules, an FDA-approved nonstimulant medication for ADHD) in adults with ADHD (based on DSM-5-TR) and comorbid depression and/or anxiety symptoms.
Methods: Participants received viloxazine ER (200–600 mg/d) for 14 weeks added to existing medications (including stimulant, antidepressant, or anxiolytic medications). Efficacy and safety measures (assessed via televisit, mobile phone app, and home monitoring devices) included clinician-and patient-reported scales evaluating ADHD, depression, and anxiety symptoms, treatment-emergent adverse events, blood pressure, pulse rate, weight, and suicidality assessment. The primary end point was change from baseline in Adult ADHD Investigator Symptom Rating Scale (AISRS) total score.
Results: Among participants receiving viloxazine ER (n=161; mean age, 39.4 years; female, 75.8%), almost all (99.4%) had substantial depression and anxiety symptoms. AISRS total score was significantly reduced (improved) from baseline (mean [SD], 37.5 [6.53]; n=150) at week 14/end of study (EOS) (mean [SD] change, −17.3 [11.34]; P<.0001); similar results were observed for patient-reported ADHD symptoms. Depression and anxiety rating scales were significantly improved from baseline to week 14/EOS (all P<.0001). Safety outcomes were consistent with previous viloxazine ER studies; 24 participants (14.9%) had adverse events leading to study discontinuation.
Conclusions: Viloxazine ER was well tolerated and associated with improvements in ADHD, depression, and anxiety symptoms in this real-world study of adults with ADHD and comorbid symptoms.
Trial Registration: ClinicalTrials.gov identifier: NCT06185985
J Clin Psychiatry 2026;87(2):25m16234
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Attention-deficit/hyperactivity disorder (ADHD) often overlaps with other conditions, including depression and anxiety, that complicate diagnosis and treatment.1 Over half of adults with ADHD also have a co-occurring mood or anxiety disorder.2,3 The presence of psychiatric comorbidities increases morbidity and mortality risk in people with ADHD,4–6 with the risk incrementally increasing with comorbidity number.4 Comorbidities can also add to long-term functional impairment for people living with ADHD.3,5–7 Therefore, it is common for individuals with ADHD to receive concomitant treatments for ADHD, depression, anxiety, sleep disorders, and other conditions.8
Viloxazine ER (extended-release capsules; Qelbree®) is a US Food and Drug Administration (FDA)-approved nonstimulant medication for pediatric and adult ADHD.9 In the US, viloxazine ER has only been evaluated for ADHD to date. However, studies from the 1970s demonstrated that viloxazine has antidepressant effects,10 and viloxazine was approved and used in Europe as an immediate-release product for depression for approximately 30 years before being discontinued for commercial reasons unrelated to efficacy or safety.11
Recent preclinical studies have confirmed that viloxazine has a multimodal norepinephrine and serotonergic pharmacodynamic profile in the therapeutically relevant dosage range used to treat ADHD, which could contribute to symptomatic response. While viloxazine and atomoxetine both have action as selective norepinephrine transporter inhibitors, viloxazine also modulates specific serotonin (5-HT) receptors, displaying partial agonist activity at the 5-HT2C receptor and antagonist activity at 5-HT2B and 5-HT7 receptors, which may explain viloxazine ER’s observed ability to increase serotonin in the prefrontal cortex in animal models.9,12–14 Whether these serotonin receptor effects contribute to the clinical response of viloxazine ER in ADHD is unknown and warrants further investigation.
Clinical trials for ADHD treatments, including viloxazine ER,15 routinely exclude participants with psychiatric comorbidities. These exclusions, while perhaps desirable for achieving regulatory approval, can limit the capacity to measure effects on mood and anxiety symptoms in phase 3 trials (due to floor effects) and restrict generalizability of findings from a clinical trial to real-world populations. Therefore, we designed the phase 4 study reported here to evaluate viloxazine ER treatment in adults with ADHD who also experience prominent depression or anxiety symptoms. The trial was designed to represent real-world viloxazine ER use, with eligibility, dosing, and concomitant medication restrictions guided by the current FDA-approved prescribing information. The trial design was fully decentralized to reduce entry barriers. Participants were recruited online, and data were collected via a mobile app and televisits with clinical raters or psychiatric nurse practitioners trained in the rating scales employed in the trial. Here, we present primary efficacy and safety results from this trial.
METHODS
Study Design, Participants, and Treatment
This phase 4, open-label, flexible-dose, decentralized study (NCT06185985) evaluated the efficacy and safety of viloxazine ER in adults with ADHD and comorbid depression and/or anxiety symptoms. Eligibility criteria were designed to reflect real-world viloxazine ER use. Prospective participants were recruited using digital tools; participation was open to adults (aged ≥18 years) who owned a functioning smartphone, had internet access, and were willing to download and use the study app. Eligible participants had a primary diagnosis of ADHD based on the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition, Text Revision, as confirmed by the Mini-International Neuropsychiatric Interview for ADHD Studies (MINI-AS), an Adult ADHD Investigator Symptom Rating Scale (AISRS16) total score ≥24, a Clinical Global Impression of Severity (CGI-S) score ≥3, and a Montgomery-Asberg Depression Rating Scale (MADRS17) total score >22 and/or a Hamilton Anxiety Rating Scale (HAM-A18) total score >22. During the screening televisit, trained raters conducted the MINI-AS, AISRS, and CGI-S evaluations and depression and anxiety symptom ratings (using the Structured Interview Guide for the MADRS [SIGMA] and Structured Interview Guide for the HAM-A [SIGH-A], respectively). The use of stimulant medications for ADHD and medications for other medical or psychiatric conditions, including depression or anxiety, was allowed. Additional details are provided in the Supplementary Methods.
