Suicide is a leading common cause of death in the United States, and drug ingestion accounts for a substantial proportion of nonfatal suicide attempts.1,2 Although single-agent overdoses often follow relatively predictable clinical courses, this reliability diminishes in multidrug ingestions, which comprise a significant share of ingestion-related suicide attempts.1–3 The pharmacologic effects of multiple agents may combine, mask one another, or interact in ways that produce mixed or evolving toxidromes, posing significant diagnostic and management challenges.4
We describe a case of intentional overdose with diphenhydramine and extended-release dextromethorphan-guaifenesin that initially presented with anticholinergic toxicity and later evolved into serotonin toxicity, underscoring the need to anticipate sequential toxidromes in complex ingestions.
Case Report
Ms B is a 19-year-old female with a history of anxiety and major depressive disorder but no prior psychiatric history who was brought to the emergency department by ambulance due to altered mental status. On arrival, she was nonverbal and unable to follow commands. Pink powder was noted around her mouth and nose. According to her family, Ms B regularly used diphenhydramine for seasonal allergies, raising concern that the observed residue represented a recent ingestion. This suspicion was supported by her initial presentation, as she exhibited an acute anticholinergic toxidrome characterized by agitation, mydriasis, tachycardia, and hypertension. She required intubation, management with midazolam infusion and fentanyl, and a trial of physostigmine 2 mg (without clinical response). Electrocardiogram and telemetry revealed no significant abnormalities.
On the morning of hospital day 2, Ms B’s vital signs normalized, and she was successfully extubated. After a short lucid interval, she developed serotonin toxicity, marked by hyperreflexia, ocular clonus, mydriasis, diaphoresis, hypertension, tachycardia, hyperthermia, and agitation, requiring reintubation.
After improvement with parenteral benzodiazepines and extubation on hospital day 3, the patient reported ingesting large amounts of diphenhydramine and extended-release guaifenesin-dextromethorphan in a suicide attempt, later confirmed by collateral history. Her serotonin toxicity continued to resolve with supportive care. Following psychiatric evaluation and further stabilization, she identified academic and social stressors preceding the attempt and denied ongoing suicidal intent. She was discharged with outpatient follow-up.
Discussion
This case illustrates the complexity of multidrug ingestion management. Accurate history, collateral information, and coordinated input from toxicology, general medicine, intensive care, and psychiatry were critical to recognizing the evolving toxidrome and directing safe, effective treatment.
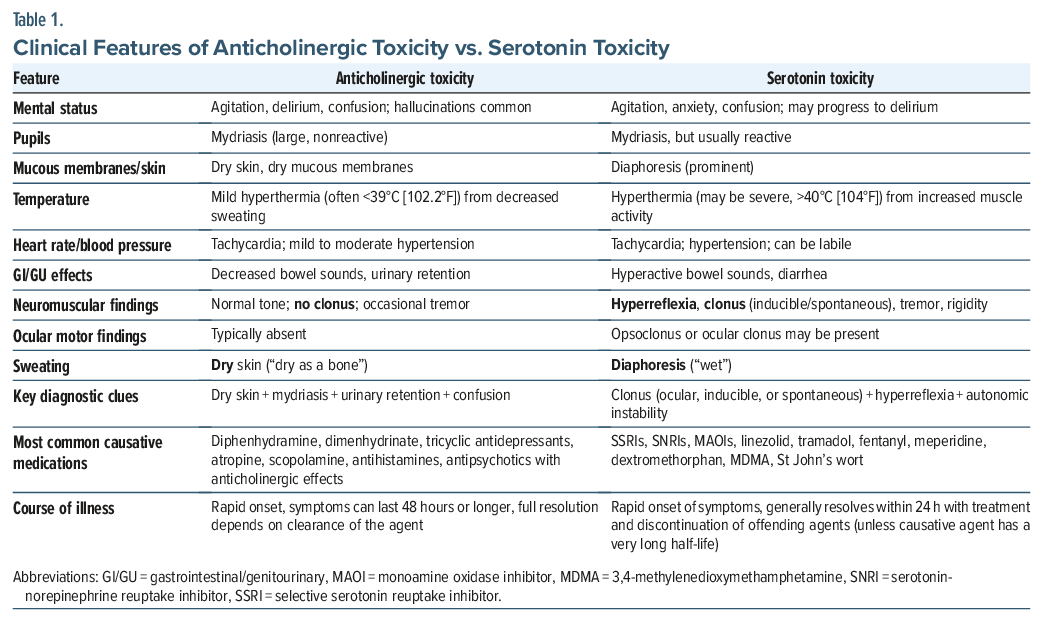
On initial presentation, anticholinergic symptoms from the diphenhydramine ingestion dominated the clinical picture. As outlined in Table 1, there may have been early signs of serotonin toxicity, though many of these overlap with anticholinergic toxicity.5,6 Because we did not have a definitive history of dextromethorphan ingestion, any contribution of serotonin toxicity to the clinical picture likely went unrecognized. Furthermore, any symptoms of either anticholinergic or serotonin toxicity would have been well-treated with benzodiazepines.6,7
Her examination findings and confirmed dextromethorphan ingestion make serotonin toxicity the most likely cause of her postextubation deterioration. The delayed presentation is best explained by slowed gastrointestinal absorption of dextromethorphan due to diphenhydramine’s anticholinergic effects.8,9 This was likely exacerbated by exposure to fentanyl, an additional serotonergic agent, administered as part of an ongoing midazolam-fentanyl infusion following intubation. The concurrent midazolam infusion may have masked symptoms of serotonin toxicity, with symptom emergence occurring after sedation was discontinued prior to extubation.7,10,11
Multidrug overdoses can produce mixed and evolving toxidromes that are difficult to recognize without careful reassessment and collateral history. This case highlights the need for vigilance in identifying sequential toxidromes, particularly when interacting agents and sedative infusions may obscure early signs. Close interdisciplinary collaboration between psychiatry, critical care, and toxicology services was key to the safe management and recovery of this patient.
