Abstract
Objective: To summarize current evidence on the use of buprenorphine for chronic pain management in individuals with sickle cell disease (SCD) and identify gaps for future research.
Data Sources: PubMed, Embase, and Cochrane CENTRAL were systematically searched from database inception through August 2025 using keywords related to buprenorphine, SCD, chronic pain, and analgesia. Searches were limited to human studies published in English.
Study Selection: Seven studies were included involving pediatric or adult patients with SCD treated with buprenorphine for chronic pain. Eligible studies reported at least 1 patient-centered outcome, including pain severity, opioid utilization, health care use, or quality of life. Included study designs were case reports, case series, observational studies, and qualitative studies. Abstract-only publications and studies not specific to SCD were excluded.
Data Extraction: Two reviewers independently extracted data using the Preferred Reporting Items for Systematic Reviews and Meta-analyses Extension for Scoping Reviews guidelines, with discrepancies resolved by consensus.
Data Synthesis: A descriptive synthesis was performed. Most studies evaluated buprenorphine initiation using microinduction strategies. Buprenorphine was generally well tolerated and associated with reduced full opioid agonist use, fewer emergency department visits and hospitalizations, and improvements in functional outcomes and patient-reported autonomy. Study heterogeneity and small sample sizes limited comparative analysis.
Conclusions: Available evidence suggests that buprenorphine may be a safe and effective option for chronic pain management in SCD. Larger prospective studies with standardized induction protocols and validated outcome measures are needed to guide clinical practice.
Prim Care Companion CNS Disord 2026;28(3):25r04126
Author affiliations are listed at the end of this article.
From the Editors

Are you a healthcare provider?
Add your NPI to personalize your JCP experience.
Sickle cell disease (SCD) is the most common hereditary hematologic disorder worldwide and affects approximately 100,000 people in the United States.1 This autosomal recessive condition leads to significant morbidity and premature mortality.1–3 Acute pain crises due to vaso-occlusive episodes are the hallmark of SCD and the leading cause of hospitalization and acute care utilization.4,5 Chronic pain, defined as pain present on most days over the last 6 months in 1 or multiple locations, is a common manifestation in SCD that affects up to 40%–50% of patients.6–8 The cause of chronic pain in SCD is multifactorial and includes nociceptive, neuropathic, and central sensitization components.9
Buprenorphine, a partial μ-opioid receptor agonist with a favorable pharmacologic profile, was first approved by the US Food and Drug Administration in 1981 for the management of severe pain and later for opioid use disorder (OUD).10 Compared with full opioid agonists (FOAs), buprenorphine is associated with a lower risk for abuse and dangerous side effects.9 Its use in chronic noncancer pain, including SCD, is expanding, with evidence suggesting it may reduce morphine milligram equivalent (MME) dosing, decrease hospital utilization, and improve both pain control and functional outcomes.9,11
FOAs, such as morphine, will be needed for acute pain management in SCD. However, the role of chronic opioid therapy in SCD has mixed evidence regarding its effectiveness and the potential for adverse effects, including central sensitization, opioid-induced hyperalgesia, escalating dose requirements, and risks of diversion or misuse.7 Buprenorphine is a potential treatment alternative. The initiation or induction of buprenorphine is more complex than the use of FOAs. The objective of this scoping review was to summarize current evidence on the use of buprenorphine for chronic pain management in individuals with SCD, identify gaps for future research, and highlight the need for standardized induction protocols.