The study comprised a 4-week screening period, 14-week treatment period, and 1-week safety follow-up period (Figure 1A). The study was fully decentralized; clinician-reported outcomes (CROs) and safety were assessed during televisits conducted by qualified raters or assessors who were trained on the evaluated scales, and participants provided patient-reported outcome (PRO) data through the study mobile app. During the treatment period, participants were instructed to take viloxazine ER 200 mg once daily in the morning during week 1 and 400 mg once daily in the morning during week 2 onward until the next contact with the study investigator. Televisits were conducted at weeks 4, 9, and 14 of treatment, and a safety follow-up televisit was conducted 1 week after the last viloxazine ER dose.

The study was approved by an institutional review board; followed guidance of US regulatory bodies, Good Clinical Practice regulations, and standards set by the International Conference on Harmonisation; and was conducted in accordance with the Declaration of Helsinki. All participants provided informed consent.
Efficacy Assessments
The primary end point was change from baseline in AISRS total score. Secondary clinician-reported efficacy end points included change from baseline in AISRS subscale (inattention and hyperactivity/impulsivity) scores, CGI-S score,19 MADRS total score, and HAM-A total score. Clinical Global Impression of Change (CGI-C) score was also assessed. Secondary PRO efficacy end points included change from baseline in Adult ADHD Self-Report Scale version 1.1 Symptoms Checklist (ASRSv1.1-SC) total and subscale (inattention and hyperactivity/impulsivity) scores20; Patient Health Questionnaire-8 item (PHQ-8) total score21; General Anxiety Disorder 7-item scale (GAD-7) total score22; Behavioral Rating Inventory of Executive Function–Adult Version (BRIEF-A23) Global Executive Composite (GEC), Behavioral Regulation Index (BRI), and Metacognition Index (MI) scores (converted to T-scores; consistent with previous viloxazine ER studies15,24); Work Productivity and Activity Impairment: Specific Health Problem Questionnaire (WPAI:SHP)25; and Pittsburgh Sleep Quality Index (PSQI) global score.26 Post hoc efficacy assessments included the proportion of participants achieving ≥30% or ≥50% reduction from baseline in AISRS total score (thresholds considered clinically meaningful improvements; consistent with those used in a phase 3 study of viloxazine ER in adults15) or clinically meaningful responses or published remission criteria according to MADRS, PHQ-8, HAM-A, or GAD-7 total scores.22,27,28
Safety Assessments
Safety assessments included the incidence of treatment-emergent adverse events (TEAEs), including investigator-assessed TEAE severity, seriousness, relationship to study medication, and whether TEAEs led to discontinuation. Additional safety assessments included the absolute values and change from baseline for systolic and diastolic blood pressure (SBP/DBP), pulse rate, and body weight, and presence of suicidal ideation and behavior (assessed at all televisits using the Columbia-Suicide Severity Rating Scale [C-SSRS]). Post hoc safety assessments included incidence of TEAEs by stimulant use.
Statistical Methods
Data were summarized descriptively. Nominal P values and 95% CIs were calculated for primary and secondary end points using t test. Week 14/end of study (EOS) analyses were based on assessments assigned to the nominal week 14 visit. Early termination visits were mapped to the next scheduled analysis visit according to the study schedule. Participants who were lost to follow-up or did not complete an early termination visit were excluded.
RESULTS
Participants
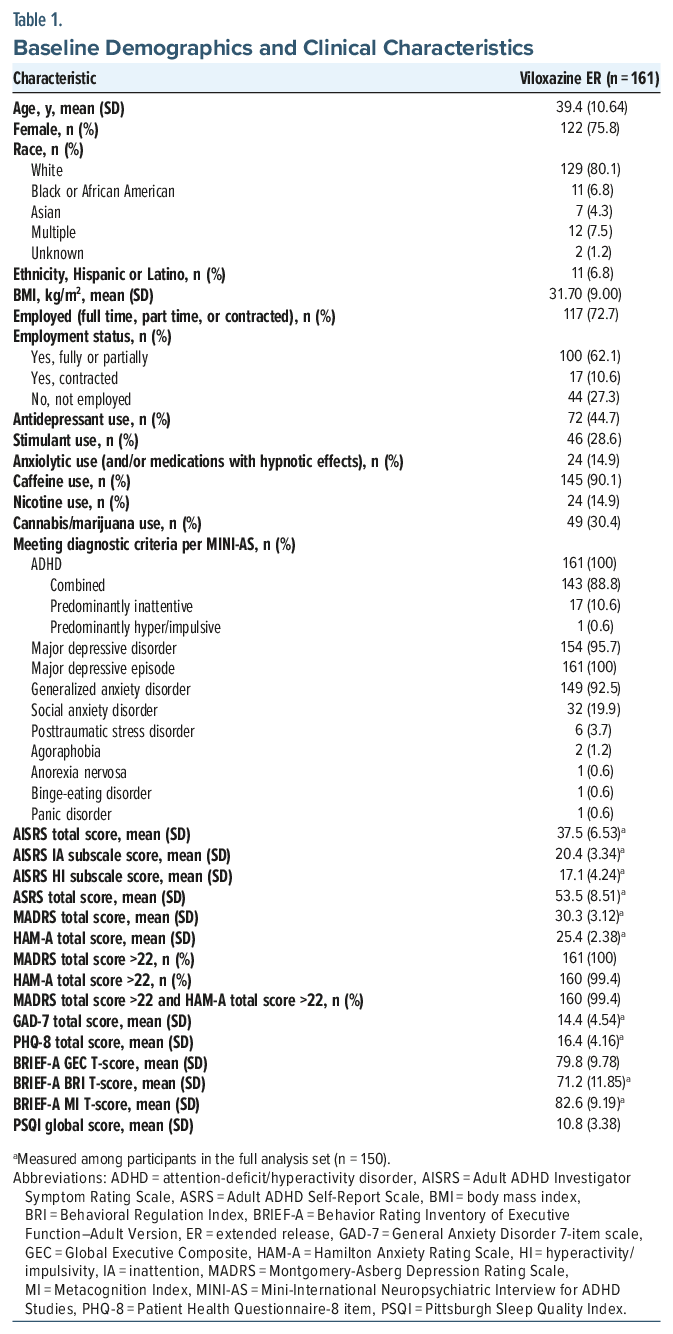
Of 1204 potential participants who provided informed consent, 662 were unable to be contacted or scheduled for a screening visit, 381 were not enrolled (primarily due to not meeting eligibility criteria, expired screening window, or withdrawn consent), and 161 received viloxazine ER treatment (Figure 1B). Of the 161 treated participants, 104 (64.6%) completed the study. Among the 161 enrolled participants (Table 1; Supplementary Table 1), most were female (75.8%), and the mean (SD) age was 39.4 (10.64) years. Mean baseline AISRS, MADRS, and HAM-A scores were consistent with moderate-to-severe ADHD, depression, and anxiety symptoms, respectively. All participants had substantial depression symptoms at baseline (MADRS >22), and almost all (99.4%) had substantial anxiety symptoms (HAM-A >22). Viloxazine ER dose distribution is shown in Supplementary Table 2. During the study, 28.6% of participants took stimulants, 44.7% took antidepressants, and 14.9% took anxiolytic and/or hypnotic medications (Supplementary Table 3).