Article Information
Published Online: April 28, 2026. https://doi.org/10.4088/PCC.25cr04166
© 2026 Physicians Postgraduate Press, Inc.
Prim Care Companion CNS Disord 2026;28(2):25cr04166
Submitted: December 15, 2025; accepted January 27, 2026.
To Cite: Schwartz AC, Delgado NK, Robbins-Welty GA. Mixed diphenhydramine and dextromethorphan overdose resulting in serotonin toxicity: a complex intentional ingestion case. Prim Care Companion CNS Disord 2026;28(2):25cr04166.
Author Affiliations: Department of Psychiatry and Behavioral Sciences, Emory University School of Medicine, Atlanta, Georgia (Schwartz, Delgado); Department of Family and Preventative Medicine, Division of Palliative Medicine, Emory University School of Medicine, Atlanta, Georgia (Robbins-Welty).
Corresponding Author: Ann C. Schwartz, MD, 12 Executive Park Drive, Suite 142, Atlanta, GA 30329 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Patient Consent: Consent was received from the patient to publish the case report, and information has been deidentified to protect patient anonymity.
ORCID: Ann C. Schwartz: https://orcid.org/0000-0002-5892-0833; Gregg A. Robbins-Welty: https://orcid.org/0000-0003-4516-7368
References (11)

- Wang J, Sumner SA, Simon TR, et al. Trends in the incidence and lethality of suicidal acts in the United States, 2006 to 2015. JAMA psychiatry. 2020;77(7):684–693. PubMed CrossRef
- Dutta S, Buciuc AG, Barry P, et al. A Narrative review on toxidromes in the psychiatric population: implications for overdose prevention. J Clin Med. 2025;14(17):6160. PubMed CrossRef
- Kang AM. Substances involved in suicidal poisonings in the United States. Suicide Life-Threatening Behav. 2019;49(5):1307–1317. PubMed CrossRef
- Mainoli B, Gonçalves N, Ferreira JJ, et al. Potential drug-drug interactions in acute poisonings managed in the intensive care unit: occurrence, risk factors and relationship to patient severity on admission. Basic Clin Pharmacol Toxicol. 2022;130(2):337–345. PubMed CrossRef
- Hughes AR, Lin A, Hendrickson RG. Clinical and patient characteristics associated with severe outcome in diphenhydramine toxicity. Clin Toxicol. 2021;59(10):918–925. PubMed CrossRef
- Patel J, Edwards J. Treating diphenhydramine overdose: a literature review of currently available treatment methods. Toxics. May 21, 2024;12(6):376. PubMed CrossRef
- Boyer EW, Shannon M. The serotonin syndrome. N Engl J Med. 2005;352(11):1112–1120. PubMed CrossRef
- Omoto N, Kanzawa Y, Ishimaru N, et al. Serotonin syndrome after an overdose of over-the-counter medicine containing dextromethorphan. J Gen Fam Med. 2022;23(1):38–40. PubMed CrossRef
- Parkman HP, Trate DM, Knight LC, et al. Cholinergic effects on human gastric motility. Gut. 1999;45(3):346–354. PubMed CrossRef
- Mikkelsen N, Damkier P, Pedersen SA. Serotonin syndrome—a focused review. Basic Clin Pharmacol Toxicol. 2023;133(2):124–129. PubMed CrossRef
- Badar A. Serotonin syndrome: an often-neglected medical emergency. J Fam Community Med. 2024;31(1):1–8. PubMed CrossRef
Please sign in or purchase this PDF for $40.