METHODS
Search Strategy
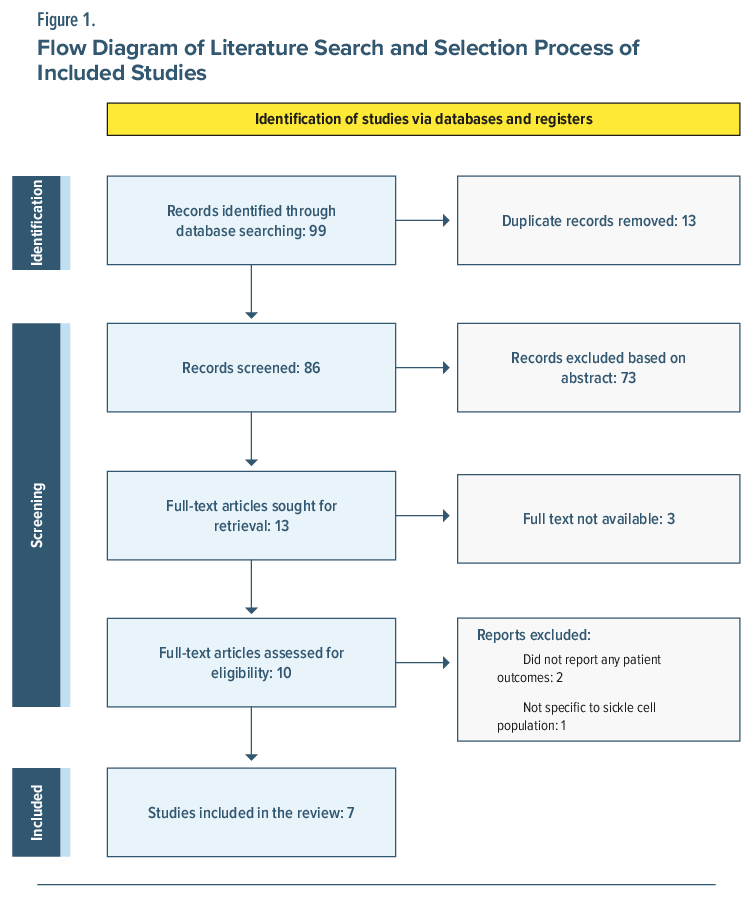
A scoping review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses Extension for Scoping Reviews guidelines (Figure 1).12 Comprehensive literature searches were conducted in PubMed, Embase, and the Cochrane Library through August 2025 to identify studies reporting the use of buprenorphine for pain management in patients with SCD. Searches combined keywords and controlled vocabulary (eg, MeSH and Emtree terms) for terms including “buprenorphine,” “sickle cell disease,” and “chronic pain” or “analgesia,” using Boolean operators to refine results. Searches were limited to studies in humans and those published in English. Grey literature was not systematically searched.
Eligibility Criteria
Studies were included if they involved patients with SCD of any age group (pediatric or adult); reported original clinical data, including case reports, case series, randomized trials, or observational studies; evaluated the use of buprenorphine for chronic pain management; or reported at least 1 patient-centered outcome, such as pain scores, opioid consumption, quality of life, or other relevant outcomes. Studies were excluded if they were not specific to buprenorphine in patients with SCD, did not report any patient-centered outcomes, or were abstracts only.
Screening Process
Titles and abstracts were independently screened by 3 reviewers (ARA, SS, and CML). The screeners then reviewed full-text articles to confirm eligibility. Discrepancies at any stage were resolved through discussion among the 3 reviewers to ensure consistency and reduce bias.
Data Extraction and Synthesis
Data were independently extracted (ARA, SS) from eligible studies, including study design, patient demographics, indication for buprenorphine, route and dose, outcomes (eg, pain scores, opioid use, quality of life), and duration of follow-up. Any discrepancies were resolved with input from the team. The extracted data were organized into summary tables, and a descriptive synthesis was performed to summarize the findings across studies. The review was registered in the Open Science Forum. Quality assessment of individual studies was not conducted, consistent with the scoping review methodology, which aims to map evidence rather than assess quality.