Efficacy
Participants in the full analysis set (n = 150) showed clinically significantly reduced clinician- and patient-reported ADHD symptom scores at all study visits; at week 14/EOS, mean (SD) change from baseline was −17.3 (11.34) for AISRS total score (P < .0001; Figure 2A) and −28.4 (14.89) for ASRSv1.1-SC total score (P < .0001; Figure 2B), representing reductions from baseline of −45.3% (27.31%) and −50.9% (24.88%), respectively. The proportion of participants achieving ≥30% and ≥50% reduction in AISRS total score at week 14/EOS was 71.8% and 45.6%, respectively (Supplementary Figure 1). AISRS and ASRS inattention and hyperactivity/impulsivity subscale scores were also significantly reduced at all study visits (all P < .0001; Table 2). Substantial improvements in ADHD severity were also demonstrated by over a 1-category change in CGI-S score from baseline to week 14/EOS (mean [SD] of −1.4 [1.06]) and a mean (SD) week 14/EOS CGI-C score of 2.3 (0.97), with 63.1% of participants rated as “very much improved” or “much improved” per the CGI-C (Table 2; Supplementary Table 4).
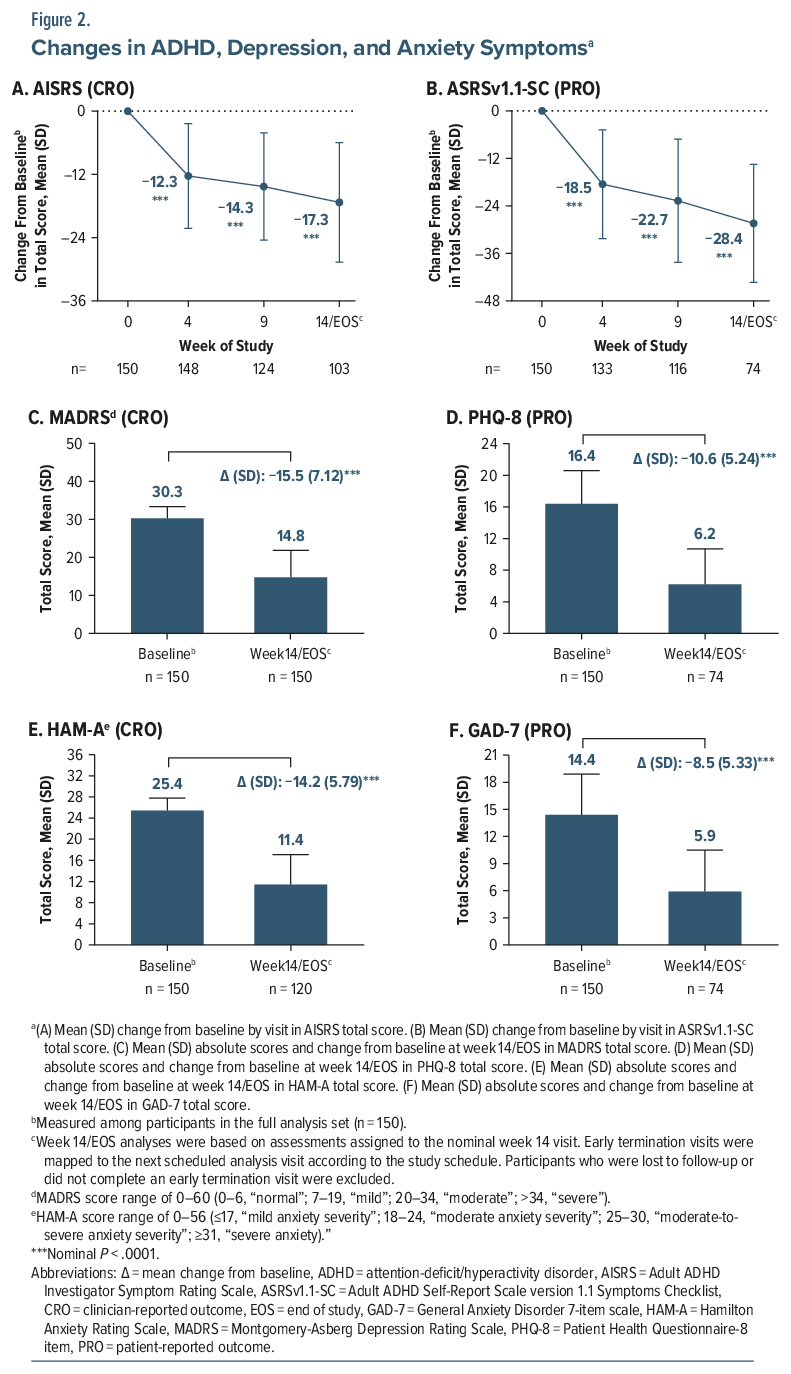
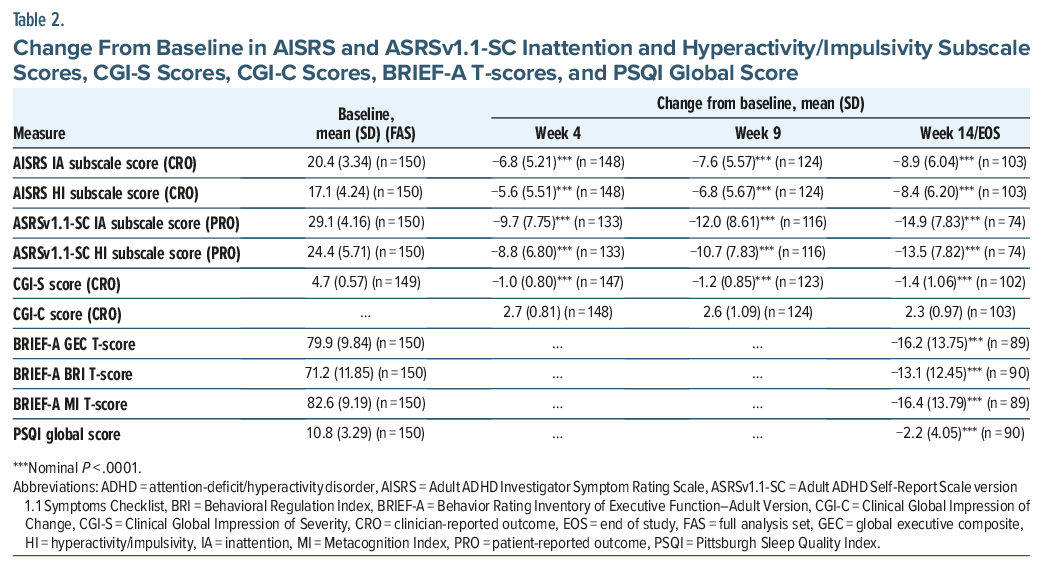
Clinician- and patient-reported depression and anxiety scores were nominally significantly reduced at all study visits (all P <.0001). At week 14/EOS, mean (SD) change from baseline in MADRS total score was −15.5 (7.12; Figure 2C) and in PHQ-8 total score was −10.6 (5.24; Figure 2D). The mean (SD) change from baseline to week 14/EOS in HAM-A total score was −14.2 (5.79; Figure 2E) and in GAD-7 total score was −8.5 (5.33; Figure 2F). For MADRS, PHQ-8, HAM-A, and GAD-7, ≥50% reduction in total score from baseline at week 14/EOS was achieved by 57.5%, 78.4%, 70.8%, and 67.6% of participants, respectively (Supplementary Figure 2A), and symptom remission was achieved by 28.3%, 48.6%, 24.2%, and 43.2% (Supplementary Figure 2B). Executive functioning and sleep measures showed significant mean reductions from baseline in BRIEF-A GEC, BRI, and MI T-scores and PSQI global scores following viloxazine ER treatment (Table 2). Work productivity impairment was significantly improved at week 14/EOS (mean [SD] change from baseline in WPAI:SHP percentages: −5.89 [20.170; P<.05] for absenteeism, −23.08 [26.072; P<.0001] for presenteeism, −36.06 [24.230; P<.0001] for regular activity, and −22.32 [26.915; P<.0001] for work productivity).
Safety
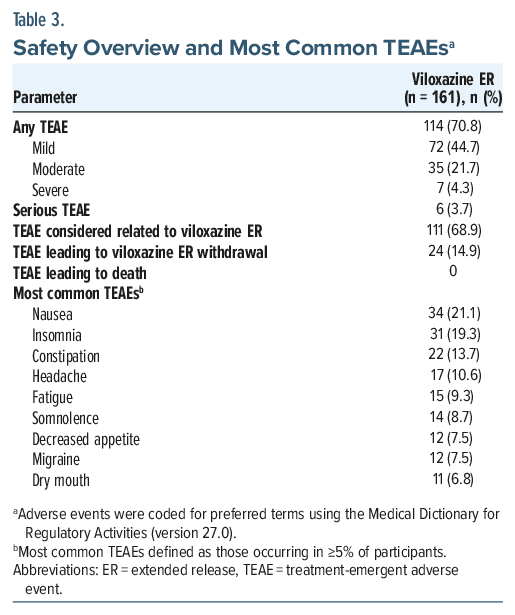
Viloxazine ER was generally well tolerated. TEAEs were experienced by 70.8% of participants; most were mild to moderate in severity (Table 3). The most common adverse events (≥5% of participants) were nausea, insomnia, constipation, headache, fatigue, somnolence, decreased appetite, migraine, and dry mouth. For 24 participants (14.9%), TEAEs led to viloxazine ER discontinuation; TEAEs leading to discontinuation of study drug in ≥3 participants included insomnia (n=8), nausea (n =5), decreased appetite (n=4), migraine (n=4), somnolence (n= 4), dizziness (n=3), and suicidal ideation (n =3; 2 considered serious, moderate in severity, and related to treatment; both reported on day 3 of study treatment). Six participants (3.7%) experienced serious TEAEs, including the 2 participants with suicidal ideation described above and 1 participant each with migraine (day 65, considered severe and possibly related to treatment, participant remained in the study), sensation of foreign body (reported term “lump in throat”; day 28, considered moderate and related to treatment, led to treatment discontinuation), and Addison disease (day 11, considered severe and unrelated to treatment, participant remained in the study). There was also 1 participant with serious adverse events of hepatic enzymes increased (day 38) and cyclic vomiting syndrome (day 64). The event of hepatic enzymes increase was considered severe and possibly related to treatment due to possible temporal association with viloxazine ER, and led to treatment discontinuation. The event of cyclic vomiting syndrome occurred 23 days after the participant discontinued study medication and was likely due to underlying gastrointestinal issues; the event was considered severe and not related to treatment. This participant also experienced TEAEs of blood cholesterol increased, thyrotoxicosis, gallbladder disease, and biliary tract disease and was taking rosuvastatin for the TEAE of blood cholesterol increased and tirzepatide for a medical history of type 2 diabetes mellitus. Viloxazine ER treatment was generally well tolerated among both participants who were or were not receiving stimulants (Supplementary Table 5). The mean (SD) number of baseline concomitant medications was higher among patients with vs without treatment-related TEAEs that were severe, serious, or led to withdrawal (3.4 [2.61], n=28 vs 2.3 [2.50], n=133, respectively).