DISCUSSION
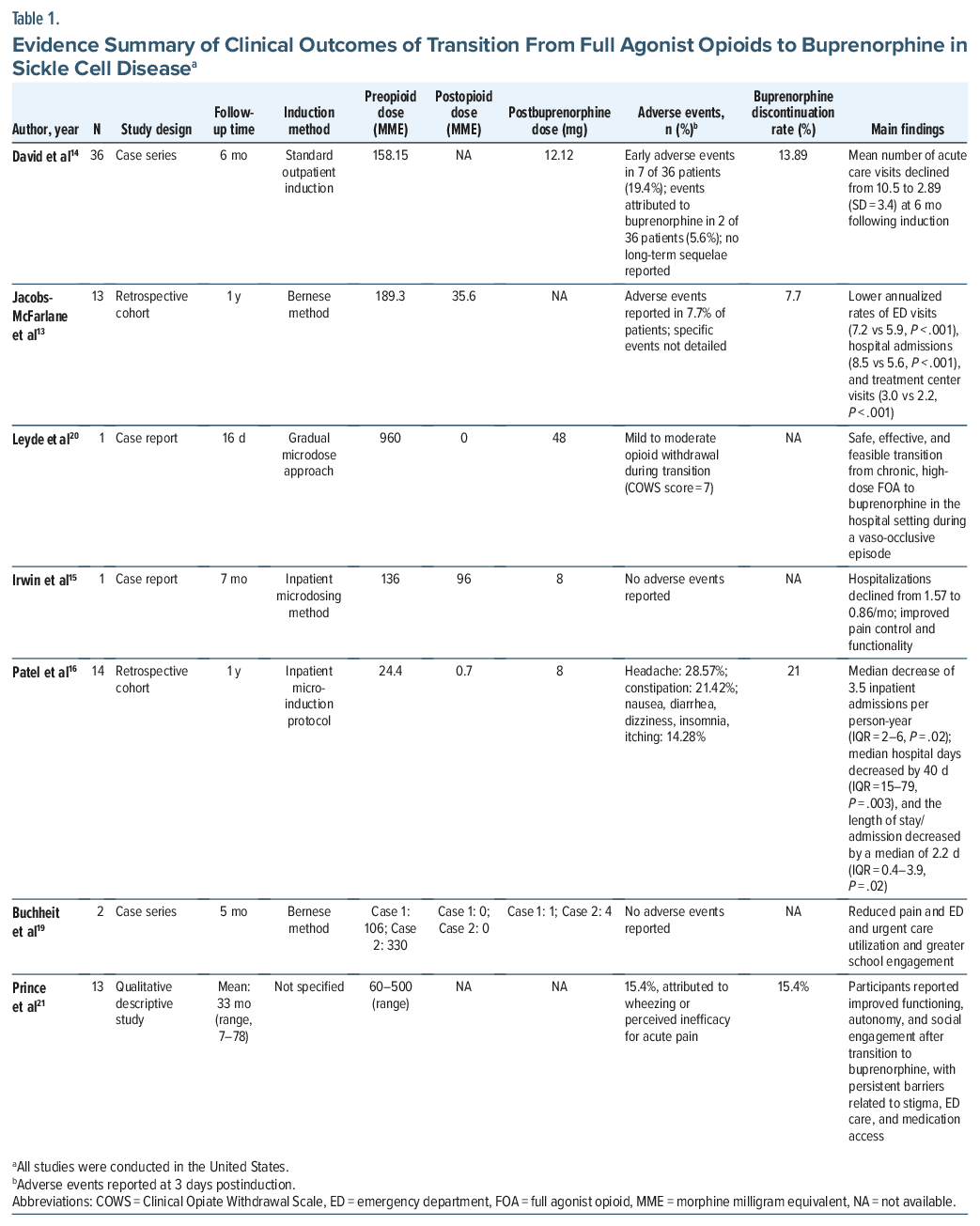
This scoping review consolidates findings from 7 different studies on the use of buprenorphine to manage pain in patients with SCD. The included studies range from case reports to larger retrospective cohorts and qualitative interviews (Table 1). Although sample sizes were small, the findings across studies were consistent. Evidence suggests that buprenorphine may be effective in reducing health care utilization,13–16 decreasing the use of FOA,13–15 and improving the overall quality of life.13–15
Induction Methods
Buprenorphine induction methods used in the included studies varied (Table 1). Historically, induction protocols for buprenorphine were designed for patients with OUD. Standard induction typically requires a period of opioid abstinence of 12–24 hours to achieve moderate withdrawal before buprenorphine initiation. Typical starting doses for OUD patients are 2 mg sublingually every 2 hours up to 4 times on the first day with rapid titration to 16–24 mg by day 3.17,18 Protocols for OUD are not appropriate for patients with SCD due to likelihood of worsening the pain.