There were modest increases in mean SBP, DBP, and pulse rate at all visits and a mean decrease in body weight at all visits (Supplementary Table 6). Overall at week 14/EOS, 20.0% and 13.3% of participants had a >15 mm Hg increase in SBP or DBP, respectively, and 10.2% had a >20 beats per minute increase in pulse rate; however, these were seldom considered TEAEs (heart rate increased, n=3 [1.9%]; hypertension, n=2 [1.2%]; palpitations, n=1 [0.6%]; blood pressure increased, n=1 [0.6%]). Five participants (3.1%) reported TEAEs of suicidal ideation (of these, 3 withdrew from the trial due to these TEAEs); suicidal ideation resolved in all cases. The proportion of participants reporting suicidal ideation on the C-SSRS during the treatment period was 5.3% (Supplementary Table 7). No suicidal behavior was reported on C-SSRS (nor as an adverse event) during viloxazine ER treatment. One patient (0.6%) reported suicidal behavior in the 6-month period before screening.
DISCUSSION
Adults with ADHD and comorbid depression and anxiety symptoms experienced substantial improvement in all 3 conditions while taking viloxazine ER treatment (alone or added to existing treatments) in this decentralized, phase 4, open-label trial (Supplementary Figure 3). Efficacy and safety results were consistent with previous phase 3 studies of viloxazine ER in adults with ADHD,15,24 and improvements in depression symptoms aligned with the past use of immediate-release viloxazine as an antidepressant in Europe.11 Measures of executive function and work productivity also improved with viloxazine ER treatment. These findings suggest that the established efficacy of viloxazine ER may extend to adults with ADHD and comorbid depression and/or anxiety symptoms, who typically represent over half of people with ADHD.2,3
Though often exclusively considered a selective norepinephrine reuptake inhibitor, early and contemporaneous pharmacology studies consistently showed that viloxazine also affects 5-HT neurotransmission.10,12–14,29–32 In drug discovery efforts, the 5-HT2B and 5-HT2C receptors are considered therapeutic targets for mood regulation and reduction of impulsivity, anxiety, and weight,33–38 and 5-HT7 antagonism has been identified as a therapeutic target to improve cognition, sleep regulation, and mood regulation.39–42 Viloxazine has previously been shown to be effective for treating depression11; whether effects on depression symptoms in this study are direct or secondary to ADHD improvement is unknown and requires evaluation in a controlled study.
Despite the high prevalence of comorbid psychiatric conditions in ADHD, including individuals with comorbid disorders (eg, anxiety, depression) in clinical studies of ADHD pharmacotherapies is uncommon. This study is the first trial of viloxazine ER in adults with ADHD to include participants with comorbid depression and/or anxiety and allow concomitant medication use for these conditions. This study had a higher proportion of female participants and higher mean baseline body weight and HAM-A scores compared with a previous adult phase 3 study population; participants in the current study also had a higher degree of executive dysfunction (according to baseline BRIEF-A T-scores) than those in the adult phase 3 trial.15 Results from the current study provide important insights into the utility of viloxazine ER treatment for people with ADHD and comorbid conditions, which comprise a large proportion of the real-world ADHD population.
Simultaneous treatment of ADHD and depression and/or anxiety symptoms can be challenging, partly due to safety concerns about combining medications.3 In a recent study evaluating stimulant use combined with other psychiatric medications, approximately half of people receiving stimulants also used antidepressants and one-third used anxiolytics, sedatives, and/or hypnotics,8 but the safety (and effectiveness) of such treatment combinations is not well studied.8 Polypharmacy can increase the risk of drug-drug interactions and TEAEs, but excluding potentially beneficial medications may also create safety risks43; whether medications like viloxazine ER could reduce co-occurring symptoms and allow reducing other medications warrants further study. Further analysis of safety outcomes is needed to uncover whether TEAEs in the current study were influenced by concomitant medication patterns (eg, medication class, duration) and/or other factors, including medical comorbidities or cannabis use. Still, preliminary safety findings from the current study are encouraging and suggest viloxazine ER can be used with other psychiatric medications with careful monitoring.
The decentralized nature of the study is a unique feature for ADHD clinical trials. This approach is encouraged by the FDA to facilitate including participants with baseline characteristics and psychiatric history that represent the real-world ADHD population.44,45 Although decentralized trials may be limited by challenges, such as ensuring validity of patient-reported data, they can also reduce participant burden and reach participants who cannot travel to a research center (due to geographical/logistical restrictions or impaired executive function).44,45 By using a decentralized design, the current study helps provide representation of viloxazine ER treatment effects in real-world populations of people with ADHD.
Strengths of this study include the real-world nature and representation of people with comorbid depression and/or anxiety symptoms (who are typically excluded from other ADHD clinical trials), its decentralized nature, and the use and high level of correlation between CROs and PROs. Limitations of the study include the open-label design (which may introduce bias and potential overestimation of treatment effects), absence of a comparator group, and lack of long-term follow-up. These analyses were conducted to descriptively characterize changes over time in an open-label, single-arm study, not to support formal confirmatory inference; no multiplicity adjustments were applied, and statistical findings across visits should be interpreted descriptively. The study was not designed to evaluate whether improvements in depression/anxiety symptoms were a direct effect of viloxazine ER or a secondary effect of ADHD symptom improvement. Concomitant medication changes or their impact on efficacy and safety have not yet been evaluated. Other limitations may include challenges inherent in a decentralized design, such as potential difficulty in consistently obtaining PROs without an in-person clinic visit, self-selection bias (considering that participants were recruited online and participated voluntarily), and inability to include individuals without online access or smartphones. The study population was mostly White and female, which could influence generalizability of the findings.
In conclusion, adults with ADHD and mood symptoms who received viloxazine ER (alone or added to existing treatments) experienced substantial improvements in ADHD, depression, and anxiety symptoms with acceptable safety and tolerability. These findings support the use of viloxazine ER to treat people with ADHD and comorbid depression and/or anxiety symptoms.
Article Information
Published Online: May 27, 2026. https://doi.org/10.4088/JCP.25m16234
© 2026 Physicians Postgraduate Press, Inc.
Submitted: November 19, 2025; accepted April 7, 2026.
To Cite: Adler LA, Lieberman VR, Brijbasi L, et al. Viloxazine extended release in adults with attention-deficit/hyperactivity disorder and depression and/or anxiety symptoms: results from a decentralized, open-label, phase 4 trial. J Clin Psychiatry. 2026; 2026;87(2):25m16234.
Author Affiliations: Department of Psychiatry, New York University Grossman School of Medicine, New York, New York (Adler); Supernus Pharmaceuticals, Inc., Rockville, Maryland (Lieberman, Brijbasi, Yarullina, Li, Earnest, Rubin); Department of Psychiatry, Washington University School of Medicine, St Louis, Missouri (Mattingly); Midwest Research Group, St Charles, Missouri (Mattingly); St Charles Psychiatric Associates, St Charles, Missouri (Mattingly).
Corresponding Author: Jonathan Rubin, MD, MBA, Supernus Pharmaceuticals, Inc., 9715 Key West Avenue, Rockville, MD 20850 ([email protected]).
Author Contributions: Conceptualization: Adler (equal), Mattingly (supporting),
Earnest (supporting), Rubin (equal); methodology: Adler (equal), Lieberman (equal), Brijbasi (equal), Rubin (equal); writing–original draft: all authors (equal); writing–reviewing and editing: all authors (equal); project administration: Lieberman (equal), Brijbasi (equal); validation: Lieberman (equal), Yarullina (equal), Li (equal); formal analysis: Li (lead); supervision: Rubin (lead).
Relevant Financial Relationships: Dr Adler has received grant/research funding from Collegium, Corium, and Otsuka and has served as a consultant for MLB, Neurocentria, NFL, Otsuka, Shire/Takeda, Signant, and Supernus. He has also received royalty payments (as an inventor) from New York University for licensing of adult ADHD scales and training materials since 2004. Ms Lieberman, Mr Brijbasi, Dr Yarullina, Dr Li, Dr Earnest, and Dr Rubin are full-time employees of Supernus Pharmaceuticals, Inc. and may hold Supernus stock or stock options. Dr Mattingly has served as a consultant for and/or received speaker fees from AbbVie, Alkermes, Axsome, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Corium, Eisai, Intra-Cellular, Ironshore, Janssen, Lundbeck, Neurocrine, Noven, Otsuka, Redax, Roche, Sage, Sirona, Sunovion, Supernus, Takeda, Teva, and Tris Pharma. He has also conducted research for AbbVie, Akili, Alkermes, Axsome, Biogen, Boehringer Ingelheim, Bristol Myers Squibb, Compass, Emalex, Idorsia, Janssen, Karuna, Lumos Labs, Medgenics, Neurocrine, NLS-1 Pharma AG, Otsuka, Redax, Relmada, Roche, Sage, Sirtsei, Sunovion, Supernus, Takeda, and Teva.
Funding/Support: Financial support for this study was provided by Supernus Pharmaceuticals, Inc. (Rockville, Maryland).
Role of the Sponsor: This study was supported by Supernus Pharmaceuticals, Inc. Supernus had the opportunity to review the manuscript for factual accuracy; the authors maintained full control of the manuscript and determined the final content.
Previous Presentation: Portions of these results were presented in a poster at the American Psychiatric Association Annual Meeting; May 17–21, 2025; Los Angeles, California, and an oral presentation at the 2025 American Professional Society of ADHD and Related Disorders Annual Conference; January 16–19, 2025; San Diego, California.
Acknowledgment: The authors thank Lauro Amezcua-Patino, MD, FAPA, for serving as an investigator on the study; Joseph T. Hull, PhD, for significant contributions to the development of the study design and protocol, study initiation, oversight of clinical trial management, review of study data, and production of the final study report; Andrea Formella, PharmD, for editorial support and coordination of post hoc analyses; and Mary Lin, PhD for editorial and graphics support. Medical writing support, funded by Supernus, was provided by Callie A. S. Corsa, PhD, ISMPP CMPPTM, of JB Ashtin, who developed the first draft based on an author-approved outline and assisted in implementing author revisions. JB Ashtin adheres to Good Publication Practice Guidelines and International Committee of Medical Journal Editors recommendations.