Most of the reviewed studies used microinduction strategies rather than the standard protocol. Microinduction involves introducing very low initial doses of buprenorphine while maintaining FOA therapy, minimizing withdrawal symptoms and pain exacerbation. Jacobs-McFarlane et al13 and Buchheit et al19 employed the Bernese method, first described in 2016, which uses incremental buprenorphine microdoses overlapping with FOAs and is considered more tolerable.18 Additionally, Patel et al16 and Leyde et al20 reported the use of transdermal buprenorphine patches to deliver the very low initial doses required for microinduction. Transition to full buprenorphine therapy using these methods may take 7–10 days. All studies used the Clinical Opiate Withdrawal Scale (COWS)22 to guide dose titration, alongside shared decision-making and considered the patient perception of induction tolerability to guide dosing and symptom relief.
Reduction in Health Care Utilization
Across the included studies, buprenorphine use was consistently associated with a substantial reduction in health care utilization. David et al14 reported that, among 36 patients, the mean number of acute care visits declined from 10.5 to 2.89 over a 6-month period. Similarly, Jacobs-McFarlane et al13 demonstrated reductions in emergency department visits (7.2 to 5.9 per year, P < .001), hospital admissions (8.5 to 5.6 per year, P < .01), and treatment center visits (3.0 to 2.2 per year, P < .001). Patel et al confirmed these outcomes in adolescents, showing a decrease in annual health care encounters from 11 to 8 (P = .02), a reduction of 40 hospital days per year (P = .003), and a shortened average length of stay of 2.2 days (P = .02).16
Reduction in Opioid Utilization
One of the main benefits of buprenorphine is its ability to reduce reliance on FOA, thereby lowering the risks associated with long-term opioid therapy. Two retrospective cohorts demonstrated significant reductions in mean daily opioid utilization: from 189.3 to 35.6 MME/day (P < .001) in Jacobs-McFarlane et al13 and from 24.4 to 0.7 MME/day (P = .002) in Patel et al.16 Evidence from case reports further supports these findings; Leyde et al20 documented a successful transition from daily high-dose oxycodone use, while Irwin et al15 and Buchheit et al19 described their experience with adolescents who required lower opioid doses after buprenorphine induction. Taken together, these findings highlight buprenorphine’s potential to reduce dependence on FOA.
Quality of Life and Functional Outcomes
Beyond reducing FOA doses and health care utilization, buprenorphine contributes to improvements in patient quality of life. In a qualitative study of 13 patients with SCD who received buprenorphine for a mean of 33 months, participants reported enhanced autonomy, stronger social relationships, and improved daily functioning.22 In pediatric patients, Irwin et al15 observed that, despite high pain scores, they were able to engage more effectively in school and family activities. Similarly, Buchheit et al19 noted that outpatient buprenorphine treatment allowed adolescents to maintain engagement in academic and work-related activities.
Adverse Events, Discontinuation Rates, and Safety
The transition to buprenorphine was well tolerated and introduced safely across diverse populations (Table 1). The adverse events reported were mild and consistent with those commonly observed with opioid therapy.23 The most frequent adverse events reported by Patel et al16 were headaches (28.1%) and constipation (21.42%). In the cohort described by David et al,14 7 early adverse events were reported among 36 patients. Two of these events were directly attributed to buprenorphine, but none resulted in long-term complications. Leyde et al20 documented only mild to moderate withdrawal (COWS score of 7) during conversion from oxycodone to buprenorphine, while Buchheit et al19 reported no clinically significant withdrawal during outpatient microinduction in adolescents. Shared decision-making, adjunctive medical treatment, and mind-body interventions were consistently noted as crucial to transition to buprenorphine.
Across the included studies, buprenorphine discontinuation rates ranged from 7.7% to 21%.13,16 These rates are higher than those reported in larger studies, likely reflecting the influence of small sample sizes.23 Discontinuation was most often attributed to patient preference, limited analgesic efficacy, or following an acute pain episode. David et al reported discontinuation in 2 patients in response to adverse events.14 These findings indicate that buprenorphine was not universally tolerated or effective and underscores the need for enhanced patient education prior to induction.
Limitations
This scoping review has several limitations. All included studies were conducted in the United States, which limits generalizability, particularly to regions with a higher prevalence of SCD or different health care systems. The review was also restricted to English-language publications, potentially excluding relevant data from other sources. Most available studies had small sample sizes. The heterogeneity in reporting further complicates interpretation: some studies emphasized quantitative outcomes such as reductions in opioid use, whereas others highlighted patient-reported experiences related to stigma or autonomy.
Future Directions
To better define the role of buprenorphine for chronic pain management in SCD, future research should initially focus on expanding to larger multicenter cohort studies to establish safety and feasibility, followed by randomized controlled trials comparing buprenorphine with care as usual. These studies should assess clinical outcomes and quality of life measures. Studies in countries with the highest SCD burden will need to address drug accessibility, local regulations, and adaptation of protocols to diverse health care settings.
Standardization of induction protocols is needed. Research should identify strategies that minimize withdrawal symptoms, improve treatment retention, and can be adapted across different clinical settings.
Future work should not overlook patient-centered outcomes. Early qualitative data suggest patients value autonomy, reduced stigma, and quality of life as top priorities. Mixed-methods studies that value patient wishes along with clinical outcomes will ensure that treatment is appropriate. Finally, buprenorphine should be evaluated within multimodal frameworks that integrate nonpharmacologic interventions.
CONCLUSION
Buprenorphine is a promising, practical, and safe option for pain management in patients with SCD. Reported benefits include lower health care visits, reduced opioid requirements, and enhanced daily functioning and quality of life. Notably, utility has been demonstrated across populations, including children and adolescents and individuals with treatment-resistant pain. Side effects were mild, and microdosing strategies, such as the Bernese method, have been shown to reduce the risk of withdrawal during induction. Overall, buprenorphine should be considered as a valuable tool in a patient-focused approach to SCD-related pain management. Larger studies with thoughtful designs incorporating themes discussed here should be undertaken to further delineate the role of buprenorphine in clinical practice.
Article Information
Published Online: June 16, 2026. https://doi.org/10.4088/PCC.25r04126
© 2026 Physicians Postgraduate Press, Inc.
Submitted: October 30, 2025; accepted January 6, 2026.
To Cite: Singh S, Akbari AR, Marín-López C, et al. Buprenorphine for chronic pain management in sickle cell disease: a scoping review of current evidence. Prim Care Companion CNS Disord 2026;28(3):25r04126.
Author Affiliations: Department of Psychiatry, Division Of Addiction Psychiatry, University of Kansas Medical Center, Kansas City, Kansas (Singh, Perchellet, Sethi); Department of Internal Medicine, University of Kansas Medical Center, Kansas City, Kansas (Akbari, Marín-López).
Corresponding Author: Roopa Sethi, MD, Department of Addiction Psychiatry, University of Kansas Medical Center, Kansas City, KS 66160 ([email protected]).
Financial Disclosure: None.
Funding/Support: None.
Previous Presentation: Poster presented at the Kansas Chapter of the American College of Physicians; Wichita, Kansas; October 16–17, 2025.
Clinical Points
- Evidence from case reports, case series, and retrospective cohorts suggests that buprenorphine can be used safely for chronic pain management in patients with sickle cell disease and is associated with reduced emergency department visits, hospital admissions, and opioid use and improved functional outcomes.
- Microinduction approaches, including the Bernese method and transdermal buprenorphine initiation, were the most used strategies in published studies and allowed patients to transition from full opioid agonists without opioid abstinence, withdrawal, or worsening pain.
- Patient-centered approaches, including shared decision-making and education about induction expectations, are critical to successful treatment, as barriers identified in the literature include concerns about analgesic efficacy, induction complexity, and stigma associated with buprenorphine use.
References (23)

- Kavanagh PL, Fasipe TA, Wun T. Sickle cell disease: a review. JAMA. 2022;328(1):57–68. PubMed
- Kato GJ, Piel FB, Reid CD, et al. Sickle cell disease. Nat Rev Dis Primers. 2018;4(1):1–22. PubMed
- Martinez RM, Osei-Anto HA, McCormick M, eds. National Academies of Sciences, Engineering, and Medicine; Health and Medicine Division; Board on Population Health and Public Health Practice; Committee on Addressing Sickle Cell Disease: A Strategic Plan and Blueprint for Action. National Academies Press; 2020.