Data Sharing Statement: Data will be made available upon reasonable request.
Supplementary Material: Available at Psychiatrist.com.
Clinical Points
- Over half of adults with attention-deficit/hyperactivity disorder (ADHD) also experience depression and/or anxiety symptoms; however, patients with comorbid depression and/or anxiety are routinely excluded from clinical trials in ADHD.
- This phase 4, open-label, decentralized study evaluated the efficacy and safety of viloxazine extended-release (ER) in adults with ADHD and comorbid depression and/or anxiety symptoms.
- Participants treated with viloxazine ER (alone or added to concomitant medications for other psychiatric symptoms) experienced improved symptoms of ADHD, depression, and anxiety with acceptable safety and tolerability.
References (45)

- Mattingly G, Childress A. Clinical implications of attention-deficit/hyperactivity disorder in adults: what new data on diagnostic trends, treatment barriers, and telehealth utilization tell us. J Clin Psychiatry. 2024;85(4):24com15592. PubMed CrossRef
- Pehlivanidis A, Papanikolaou K, Mantas V, et al. Lifetime co-occurring psychiatric disorders in newly diagnosed adults with attention deficit hyperactivity disorder (ADHD) or/and autism spectrum disorder (ASD). BMC Psychiatry. 2020;20(1):423. PubMed CrossRef
- Mattingly GW, Wilson J, Ugarte L, et al. Individualization of attention-deficit/ hyperactivity disorder treatment: pharmacotherapy considerations by age and co-occurring conditions. CNS Spectr. 2021;26(3):202–221. PubMed CrossRef
- Sun S, Kuja-Halkola R, Faraone SV, et al. Association of psychiatric comorbidity with the risk of premature death among children and adults with attention-deficit/hyperactivity disorder. JAMA Psychiatry. 2019;76(11):1141–1149. PubMed CrossRef
- Kosheleff AR, Mason O, Jain R, et al. Functional impairments associated with ADHD in adulthood and the impact of pharmacological treatment. J Atten Disord. 2023;27(7):669–697. PubMed CrossRef
- National Academies of Sciences, Engineering, and Medicine. Adult attention-deficit/hyperactivity disorder: diagnosis, treatment, and implications for drug development: proceedings of a workshop. The National Academies Press; 2024.
- Childress A. ADHD in adults. 2024. https://www.nationalacademies.org/documents/embed/link/LF2255DA3DD1C41C0A42D3BEF0989ACAECE3053A6A9B/file/D15C556D5C9A165A6D3DE4A1B93A7943932A29C2ECCD?noSaveAs=1. Accessed May 7, 2025.
- Moore TJ, Wirtz PW, Curran JN, et al. Medical use and combination drug therapy among US adult users of central nervous system stimulants: a cross-sectional analysis. BMJ Open. 2023;13(4):e069668. PubMed CrossRef
- Qelbree (viloxazine extended-release capsules). Prescribing information. In: Supernus Pharmaceuticals. Inc.; 2025. https://www.accessdata.fda.gov/drugsatfda_docs/label/2025/211964s013lbl.pdf
- Greenwood D. Animal pharmacology of viloxazine (Vivalan). J Int Med Res. 1975;3(Suppl 3):18–30.
- Findling RL, Candler SA, Nasser AF, et al. Viloxazine in the management of CNS disorders: a historical overview and current status. CNS Drugs. 2021;35(6):643–653. PubMed CrossRef
- Garcia-Olivares J, Yegla B, Earnest J, et al. Unraveling the mechanism of action of viloxazine ER in ADHD. Neuropsychopharmacology. 2023;48(1):63–210. American College of Neuropsychopharmacology Meeting abstract P175.
- Earnest J, Garcia-Olivares J, Yegla B, et al. An experimental program to determine the effects of viloxazine on cortical serotonin neurotransmission at doses relevant for ADHD treatment. Neuropsychopharmacology. 2022;47(Suppl 1):220–370. American College of Neuropsychopharmacology Annual Meeting abstract P434. PubMed
- Yu C, Garcia-Olivares J, Candler S, et al. New insights into the mechanism of action of viloxazine: serotonin and norepinephrine modulating properties. J Exp Pharmacol. 2020;12:285–300. PubMed CrossRef
- Nasser A, Hull JT, Chaturvedi SA, et al. A phase III, randomized, double-blind, placebo-controlled trial assessing the efficacy and safety of viloxazine extended-release capsules in adults with attention-deficit/hyperactivity disorder. CNS Drugs. 2022;36(8):897–915. PubMed CrossRef
- Spencer TJ, Adler LA, Meihua Q, et al. Validation of the adult ADHD Investigator Symptom Rating Scale (AISRS). J Atten Disord. 2010;14(1):57–68. PubMed
- Müller MJ, Himmerich H, Kienzle B, et al. Differentiating moderate and severe depression using the Montgomery-Asberg Depression Rating Scale (MADRS). J Affect Disord. 2003;77(3):255–260. PubMed CrossRef
- Hamilton M. The assessment of anxiety states by rating. Br J Med Psychol. 1959;32(1):50–55. PubMed CrossRef
- Guy W. ECDEU Assessment Manual for Psychopharmacology. U.S. Department of Health, Education, and Welfare, Public Health Service, Alcohol, Drug Abuse, and Mental Health Administration. National Institute of Mental Health, Psychopharmacology Research Branch, Division of Extramural Research Programs; 1976.