- Brousseau DC, Owens PL, Mosso AL, et al. Acute care utilization and rehospitalizations for sickle cell disease. JAMA. 2010;303(13):1288–1294. PubMed
- Ballas SK, Gupta K, Adams-Graves P. Sickle cell pain: a critical reappraisal. Blood. 2012;120(18):3647–3656. PubMed
- Smith WR, Penberthy LT, Bovbjerg VE, et al. Daily assessment of pain in adults with sickle cell disease. Ann Intern Med. 2008;148(2):94–101. PubMed CrossRef
- Brandow AM, Carroll CP, Creary S, et al. American Society of Hematology 2020 guidelines for sickle cell disease: management of acute and chronic pain. Blood Adv. 2020;4(12):2656–2701. PubMed CrossRef
- Dampier C, Palermo TM, Darbari DS, et al. AAPT diagnostic criteria for chronic sickle cell disease pain. J Pain. 2017;18(5):490–498. PubMed
- Dalal S, Chitneni A, Berger AA, et al. Buprenorphine for chronic pain: a safer alternative to traditional opioids. Health Psychol Res. 2021;9(1):27241. PubMed CrossRef
- US Drug Enforcement Administration. Diversion control division, drug & chemical evaluation section. Buprenorphine. 2025. Accessed September 9, 2025. https://deadiversion.usdoj.gov/drug_chem_info/buprenorphine.pdf
- Webster L, Gudin J, Raffa RB, et al. Understanding buprenorphine for use in chronic pain: expert opinion. Pain Med. 2020;21(4):714–723. PubMed
- Tricco AC, Lillie E, Zarin W, et al. PRISMA extension for scoping reviews (PRISMA-ScR): checklist and explanation. Ann Intern Med. 2018;169(7):467–473. PubMed CrossRef
- Jacobs-McFarlane C, Liu A, McCrary B, et al. Buprenorphine is associated with lower home opioid use and acute care utilization in sickle cell disease. Pain Manag Nurs. 2025. ;[Epub ahead of print].
- David MS, Jones J, Lauriello A, et al. Converting adults with sickle cell disease from full agonist opioids to buprenorphine: a reliable method with safety and early evidence of reduced acute care utilization. Am J Hematol. 2022;97(11):1435–1442. PubMed CrossRef
- Irwin M, Gunther W, Keefer P, et al. Buprenorphine for chronic pain in a pediatric patient with sickle-cell disease. J Pain Symptom Manage. 2021;62(5):1086–1091. PubMed CrossRef
- Patel A, Kalmus G, Dampier C, et al. Treatment experience using a microinduction buprenorphine protocol for chronic pain in pediatric sickle cell disease. Pediatr Blood Cancer. 2025;72(8):e31731. PubMed CrossRef
- Ahmed S, Bhivandkar S, Lonergan BB, et al. Microinduction of buprenorphine/naloxone: a review of the literature. Am J Addict. 2021;30(4):305–315. PubMed CrossRef
- Hämmig R, Kemter A, Strasser J, et al. Use of microdoses for induction of buprenorphine treatment with overlapping full opioid agonist use: the Bernese method. Subst Abuse Rehabil. 2016;7:99–105. PubMed CrossRef
- Buchheit BM, Joslin T, Turner HN, et al. Ambulatory microdose induction of buprenorphine-naloxone in two adolescent patients with sickle cell disease. Pediatr Blood Cancer. 2021;68(1):e28766. PubMed CrossRef
- Leyde S, Suen L, Pratt L, et al. Transition from oxycodone to buprenorphine/ naloxone in a hospitalized patient with sickle cell disease: a case report. J Gen Intern Med. 2022;37(5):1281–1285. PubMed CrossRef
- Prince E, Loeser P, Early M, et al. “Buprenorphine, it works so differently”: adults with sickle cell disease describe transitioning to buprenorphine for treatment of chronic pain. J Pain. 2024;25(3):632–641. PubMed CrossRef
- Wesson DR, Ling W. The Clinical Opiate Withdrawal Scale (COWS). J Psychoactive Drugs. 2003;35(2):253–259. PubMed
- Powell VD, Rosenberg JM, Yaganti A, et al. Evaluation of buprenorphine rotation in patients receiving long-term opioids for chronic pain: a systematic review. JAMA Netw Open. 2021;4(9):e2124152. PubMed CrossRef
This PDF is free for all visitors!