- Adler LA, Faraone SV, Sarocco P, et al. Establishing US norms for the Adult ADHD Self-Report Scale (ASRS-v1.1) and characterising symptom burden among adults with self-reported ADHD. Int J Clin Pract. 2019;73(1):e13260. PubMed CrossRef
- Kroenke K, Strine TW, Spitzer RL, et al. The PHQ-8 as a measure of current depression in the general population. J Affect Disord. 2009;114(1-3):163–173. PubMed CrossRef
- Spitzer RL, Kroenke K, Williams JB, et al. A brief measure for assessing generalized anxiety disorder: the GAD-7. Arch Intern Med. 2006;166(10):1092–1097. PubMed CrossRef
- Roth RM, Gioia GA. Behavior rating inventory of executive function-adult version. Lutz (FL). Psychological Assessment Resources; 2005.
- Childress A, Cutler AJ, Adler LA, et al. An open-label extension study assessing the long-term safety and efficacy of viloxazine extended-release capsules in adults with attention-deficit/hyperactivity disorder. CNS Drugs. 2024;38(11):891–907. PubMed CrossRef
- Reilly MC, Zbrozek AS, Dukes EM. The validity and reproducibility of a work productivity and activity impairment instrument. Pharmacoeconomics. 1993;4(5):353–365. PubMed CrossRef
- Buysse DJ, Reynolds CF 3rd, Monk TH, et al. The Pittsburgh Sleep Quality Index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. PubMed CrossRef
- Frank E, Prien RF, Jarrett RB, et al. Conceptualization and rationale for consensus definitions of terms in major depressive disorder. Remission, recovery, relapse, and recurrence. Arch Gen Psychiatry. 1991;48(9):851–855. PubMed CrossRef
- Steele M, Jensen PS, Quinn DM. Remission versus response as the goal of therapy in ADHD: a new standard for the field?. Clin Ther. 2006;28(11):1892–1908. PubMed CrossRef
- Lippman W, Pugsley TA. Effects of viloxazine, an antidepressant agent, on biogenic amine uptake mechanisms and related activities. Can J Physiol Pharmacol. 1976;54(4):494–509. PubMed CrossRef
- Jones RS, Roberts MH. Effects of viloxazine on cortical neurone responses to monoamines and acetylcholine [proceedings]. Br J Pharmacol. 1977;59(3):460p. PubMed
- Jones RS, Roberts MH. Potentiation of monoamine responses of denervated cells by a noradrenaline uptake inhibitor (viloxazine) [proceedings]. Br J Pharmacol. 1978;62(3):403p–404p. PubMed
- Jones RS, Roberts MH. Potentiation of responses to monoamines by antidepressants after destruction of monoamine afferents. Br J Pharmacol. 1979;65(3):501–510. PubMed CrossRef
- Wold EA, Wild CT, Cunningham KA, et al. Targeting the 5-HT2C receptor in biological context and the current state of 5-HT2C receptor ligand development. Curr Top Med Chem. 2019;19(16):1381–1398. PubMed CrossRef
- Higgins GA, Zeeb FD, Fletcher PJ. Role of impulsivity and reward in the anti-obesity actions of 5-HT(2C) receptor agonists. J Psychopharmacol. 2017;31(11):1403–1418. PubMed CrossRef
- Yegla B, Garcia-Olivares J, Zweibaum D, et al. Viloxazine increases interstitial levels of norepinephrine and serotonin in a dose dependent fashion in rat medial prefrontal cortex. Neuropsychopharmacology. 2022;47:63–219. American College of Neuropsychopharmacology Meeting abstract P167. PubMed
- Devroye C, Cathala A, Piazza PV, et al. The central serotonin(2B) receptor as a new pharmacological target for the treatment of dopamine-related neuropsychiatric disorders: rationale and current status of research. Pharmacol Ther. 2018;181:143–155. PubMed CrossRef
- Chagraoui A, Thibaut F, Skiba M, et al. 5-HT2C receptors in psychiatric disorders: a review. Prog Neuropsychopharmacol Biol Psychiatry. 2016;66:120–135. PubMed CrossRef
- Di Giovanni G, De Deurwaerdère P. New therapeutic opportunities for 5-HT2C receptor ligands in neuropsychiatric disorders. Pharmacol Ther. 2016;157:125–162. PubMed CrossRef
- Hedlund PB. The 5-HT7 receptor and disorders of the nervous system: an overview. Psychopharmacol Berl. 2009;206(3):345–354. PubMed CrossRef
- Blattner KM, Canney DJ, Pippin DA, et al. Pharmacology and therapeutic potential of the 5-HT(7) receptor. ACS Chem Neurosci. 2019;10(1):89–119. PubMed CrossRef
- Gottlieb N, Li TY, Young AH, et al. The 5-HT7 receptor system as a treatment target for mood and anxiety disorders: a systematic review. J Psychopharmacol. 2023;37(12):1167–1181. PubMed CrossRef
- Nikiforuk A. Targeting the serotonin 5-HT7 receptor in the search for treatments for CNS disorders: rationale and progress to date. CNS Drugs. 2015;29(4):265–275. PubMed CrossRef
- Cadogan CA, Ryan C, Hughes CM. Appropriate polypharmacy and medicine safety: when many is not too many. Drug Saf. 2016;39(2):109–116. PubMed CrossRef
- Jean-Louis G, Seixas AA. The value of decentralized clinical trials: inclusion, accessibility, and innovation. Science. 2024;385(6711):eadq4994. PubMed CrossRef
- Hanley DF Jr., Bernard GR, Wilkins CH, et al. Decentralized clinical trials in the trial innovation network: value, strategies, and lessons learned. J Clin Transl Sci. 2023;7(1):e170. PubMed CrossRef
This PDF is free for all visitors!




